Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
ANTIARRHYTHMIC DRUGS
Every hour
2000 patients around the world
die from sudden arrhythmia
attack
CARDIAC ARRHYTHMIAS, LOCAL CAUSES
CARDIAC
ARRHYTHMIAS
SYSTEMIC
CAUSES
Extrasystolia, scintillating arrhythmia,
paroxysmal tachycardia, fibrillation
Causes
Mechanisms
Surplus of catecholamines
(thyreotoxicosis)
Increasing of frequency of
spontaneous diastolic
depolarization (calcium type) in
Р-cells of sinus node
Disturbance of ion balance
Development of sodium ("fast")
(hypopotassiumemia,
type of spontaneous
hypomagnesiumemia), ischemia, depolarization in elements of
hypoxia of myocardium,
conductive system of the heart
intoxication (cardiac glycosides) which don’t have automatism in
normal conditions
Insufficient power of potential
Manifestation of activity of
which exits from sinus node
heterotopous source of impulse
development
Disturbance of conductivity
Local circulation of impulses
(re-entry mechanism)
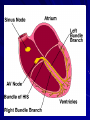
Scheme of mechanism of repeated entry
norm
Nervous
impulse
Wall of the ventricles
One-side
blockade
2
1
Impulse goes in reverse direction
and enters the starting point
(circulation of the impulse),
which leads to out of order and
non regular contraction of the heart
Arrhythmia riskier in athletes
Cardiac problems like
an abnormal
heartbeat are
exacerbated by
rigorous exercise in a
way that can be fatal
in athletes, and
regular testing for the
problem could save
lives
Drugs can provoke arrhythmias
(arrhythmogenic action)
All antiarrhythmics
except betaadrenoblockers
Antidepressants
Adrenomimetics
Some antiallergics
(terfenadine=telfast)
Supra ventricular tachyarrhythmias
VENTRICULAR ARRHYTHMIAS
Classification of antiarrhythmic drugs accordingly
to Williams and Harrison (1970, 1981)
Class
I
Mechanism of action
Membrane
blockers
stabilizing,
sodium
Drugs
canals
IА
Slow down Na+ ions entry into cells Chinidine,
moderately (0-phase of action potential), disopyramid,
considerably prolong (during phase 3) primalin etc.
action potential and repolarization
duration
IB
Weakly influence on Na+ ions entry, Lidocain,
trimecain,
shorten repolarization duration and action tokainid, difenin
potential
IС
Considerably depress Na+ ions entry but Flecainid,
encainid,
ethmosin,
almost don’t influence on repolarization ethacisin, alapinin, propaphenon
period and action potential duration
II
Beta-adrenergic receptors blockers
III
Prolong
repolarization
and
action Amiodaron, brethylium,
potential (potassium canals blockers)
nibentan etc.
IV
Calcium canals blockers
Verapamil,
bepridil
5th
Bradycardiaс agents
Alinidin
6th
Purinergic receptors stimulants
Adenosine, ATP
novocainamid,
aimalin, imipramin,
mexyletin,
Anaprilin, nadolol, esmolol, atenolol,
methoprolol, bisoprolol
galopamil,
d-sotalol,
dilthiazem,
Indications for using Chinidine sulfate (I-А class)
Stabile form of
scintillating
arrhythmia
Ventricular extrasystolia and
tachycardia (rarely)
Stopping of
scintillating arrhythmia
paroxysms
Supporting of normal
rhythm after cardio version
(electro-impulse therapy)
