Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
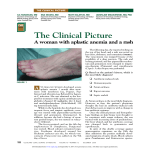
Serum Sickness Jill Tichy, M.D. PGY III Serum Sickness What is it? Immunization of host (human) by heterologous (non-human) serum proteins caused by formation of immune complexes A diagnosis made clinically and one of exclusion Definition continued… Cardinal symptoms include rash, fever, polyarthralgias or polyarthritis Malaise Occurs one to two weeks after first exposure to responsible agent Resolves within a few weeks of discontinuing the drug Type III or Immune Complex Mediated Hypersensitivity Antigens combine with host immunoglobulins specific to those antigens Resultant immune complexes are in excess of phagocyte system Deposit in tissues and trigger the inflammatory response Blame the heterologous proteins Equine or Rabbit Antithymocyte Globulin (ATG) Rituximab Inflimixab Venom Anti-toxins Rabies Vaccine Streptokinase Penicillin Cefaclor Amoxicillin Bactrim Supportive Physical Exam Findings Pruritic Rash sparing the mucous membranes Rash can be serpiginous and macular which starts at the trunk and spreads distally *Skin changes at the junction of the lateral aspect of palms and soles Supportive Physical Exam Findings Supportive Physical Exam Findings Joints commonly involved are: MCP, knees, wrists, ankles and shoulders Spine and TMJ involvement is also reported Joint pain typically occurs after rash has started Myalgias also seen Trismus Supportive Laboratory Data Neutropenia with reactive lymphocytes Mild Thrombocytopenia Eosinophilia Elevated CRP and ESR Proteinuria (50% of patients) Elevations in creatinine Supportive Laboratory Data Dermatopathology Histology varies Typical is mild peri-vascular infiltrates with lymphocytes and histiocytes without vessel necrosis Differential Diagnosis Acute Rheumatic Fever Disseminated gonococcemia and meningococcemia Reactive Arthritis (Reiter’s Syndrome) Rickettsial Diseases Disseminated EBV/CMV Stevens-Johnson Syndrome Still’s Disease Kawasaki’s Disease Viral Exanthems Treatment Stop offending agent Mild symptoms self-limiting Anti-histamines; NSAIDs Severe symptoms (fever > 38.5; extensive rash, severe arthritis) give steroids Avoid responsible drug in the future Not clear if similar drugs should be avoided References Lawley, TJ, Bielory, L, Gascon, P, et al. A prospective clinical and immunologic analysis of patients with serum sickness. N Engl J Med 1984; 311:1407 Bielory, L, Yancey, KB, Young, NS, et al. Cutaneous Manifestations of serum sickness in patients receiving antithymocyte globulin. J AM Acad Dermatol 1985; 13:411 Snow, M, Cannella, A, Stevens, RB, Presumptive Serum Sickness as a Complication of Rabbit-Derived Antithymocyte Globulin Immunosuppression Harrison’s Textbook of Internal Medicine Uptodate photography