Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
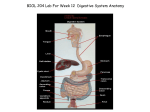
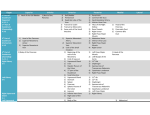
Dr. Hendershot OMM Lecture – Abdominal Exam Objectives: Describe the needed historical data(Hx) and review of systems (ROS) in a patient with an abdominal complaint Interpret how this information may help with the differential diagnosis and refinement of your diagnosis Identify the techniques of the integrated abdominal examination Organize historical and physical data into a comprehensive SOA(D)P RUQ – liver, GB, pylorus, duodenum, pancreas head, r.adrenal, r kidney upper pole, end of ascending colon, beg of transverse colon LUQ – liver left lobe, spleen, stomach, pancreas body, l. adrenal, l. kidney upper pole, end of transverse and beg of descending colon RLQ – r. kidney lower pole, cecum, appendix, beg of ascending colon, r. ureter, r. ovary, r. fallopian tube, r. spermatic cord, uterus if enlarged, bladder if enlarged LLQ - l. kidney lower pole, sigmoid colon, end of descending colon, l. ureter, l. ovary,, l. fallopian tube, l. spermatic cord, uterus if enlarged, bladder if enlarged *** kidneys, duodenum, and pancreas are posterior and cannot be palpated in adults, in children you may be able to palpate renal masses *** Symp: pain, spasm, nausea, vomiting, rectal bleeding, abd distension, BM changes, early satiety, jaundice, pruitis **Don’t forget to ask women about last period and pregnancies! Pain Descriptors: Pain – mucosal irritation, smooth muscle spasm, peritoneal irritation, capsular swelling or direct nerve stimulation Acute pain: acute perforation, inflammation, torsion of organ (Determine location at onset, localization, character, and radiation; small intestine radiates to umbilicus or epigastric area, appendicitis begins at umbilicus; localization – appendicitis may localize to RLQ .) Description of pain: gastric ulcer perforation- burning; dissecting aneurysm –tearing; intestinal obstruction – gripping; pyelonephritis – dull; nephrolithiasis/renal colic – crampy Referred pain – pain originates areas supplied by somatic nerves entering the spinal cord at the same segment as the sensory nerves from the organ responsible for the pain Time of pain : with food –peptic ulcer, 2-3 hours after eating –duodenal ulcer; nocturnal –duodenal ulcer; pain after eating – mesenteric ischemia (abdominal angina) Pain from Hollow Viscera ;crampy/paroxismal , often poorly localized , related to peristalsis , patient writhing on exam table Pain from Peritoneal Irritation; steady/constant , often localized , patient lies still with knees up Area of pain Affected Organ substernal esophagus esophagitis shoulder diaphragm subphrenic abscess Epigastric stomach, duodenum GB, liver, pancreas Clinical gastric & duodenal ulcer cholycystitis, hepatitis, pancreatitis Right scapula biliary tract biliary colic Mid back aorta, pancreas aortic dissection, pancreatitis periumbilical small intestine obstruction Hypogastrium colon diverticulitis, UC Sacrum rectum proctitis, abscess Nausea and vomiting – irritation of peritoneum, perforation of an organ; obstruction of bile duct, ureter, or intestine; or toxins. Extra abdominal conditions include: CNS conditions, pregnancy, MI, drug toxicity - Ask: color, how long, often, related to eating?, stool changes? o How long-relation of pain to emesis -in acute appendicitis pain precedes emesis by a few hrs. o o o Odor or color to vomitus- acute gastritis causes stomach contents to appear. Biliary colic produces green-yellow vomitus. Intestinal obstruction reveals fecal smelling emesis. Nausea without vomiting is seen in hepatocellular disease, pregnancy, and metastatic disease. Emesis and hearing and tinnitus may be seen with Meniere’s disease. BM changes – stool chart - Ask: How long have you had the diarrhea-onset after a meal suggests viral infection or toxin o 2. How many bowel movements daily-multiple movements may mean a bacterial infection o 3.Did the diarrhea start suddenly? o 4. Are they malodorous, bloody, watery- watery diarrhea is associated with inflammatory disease of small or large bowel. Bloody diarrhea can be caused by the bacteria shigella or amebiasis. o 5. Is the diarrhea associated with abdominal pain, decreased appetite, nausea, vomiting? Chronic diarrhea – - Ask: How long have you has diarrhea? o 2. Do you have diarrhea altering with constipation? - colon cancer or diverticulitis o 3. Are stools watery? -inflammatory bowel disease & protein losing enteropathies; loose? – diseases of left colon; floating - malabsorption ; or malordorous? o 4. Is there any blood, mucus, undigested food? - Bloody stool mixed with mucus- inflammatory bowel disease. o 5. What is color? Any relation to eating and timing? – IBS