Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
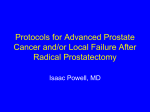
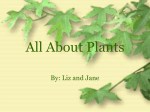
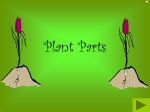
Radiotherapy - the art of the invisible Terry Kehoe Consultant Clinical Scientist Head of Oncology Physics Edinburgh Cancer Centre “How to crack a walnut” CRUK - Radio 5 on 10th June 2014 50% survive 5yrs today 30yrs ago – 25% 20yr target – 75% CRUK - TI report May 2014 Addition of RT – 16% ↑ in 5yr survival Addition of CT – 2% ↑ in 5yr survival Why does so much money go into drug development? Improved survival from prostate cancer over my career 46.7% -5yr survival in the early 80’s By the end of the 80’s 5yr survival ↑ 56.3%. By mid 90’s 5yr survival ↑ to 70%. Mid ‘00‘s - 5yr survival ↑ to 85.2% When I started in 1979 We increased our doses safely – how? Early Image Guided Radiotherapy IGRT 2004 Fiducial Markers Inserted trans rectally Images true prostate position We increased our doses safely – how? Diagnostic quality imaging Modern Image Guided Radiotherapy IGRT 2009 Same Fiducial Markers Now CT capability Images true prostate position and software calculates how much to move the field to correct for it Why we can increase our doses safely New in 2011 even better IMRT Will have all LinAcs with this arc therapy by end of 2015 IMRT 5½mins VMAT 1½mins ~ Doubling in 5yr survival in 3½ decades All from RT? No - 46% of prostate cancer patients receive external beam radiotherapy. Will the 85.2% 5yr survival rise? Probably. How do you know you are doing it right? Image Guided – IMRT is best. Is it new? No it’s been around for a century. Some people call it a “black art” perhaps its “magic” I-125 day case permanent implant Volume Study 2001 Classic 2-stage procedure Volume study to assess prostate size, pubic arch problems and plan treatment Good for learning curve Single stop intraoperative prostate Seeds Brachytherapy ECC late 2009 HDR temporary implant Meta-analysis of large patient studies Using % PSA progression free as an indication of survival Criteria for Inclusion of Article* 1 Patients should be separated into Low, Intermediate, and High Risk 2 Success must be determined by PSA analysis 3 All Treatment types considered 4 Article must be in a Peer Reviewed Journal 5. Low & Intermediate Risk articles must have a min of 100 patients 6. High Risk articles, because of fewer patients, need only 50 patients to meet criteria 7. Patients must have been followed for a median of 5 years * Expert panel consensus LOW RISK RESULTS Weighted Brachy % PSA Progression Free Treatment Success 100 23 25 4 22 30 6 EBRT 37 31 90 19 105 24 14 21 13 8 35 3 33 29 101 39103 18 102 38 40 1 100 27 32 10 28 36 2 26 EBRT & Seeds 5 16 12 7 104 9 80 15 Surgery 70 34 ← Years from Treatment → 60 11 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Robot RP Seeds Surgery EBRT CRYO HIFU Protons HDR INTERMEDIATE RISK RESULTS % PSA Progression Free Treatment Success Weighted EBRT & Seeds Brachy 100 33 14 90 24 2313 35 16 4 30 36 45 40 38 32 43 18 47 19 5 7 42 3 28 9 26 25 29 41 1 8 10 11 60 EBRT 20 Hypo EBRT 17 27 2 46 Surgery 50 ← Years from Treatment → 40 2 3 4 5 6 21 7 8 Brachy Seeds Alone Surgery EBRT CRYO HIFU HDR EBRT, Seeds + ADT 22 1 Seeds + ADT EBRT & Seeds 39 6 12 70 + 34 15 44 80 Robot RP 37 9 10 11 12 13 14 15 Protons HIGH RISK RESULTS Weighted % PSA Progression Free Treatment Success EBRT, Seeds & ADT 20 Brachy 16 109 45 19 18 4 38 22 100 108 EBRT & ADT 17 EBRT & Seeds 40 3 34 9 41 13 36 25 101 106 EBRT 44 48 1 33 21 43 32 2 10 12 14 46 42 8 110 31 28 104 24 5 Surgery 30 27 107 102 15 105 Protons HDR 23 29 ← Years from Treatment → Hypo EBRT 39 11 7 6 26 103 35 37 47 49 EBRT Seeds + ADT Robot RP Thank you for listening What other radiotherapy improvements will increase 5yr survival? • SABR – similar to VMAT but 5 visits only • Better planning including radiobiological systems • Better on-board imaging & faster delivery • Ability to adapt treatment while on the couch •Better knowledge of impact • Physically – transit dosimetry • Biologically – chip on a pill New imaging Robotic delivery Protons HIFU CRYO Photodynamic “Nanoknife”