Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
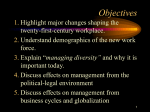
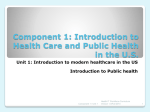
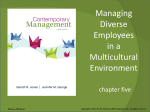
PRODUCTIVITY AND COSTS IN THE SYSTEM OF HEALTH CARE Cost Identification Analysis The first type of analysis we will consider is cost identification. Generally speaking, cost identification studies measure the total cost of a given medical condition or type of health behavior on the overall economy. The total cost imposed on society by a medical condition or a health behavior can be broken down into three major components: Direct medical care costs Direct nonmedical costs Indirect costs Direct medical care costs encompass all costs incurred by medical care providers, such as hospitals, physicians, and nursing homes. They include such costs as the cost of all necessary medical tests and examinations, the cost of administering medical care, and the cost of any follow-up treatments. Direct nonmedical costs represent all monetary costs imposed on any nonmedical care personnel, including patients. For the patient, direct nonmedical costs include the cost of transportation to and from the medical care provider, in addition to any other costs borne directly by the patient. For example, the patient may require home care or have specific dietary restrictions. Others may also be influenced by the treatment. Indirect costs consist primarily of the time costs associated with implementation of the treatment. Indirect costs include the opportunity cost of the patient’s (or anyone else’s) time that the program affects, especially because many health behaviors and medical conditions result in lost productivity due to injury, disability, or loss of life. Consider the substance abuse program previously discussed. Costs should reflect the opportunity costs of the time needed to educate workers about the potential dangers of substance abuse. The time cost is borne by the employer and equals the value of forgone production. Uses of Medical Funds Uses of Medical Funds the data in the figure show that great strides have been taken in terms of more people insured in the United States. A Note on the Relation between System Structure and Performance Health care is extremely labour-intensive, perhaps more than any other public sector activity. With more than six million workers, health and welfare constitute one of the most significant sectors of the economy in the EU, providing employment for 9.7% of the EU workforce (European Commission 2002). While health care consumes between 7% and 11% of the gross domestic product (GDP) in western European countries, approximately 70% of health budgets are allocated to salaries and other charges related directly to employment. In CEE and the NIS of the former USSR the health sector has an even greater role in employment due to the relative underinvestment in capital, resulting in a labour-intensive model of service delivery. Approaches to analysing future trends Medical Care Quality Mapping the future of HRH in Europe: analysing the factors affecting the health care workforce While the different approaches to analysing trends in health and HRH explored in the previous section may contribute usefully to exploring future trends in Europe, it is clear that no single discipline can address all aspects of human resources using these three perspectives simultaneously. Instead, a multidisciplinary approach is required to examine the full array of forces affecting HRH and to gain insights about how and why they are changing. Amount of Medical Care Spending A framework for analysing future trends in HRH Demographic trends Demographic trends pose one of the most fundamental challenges to optimizing HRH, shaping the future health labour market directly, by impacting on the supply and composition of the health care workforce, and indirectly, by influencing the demand for products and services. the data in the figure show that great strides have been taken in terms of more people insured in the United States. Direct effects Across Europe, the ageing of populations - a consequence of persistently low fertility rates coupled with substantial gains in life expectancy - has emerged as a critical policy issue with important implications for both the nature of health care and the workforce that will provide it. The United Nations predicts that the population of Europe (including the Russian Federation) will fall from 726 million in 2003 to 696 million in 2025, resulting in a decline of the European share of the world's population from 11.5% to 9% (United Nations 2003). Within the 15 countries belonging to the EU before May 2004, the average age of the population is predicted to rise from 38.3 years in 1995 to 41.8 in 2015, with consequences for the available labour force. Thus, the working-age population, which increased consistently until the early 1990s, is estimated to decline over the next 25 years (European Commission 2000). Trends in the share of the female workforce as a percentage of the total health workforce in selected countries in the 1990s Medical Care Quality Lisbon Strategy set out in 2000, the Stockholm European Council in 2001 recommended that Member States increase significantly the number of older people (aged 55-64) remaining in the workforce and the Barcelona European Council in 2002 proposed increasing the age of retirement by five years by 2010 (currently it averages 58 years). Yet, in 2001, the employment rate of older workers was only 38% in the 15 Member States of the EU pre2004 and 37% in the enlarged EU (European Commission 2002). This figure is substantially lower in, for example, France, Italy, Belgium and Luxembourg, mainly because of advantageous earlyretirement schemes that contrast with the lack of employment opportunities in CEE. In general, there seems to be a trend towards early retirement. As a result, the length of retirement compared to the duration of working life has increased in all parts of Europe. It seems increasingly obvious that any increase in workforce participation by older workers will thus require fundamental changes in pension schemes and in employers' policies on recruitment and retention, including organizational practices and working conditions. A Note on the Relation between System Structure and Performance Female practising physicians as a percentage of all practising physicians in selected countries in the 1990s The TSB curve represents the monetary value of the total social benefit generated from consuming medical care. The curve is positively sloped to reflect the added monetary benefits that come about by consuming more medical care. Figure 3-3 provides some average estimates of the PV of lifetime earnings (including fringe benefits) by age and gender, discounted using a 3.0 percent discount rate. Table 3-1 summarizes the findings for the scenarios where students contract meningococcal disease at 2 times and 15 times the national average. For example, assume that a new medical treatment, new, is being compared to an existing treatment, old, and the cost and medical effectiveness of each treatment are C old, C new and E old, E new respectively. If the new treatment is less costly than the old (C new < C old) and more effective ( E new > E old), then the new treatment is said to dominate the old and should be adopted. An Application of Cost-Effectiveness Analysis: Autologous Blood Donations – Are They Cost Effective? THANK YOU!