more diarrhea in AM. o 6. How many BM’s/day? o 7. Any association with pain, distention, nausea, or emesis? o 8. Any weight loss? Constipation - Ask: How long constipated, how often do you have BM? o 2. What is the size? – thin stools associated with rectal cancer; Color? – pale stools absence of bile o 3. Any blood or mucus? o 4. Are there alternating periods with diarrhea? o 5. Any flatus? Weight change or appetite change? – thyroid Rectal bleeding bright red blood (hematochezia) – tumors, diverticular disease, ulcerative colitis. red blood mixed with stool- inflammatory disease, tumors, or hemorrhoids. .Black tarry stools (melena)-bleeding from above the small bowel caused by stomach tumors or ulcer disease though may also be red Silver colored stools ( acholic )- dudodenal cancer with sloughing off of tissue. Tenesmus – painful, continued straining during stooling caused by lesion in distal rectum or anus How long? Any streaking with blood? any mixing with stool? Any rectal sensation? Any vomiting, diarrhea, abdominal pain, sweating, weight changes Jaundice – think LIVER! How long? Did it occur slowly or suddenly? Any abdominal pain? weight loss? Nausea? Vomiting? Any fevers? Chills? Pruritis? Any hx of transfusions? IV drug use? Tattooing?- Hepatitis C Any travel abroad? Ingestion of raw seafood?- Hepatitis A Changes in color of stool or urine? Type of work performed and hobbies – Hepatitis B Clues 1.Slowing developing jaundice with pale stools-bile obstruction with stones or cancer 2.Rapid jaundice with nausea and loss of appetite-liver disease such as viral hepatitis 3.Liver enlargement without pain to palpation-liver toxicity as alcoholism or toxic chemical exposure 4. carbon tetra chloride and vinyl chloride may cause liver disease from occupational exposure Abdominal distension – increased gas in intestines from malabsorption, irritable colon, ascities in liver How long? Any relation to eating? Any changes with the passage of gas from above or below? Any nausea? Emesis? Weight loss? Appetite change? Bowel changes? Shortness of breath? Abdominal pain? Clues 1. Intermittent distension related to eating –relieved by passage of gas 2.Slow distension ( ascites)- liver disease or malignancy; with shortness of breath-congestive heart failure; possible -aortic aneurysm Abdominal mass – may be hernia or neoplasm inside cavity/skin Pulsatile mass in abdomen- think aortic aneurysm Abdominal nodule – cutaneous Sister Mary Joseph nodule - cutaneous metastasis localized to the umbilicus (malignancy/carcinoma) Pruritus-itching 1.Rectal itching (pruritis ani)-fistulas, parasites, psoriasis, or diabetes 2. Generalized itching- chronic renal or liver disease, in elderly may be winter itch or dry skin alone 3.Intense generalized itching- lymphoma , Hodgkin’s disease, or cancer of GI tract **OMM exam during all phases of exam with painful areas last! 1. 2. Inspection.. general appearance, respiration, skin, hands/nails, face, abdomen, asymmetry, ecchymosis a. Silver striae = weight loss b. Purple striae = adrenocortical excess c. Grey turner sign = flanks from pancreatitis d. Cullens sign = bluish umbilicus from hemoperitoneum e. Caput medusa = dilation of veins at umbilicus Auscultation… bowel sounds 3. 4. a. Normal bowel sounds are every 5-10 seconds b. Low pitched rumbling sounds are known as borborygmi c. Succussion splash - while moving pt. side to side a sloshing sound is heard – distention of stomach or colon d. bruits may mean renal artery or aortic stenosis e. peritoneal friction rub – heard in right or left upper quadrant with hepatic or splenic disorders Percussion… fluid, gas, mass presence a. Start midclavicular then downward to liver b. Traube space at 6th rib superiorly, axillary line laterally and costal margin inferiorly c. Ascites – dullness will shift to dependent position (shifting dullness) and fluid wave Chapman’s Points 5. OMT… viscerosomatic reflex either para/sympathetic a. Para- look for changes in high cervical region (vagus) and sacral b. C1-C2 right sided – pancreas,liver,GB,small intestine, ascending colon and right half of transverse colon c. C1-C2 left side – esophagus , stomach, and duodenum d. sacral - S2-4 - left half transverse colon, descending colon, sigmoid, and rectum e. Parasymp: VAGUS! Pharynx down to splenic flexure f. Sympathetics in splanchnics (celiac ganglion in foregut, sup mes in midgut, inf mes in hindgut) i. Celiac ganglion: T5-9 to distal esophagus, stomach, prox duodenum, liver, gallbladder, spleen, pancreas ii. Sup mesenteric: T8-12 to distal duodenum, pancreas, jejunum, ileum, asc colon, transverse colon iii. Inf mesenteric: T10-L2 to distal transverse colon, desc colon, sigmoid colon, rectum 6. Lymphatics…. Left off slide 39/56