Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
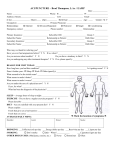
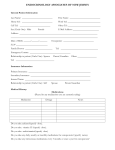
WakeMed Children’s Endocrinology & Diabetes 23 Sunnybrook Road, Suite 200, Raleigh, NC 27610 (919) 350-7584 NEW PATIENT Why is your child being seen today? What is your preferred pharmacy? ____________________________________________________________ _____________________________________________________________ ____________________________________________________________ _____________________________________________________________ Who is your child’s regular doctor? What is your preferred contact number? ___________________________________________________________ _____________________________________________________________ BIRTH HISTORY: SURGICAL HISTORY: ☐Full Term ☐Premature: _________ weeks Has your child had any surgeries? ☐ Yes (list) ☐No ☐Vaginal ☐C-section ____________________________________________________________ Any problems during the pregnancy? ☐Yes (list) ☐No ____________________________________________________________ ___________________________________________________________ ALLERGIES: Any problems with the delivery? ☐Yes (list) ☐No Does your child have any allergies to medications? ___________________________________________________________ ☐ Yes (list name & type of reaction) ☐ No Birth Weight______________ Birth Length______________ ____________________________________________________________ Did your child need help breathing after birth? ☐Yes ☐No Does your child have any allergies to food? Did your child go to the NICU after birth? ☐Yes ☐No ☐ Yes (list) ☐No ______________________________________ Infant Diet: ☐Breast Milk MEDICATIONS: ☐Formula MEDICAL HISTORY: Please list all of your child’s current medications, Has your child had any of the following: including vitamins & supplements. ☐Asthma ☐Allergies (seasonal) ☐ADD/ADHD NAME ☐PCOS (polycystic ovarian syndrome) ☐Thyroid Disease _____________________________________________________________ ☐High Blood Pressure ☐High Cholesterol _____________________________________________________________ List any other medical conditions that your child has: _____________________________________________________________ _________________________________________________________________ _____________________________________________________________ _________________________________________________________________ _____________________________________________________________ _________________________________________________________________ _____________________________________________________________ Has your child ever been hospitalized? ☐ Yes (list) ☐No _____________________________________________________________ _________________________________________________________________ _____________________________________________________________ _________________________________________________________________ _____________________________________________________________ OVER DOSE FREQUENCY IMMUNIZATIONS: FAMILY HISTORY: Are your child’s immunizations up to date? ☐Yes ☐No Mother’s Height? ___________ Father’s Height?__________ Has your child received a flu shot this year? ☐Yes ☐No Age of mother’s first menstrual period? _______________ Did anyone go through puberty: ☐early ☐late SOCIAL HISTORY: PARENTS NAMES AGE OCCUPATION _______________________________________________________________ Please identify any blood-relatives with the following medical problems: _______________________________________________________________ ☐Married ☐Separated/Divorced ☐Not Married Yes Diabetes, Type 1 Lives with: Diabetes, Type 2 ☐Both Parents ☐Mother Only ☐Father Only Early heart disease ☐Other _____________________________________________________ SIBLING NAMES AGE MEDICAL PROBLEMS? _______________________________________________________________ High blood pressure High cholesterol _______________________________________________________________ Thyroid disorder _______________________________________________________________ Overweight What school or day care does your child attend? ______________________________________________________________ What grade is your child in? _____________________________ Next Page Polycystic ovarian syndrome (PCOS) Other: No Who/relation/when WakeMed Children’s Endocrinology & Diabetes NEW PATIENT—Symptom Checklist DOES YOUR CHILD HAVE ANY OF THE FOLLOWING: YES NO General ☐ ☐ Dietary Change ☐ ☐ Fatigue ☐ ☐ Weight Gain ________ pounds ☐ ☐ Weight Loss ________ pounds ☐ ☐ ☐ ☐ Eyes Visual disturbances Date of last eye exam ____________ ☐ ☐ ☐ ☐ ☐ ☐ Ears/Nose/Throat Earaches Nosebleeds Sinus/Allergies ☐ ☐ ☐ ☐ Respiratory Cough Shortness of breath ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Cardiovascular Chest Pain Fainting Palpitations Sweating ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Gastrointestinal Abdominal Pain Constipation Nausea Vomiting Mental Health Anxiety Mood changes Problems in school During the past month, has the patient been feeling down, depressed, hopeless, or irritable? During the past month, has the patient had little interest or pleasure in doing things? YES NO ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Skin Hair changes Injection site problems Skin lesion or rash ☐ ☐ ☐ ☐ ☐ ☐ Musculoskeletal Back Pain Joint Pain Muscle aches ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Endocrine Cold intolerance Excessive thirst Excessive urination Heat intolerance Hypoglycemia Thyroid issues ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Neurologic Dizziness Headache Paresthesia (burning/tingling) Seizures ☐ ☐ ☐ ☐ ☐ ☐ Hematology Blood clots Easy bruising Excessive bleeding ☐ ☐ ☐ ☐ Genitourinary Amenorrhea (no menses) Pain with urination Date of Last Menses_______________ TB Screen Has the patient ever had a positive TB skin test? Has the patient had any unexplained night sweats, weight loss, fatigue, or persistent cough?