Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmaceutical industry wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Adherence (medicine) wikipedia , lookup
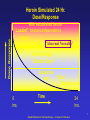
Medication Assisted Treatment (MAT) in Pregnant Women Susan F. Neshin, M.D. Medical Director JSAS Healthcare, Inc. Asbury Park, NJ E-mail: [email protected] Overview of Presentation • • • • • • • What is MAT? Rationale for MAT Importance of Dose Adequacy Impact of MAT The Medications Women’s Issues/PREGNANCY Addressing Stigma What is MAT? • MAT=Medication Assisted Treatment in context of substance abuse treatment • EUPHEMISM for opioid maintenance therapy – Methadone – Buprenorphine • Broaden definition – Naltrexone – Medication for other drug dependencies – Medication in the treatment of chronic disease Medications Development Division • Branch of National Institute on Drug Abuse (NIDA) • Developing new medications • Addiction as a brain disease • Drug craving as a physiologic phenomenon Rationale for MAT/OMT For Chronic Opioid Dependence • Dole’s concept of metabolic derangement • Current concept of neuronal adaptations to repeated exposures of the drug • Pre-existing vulnerability and/or consequence of opioid use • Corrective, not curative On/Off - Non-Tolerant Drug States Overdose “ON” Intoxication Drug Effect Euphoria “OFF” No Drug Effect; “Normophoria” “Normal” Dysphoria Opioid Maintenance Pharmacotherapy - A Course for Clinicians 6 Dose Response Heroin Simulated 24 Hr. Dose/Response With established heroin “Loaded” tolerance/dependence “High” “Abnormal Normality” Normal Range “Comfort Zone” Subjective “Sick” w/d Objective w/d 0 hrs. Time 24 hrs. 7 Opioid Maintenance Pharmacotherapy - A Course for Clinicians Dose Response Methadone Simulated 24 Hr. Dose/Response At steady-state in tolerant patient “Loaded” “High” “Abnormal Normality” Normal Range “Comfort Zone” Subjective “Sick” w/d Objective w/d 0 hrs. Time 24 hrs. 8 Opioid Maintenance Pharmacotherapy - A Course for Clinicians Goals for Pharmacotherapy • Prevention or reduction of withdrawal symptoms • Prevention or reduction of drug craving • Prevention of relapse to use of addictive drug • Restoration to or toward normalcy of any physiological function disrupted by drug addiction Importance of Dose Adequacy! Recent Heroin Use by Current Methadone Dose 120 100 80 60 40 20 0 0 10 20 30 40 50 60 70 Current Methadone Dose mg/day J. C. Ball, November 18, 1988 80 90 100 Retention in Treatment Relative to Dose 80 + mg 60-79 mg < 60 mg 0 20 40 60 80 100 Adapted from Caplehorn & Bell - The Medical Journal of Australia Impact of Maintenance Treatment • Reduction death rates (Grondblah, ‘90) • Reduction IVDU (Ball & Ross, ‘91) • Reduction crime days (Ball & Ross) • Reduction rate of HIV seroconversion (Bourne, ‘88; Novick ‘90,; Metzger ‘93) • Reduction relapse to IVDU (Ball & Ross) • Improved employment, health, & social function DEATH RATES IN TREATED AND UNTREATED HEROIN ADDICTS 8 7 6 5 OBSERVED EXPECTED 4 3 2 1 0 MMT VOL DC TX INVOL DC TX UNTREATED Slide data courtesy of Frank Vocci, MD, NIDA - Reference: Grondblah, L. et al. ACTA PSCHIATR SCAND, P. 223-227, 1990 14 Impact of MMT on IV Drug Use for 388 Male MMT Patients in 6 Programs ADMISSION 100 * * 0 Pre| 1st Year Year Admission | 2nd Year | 3rd Year Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991 | 4th Crime among 491 patients before and during MMT at 6 programs Crime Days Per Year 300 250 200 Before TX During TX 150 100 50 0 A B C D E F Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991 HIV CONVERSION IN TREATMENT 25% 20% 15% Tx Status 10% 5% 0% In Tx (N=95) Partial Tx (N=45) No Tx (N=55) 18 month HIV conversion by treatment retention Source: Metzger, D. et. al. J of AIDS 6:1993. p.1053 OMT as Treatment of Choice for Chronic Relapsing Opioid Addict • Concept of “prolonged abstinence” – Hyper-reactivity to stress – Dysphoria/craving increase vulnerability to relapse Relapse to IV drug use after MMT 105 male patients who left treatment 100 82.1 Percent IV Users 80 72.2 60 57.6 45.5 40 28.9 20 0 IN 1 to 3 Treatment 4 to 6 7 to 9 10 to 12 Months Since Stopping Treatment Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991 The Medications • Methadone – Long-acting full