Complications
оf chinidine sulfate
1. Sinus bradycardia
2. Cardiac insufficiency
3. Pirouette tachycardia (“torsade de points” polymorphic ventricular tachycardia)
4. Thromboembolia
5. Hypotension
6. Nausea, vomiting
7. Ringing in ears, hearing disorders
8. Eyesight (vision) disorders
9. Skin rash
10. Agranulocytosis (bone marrow suppression)
11. Hepatitis etc.
Indications for administration of
Novocain amid (I-А class)
1. Paroxysms of scintillating arrhythmia (in a
case when verapamilum and ATP are
ineffective)
2. Fibrillation of atria
3. Prophylaxis and treatment of paroxysmal
ventricular tachycardia, extrasystolia
Complications of novocainamid
• Allergic reactions (cross-allergic reactions with other
drugs of PABA structure)
• Nausea, vomiting
• Insomnia, headache
• Seizures
•Arterial hypotension
• Disorders of conductivity and contractility of
myocardium
• Arrhythmogenic action
• Leukopenia, agranulocytosis
• Symptoms of system lupus
Pulsnorma (aimalin)
(I-А class)
Indications for
administration
Lidocain (I В class)
It is a drug of choice in case of heavy ventricular
arrhythmias (extrasystolia, paroxysmal tachycardia,
fibrillation) of different origin, including acute
myocardial infarction (0,2 % sol. i. v. very slowly)
Difenin (I В class)
To treat tachyarrhythmias caused by intoxication with
cardiac glycosides
Antiarrhythmic drugs of І С class
ethmosin
Atrial and ventricular
paroxysmal tachycardia,
extrasystolia
ethacysin
Ventricular
tachyarrhythmias
Nowadays it is recommended to limit administration of
1 C class drugs using only for the most life threatening
ventricular arrhythmias with considerable clinical
symptoms
IС class
-adrenoblockers (II class)
(anaprilin, atenolol, methoprolol)
Administration:
sinus
tachycardia
(for
thyrotoxicosis),
supraventricular
extrasystolia,
paroxysmal tachycardia, including acute myocardial
infarction
Contraindications: bronchial asthma,
mellitus,
diseases
of
peripheral
atrioventricular blockade
diabetes
vessels,
Anaprilin
Atenolol
Vasocardin (Methoprolol tartrate)
Potassium canals blockers (III class)
(amiodaron, brethylium, sotalol)
Usage: atrial and ventricular tachyarrhythmias
Amiodaron
drug of choice in case of
paroxysmal scintillating
arrhythmia and malignant
ventricular disorders of rhythm
Amiodaron
Scheme of amiodaron administration
І - Saturation period (1,5-2 weeks):
200 mg 2-3 times daily
ІІ – Supporting therapy:
200 mg daily 5 days, 2-days brake, after
- a certain period of time accordingly to
this scheme
Arrhythmil (amiodaron)
Amiodaron
Amiodaron induced
skin discoloration
Amiodaron induced pulmonary infiltrates
Calcium canals blockers (IV class)
(verapamil, dilthiazem)
Administration
supraventricular tachyarrhythmias
(paroxysmal tachycardia, extrasystolia,
scintillating arrhythmia)
Finoptin (verapamil)
Verapamilum
Combination of verapamilum and digoxinum
can cause acute digoxine intoxication (they
compete for binding with plasma proteins)
I.v. verapamile introduction on the basis of
β-adrenoblockers administration can provoke
severe bradycardia, heart blockade and acute
hypotension
ADENOSINTRIPHOSPHATE (ATP)
Administration – supraventricular arrhythmias
(i. v. by bolus)
Complications
ATP introduction after β-adrenoblockers
can provoke syno-atrial node depression and
even cardiac arrest
When vasospastic type of IHD – ATP
introduction can lead to severe angina attack
Specific antagonist of ATP - theophylline
Choice of antiarrhythmic agent depending on kind of
tachyarrhythmia
• supraventricular tachyarrhythmias – verapamil,
beta-adrenoblockers, cardiac glycosides
• ventricular
tachyarrhythmias
–
lidocain,
trimecain, mexyletin, phenitoin (diphenin),
ornide, flecainid, rhythmilen
• effective in both cases - for supraventricular and
ventricular tachyarrhythmias – chinidine,
novocainamid, ethmosyn, ethacysyn, amiodaron,
sothalol, potassium preparates
Administration of antiarrhythmic drugs
due to life-threatening indications
1. frequent and polytopic extrasystoles –
manifestations of possible fibrillation
2. constant and paroxysmal ventricular
tachycardia
3. fibrillation of ventricles
4. atrial rhythm disorders, if accompanied by
considerable haemodynamic disorders
!This arrhythmia is accompanied by multiple
ectopic seats of impulses in atria, which leads to
increasing of frequency of ventricular
contractions (100-150 beats per minute), which
becomes irregular
Administration of antiarrhythmic drugs
Antiarrhythmic drugs
Type of
arrhythmia
Atrium
arrhythmia
Scintillation
of atria
Fibrillation
of atria
Class I
Class II
chinidine
anaprilin
chinidine
anaprilin
Class III
Class IV
others
verapamil
digoxin
Beta-blockers – are the drugs of choice
in case of atria fibrillation.
Long lasting administration of
anticoagulants in small doses decreases
risk of stroke associated with
fibrillation of atria
anticoagulant
therapy
amiodaron
Supraventricular
tachycardias
Mechanism of
reentry
anaprilin
Acute
supraventricular
tachycardia
verapamil
digoxin
verapamil
adenosine
Ventricular
tachycardias
Acute
ventricular
tachycardia
Fibrillation of
ventricles
(the previous
defibrillation is
not effective)
lidocain
Sotalol,
amiodaron
lidocain
brethylium,
amiodaron
This arrhythmia is an often cause of death
of patinets with myocardium infarction.
It can be quickly transformed into fibrillation
of ventricles. It needs an immediate treatment.
The most widely used drug
The alternative drug
adrenalin
CONDUCTION OF IMPULSE
THROUGH ATRIO-VENTRICULAR
NODE CAN BE SLOWED DOWN
BY:
ANAPRILIN,
VERAPAMIL,
DIGOXIN
Influence of prolonged administration of antiarrhythmic drugs on
mortality
(results of placebo-controlled multicenter randomized trials)
mortality increasing
mortality decreasing
Can possibly decrease
mortality (modern data is
not convincing)
encainid
flecainid
moracisin
beta-adrenoblockers
amiodaron
dysopyramid
mexylethyn
novocainamid
propaphenon
chinidine
sotalol
?
MANAGEMENT of ATRIOVENTRICULAR
BLOCKADE
M-cholinoblockers (atropine)
β-adrenomimetics (isadrine)
Glucagon
Calcium preparations
diphenylhydantoin