opioid agonist – Orally effective – Can be taken once a day – Prescribed and dispensed at licensed OTPs The Medications • Buprenorphine – Approved by FDA in October, 2002 – Result of DATA 2000 – Long-acting partial opioid agonist – Sublingually effective – Can be taken once a day or less frequently – Prescribed by private practitioner with waiver The Medications • Naltrexone – Long-acting opioid antagonist – Orally effective – Can be taken once a day or less frequently – Benefits subgroups of opioid addicts Addiction as a Biopsychosocial Disease • OMT addresses the biological aspect • Psychosocial aspects addressed – Substance abuse counseling – Mental health treatment – Support and self-help groups • Accreditation standards – Should improve treatment – Eliminate “gas and go” model Women’s Issues • • • • • • • Higher levels of dual diagnosis than men Childcare Transportation Domestic Violence Educational/Vocational Financial Pregnancy How to Address Women’s Issues • • • • Accreditation standards Variable levels of resources Women’s Set-Aside funds One-stop shopping Dual Diagnosis • • • • Depression/mood disorders Anxiety disorders/PTSD Eating disorders Symptoms – Guilt and shame – Low self esteem Dual Diagnosis • • • • Train counseling staff Availability of therapist Availability of psychiatrist Staff with expertise in “survivor” issues – Lifetime prevalence of drug abuse > 4 times greater in women who report history of sexual assault • Support/therapy groups Childcare Issues • Most women in treatment are of childbearing age • Children as barrier to treatment • Services to address – Children welcome – On-site child care – Parenting classes Transportation Issues • Lack of transportation as barrier to treatment • Clinics in “out of the way” areas • Services to address – Use of medical transportation for Medicaid patients – Site program close to public transportation – Give “take-homes” when earned – Van service Domestic Violence • Train staff • Facilitate referral to shelter when appropriate • Support/therapy group Educational/Vocational Issues • Most women in treatment are “undereducated” and “underemployed” • Services to address: – Train staff about community resources/state-funded programs – On-site vocational counselor – Address “sex for drugs” issues Financial Issues • Treatment is expensive • Proprietary vs. publicly-funded non-profit programs • Services to address patient issues – Accept Medicaid as payment – Allow for reduced fee/indigency – Counsel on budgeting – Counselor referrals to/interventions with local service agencies Financial Issues • Program issues – Fund raising – Lobbying for higher state/federal funding Considerations for Treatment of Pregnant Opiate Addict • • • • • • • Tolerance level Chronicity of use Route of administration Pregnancy history Motivational level Recovery environment Ideal vs. Reality OMT/MAT as Standard of Care • Steady levels of opiates normalize neuroendocrine functioning and prevent fetal distress • Decreases rates of pregnancy complications, e.g. miscarriage, stillbirth, IUGR, abruptio placenta, infection, hemorrhage • Improves prenatal care • Allows for psychosocial interventions to improve level of functioning Perinatal Addiction • Importance of pregnancy testing at intake • Priority admission should be given to pregnant patients • Family planning as counseling issue with periodic pregnancy testing, especially during medically supervised withdrawal • Dose of methadone should be individually determined and adequate to control craving and prevent withdrawal syndrome Perinatal Addiction • MMT patients who become pregnant should be continued at established dose. A midtrimester reduction may be appropriate in anticipation of 3rd trimester dose increase. • Altered pharmacokinetics during 3rd trimester often require dose increases and often a split dose to “flatten the curve” and improve maternal and fetal stability. Perinatal Addiction • There is no consistent correlation between maternal methadone dose and the severity of neonatal withdrawal syndrome (Stimmel et al., 1982). • Protocols are available for scoring signs of opioid withdrawal to guide the appropriate use of medications to facilitate a safe and comfortable withdrawal of the passively addicted neonate (Finnegan, 1985). Perinatal Addiction • Breast-feeding may be encouraged during MMT - if not otherwise contraindicated (Kaltenbach, 1992). • Multiple longitudinal studies find that methadone-exposed infants score well within the normal range of development (Kaltenbach, 1992). Perinatal Addiction • Obstacles and barriers to MMT must be removed for the pregnant patients. • More research is needed on innovative models of treatment including medically supervised withdrawal during pregnancy with residential care, intensive relapse prevention and monitoring, high-risk prenatal care. When appropriate hospitals, clinics and individual obstetricians could provide methadone maintenance. Withdrawal during Pregnancy Rarely appropriate during pregnancy (ASAM 1990) • Same recidivism as non-pregnant opioid addicts • Slow withdrawal between 14 and 32 week Patient lives in an area where MM is not available. Patient refuses to be placed on MM. Patient has been stable and requests withdrawal prior to delivery. Withdrawal during Pregnancy • No harm reduction with OMT • Patient has been so disruptive to the treatment setting that the treatment of other patients is jeopardized, necessitating the removal of the patient from the program. Pregnancy Comprehensive OMT with adequate prenatal care can reduce the incidence of obstetrical and fetal complications, in utero growth retardation, and neonatal morbidity and mortality (Finnegan, 1991). Model Perinatal Program • • • • On-site prenatal care On-site well-baby care On-site child care Educational groups – Pregnancy/medical issues – Methadone and pregnancy – Effects of drugs of abuse, including alcohol and nicotine, on fetus Model Perinatal Program • Educational groups--continued – Nutrition – Baby care – Parenting skills--include fathers – Contraception/Family Planning – Domestic Violence Model Perinatal Program • Counseling on pregnancy termination and adoption • On-Site Psychiatric/Psychological evaluation and treatment Use of Psychotropic Medication During Pregnancy • Weigh risks vs. benefits • Inform patient of drug’s potential for teratogenic or other adverse effects (Category) • Consider consequences of untreated psychiatric illness • Use lowest effective dose Antidepressants in Pregnancy • No increase in major malformations – ?cardiac defects with paroxetine • No increase in long term neurodevelopmental adverse outcomes • SSRI’s in third trimester – may see withdrawal syndrome in neonate – increase in persistent pulmonary hypertension – no long term residual effects • Tricyclics relatively safe • MAI inhibitors contraindicated Benzodiazepines During Pregnancy • Slight increase in oral clefts • Possible withdrawal syndrome • No long term neurodevelopmental adverse effects Risks of Untreated Depression • Increase in miscarriage, hypertension and preeclampsia • Increase in likelihood of relapse to depression with stopping antidepressant medication • Global IQ negatively associated with duration of depression • Language development negatively correlated with number of postnatal depressive episodes Addressing Stigma • EDUCATE OURSELVES! – “I don’t believe in methadone!” – ASAM addressing physician bias • Arizona study -- 96% refusal to treat or give pain meds • Example of physician opioid addict Addressing Stigma • EDUCATE OURSELVES!--continued – Need to educate therapeutic communities, Minnesota model programs – Need to educate Twelve Step community • Methadone/buprenorphine as prescribed medications rather than drugs of abuse • Patients on OMT can work a program of recovery Addressing Stigma • Educate service agencies and the general public – Arizona study -- 66% refused employment or lost job • Educate patients about the chronic disease concept – Methadone/buprenorphine as corrective, not curative • Educate family members Addressing Stigma • Publicly funded programs should be mandated to accept patients on OMT • Private programs should be encouraged to accept patient on OMT – Great need for residential treatment/halfway houses for women (pregnant or non-pregnant) and their children Addressing Stigma • Patients should be encouraged to get involved in advocacy • Patients need to risk divulging status to treatment providers with support from program staff