Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
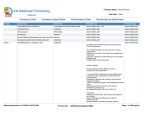
Premera Blue Cross Medicare Advantage Pharmacy Policy Updates The following recommendations included on this update have been approved by the Pharmacy and Therapeutics Committee (P&T). Please note: For Medicare Advantage plans, most Part D–eligible drugs and drug policies are not effective and administered until Centers for Medicare and Medicaid Services approval is obtained. Please refer to the most current approved formulary document, which is available at premera.com/medicare-advantage/pharmacy-services/ Pharmacy policies are updated and available on the secure provider Medicare Advantage website at premera.com/wa/provider/medicare-advantage/; simply click on the Get Started button. Class Reviews Colony-Stimulating Agents • • The following drugs were reviewed: Filgrastim (Neupogen®), Pegfilgrastim (Neulasta®), Sargramostim (Leukine®) and a new drug, TBO-filgrastim (Granix®). Significant changes: o TBO-filgrastim added to formulary o Health plan: Remove filgrastim and pegfilgrastim from prior authorization (PA) Health Plan: All agents on formulary Prothrombin Complex Concentrate • • The following drugs were reviewed: Bebulin® VH, Profilnine® SD, and Feiba® NF and a new drug, Kcentra®). Significant changes: o Kcentra® added to Formulary o Non-formulary: Bebulin®VH and Profinine®SD Health Plan: All agents covered as medical benefit ESA Agents • Page | 1 The following drugs were reviewed: epoetin alfa (Epogen®), epoetin alfa (Procrit®), darbepoetin alfa (Aranesp®) and peginesatide (Omontys®) An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) • Significant changes: No changes to current formulary setup Health Plan: Formulary agents are epoetin alfa (Epogen®), epoetin alfa (Procrit®) and darbepoetin alfa (Aranesp®) Ulcerative Colitis Mesalamine Products • • The following drugs were reviewed: Oral: Asacol®, Delzicol®, Apriso®, Pentasa®, Lialda® Rectal: Canasa®, Rowasa(r) Significant changes: o Health Plan: All agents are now formulary with no restrictions Health Plan: All agents on formulary New Drugs: Granix® (TBO-Filgrastim – syringe) • Please refer to the Colony-Stimulating Agents class review above KCentra® (Human Prothromin Complex– kit) • Please refer to the Prothrombin Complex Concentrate class review above Xofigo® (Radium-223 dichloride – vial) • Indication: treatment of patients with castration-resistant prostate cancer (CRPC), symptomatic bone metastases and no known visceral metastatic disease. Health Plan: Medical Benefit with criteria for use Clinical criteria for use: o Must be prescribed by, or in consultation with, an oncologist Lymphoseek® (Technetium Tc 99m tilmanocept - injection) • Page | 2 Indication: indicated for lymphatic mapping with a hand-held gamma counter to assist in the localization of lymph nodes draining a primary tumor site in patients with breast An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) cancer or melanoma. Health Plan: Medical Benefit Brintellix® (Vortioxetine HCL - tablet) • Indication: Treatment of Major Depressive Disorder Health Plan: Formulary with PA Criteria for use: • Documented trial, failure, intolerance or contraindication to at least two formulary generic SSRI medications New Strengths & Formulations: Nymalize® (Nimodipine - oral solution) • Indication: For the improvement of neurological outcome by reducing the incidence and severity of ischemic deficits in adult patients with subarachnoid hemorrhage (SAH) from ruptured intracranial berry aneurysms regardless of their post-ictus neurological condition Health Plan: Medical Benefit Marqibo® (Vincristine Sulfate - infusion) • Indication: Treatment of adult patients with Philadelphia chromosome negative (Ph-) acute lymphoblastic leukemia (ALL) in second or greater relapse or whose disease has relapsed following two or more anti-leukemia therapies Health Plan: Medical Benefit with PA Criteria for use: • Must be prescribed by, or in consultation with, an oncologist Minastrin 24 FE® (Noreth A-ET Estra/FE Fumarate - chewable tablet ) • • Page | 3 Indication: indicated for use by women to prevent pregnancy. Formulary alternatives: Junel Fe, Microgestine Fe, Loestrin Fe 1/20 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) Health Plan: Non-formulary Lo Minastrin FE® (Noreth A-ET Estra/FE Fumarate - chewable tablet ) • • Indication: indicated for use by women to prevent pregnancy. Formulary alternatives: Junel Fe, Microgestine Fe, Loestrin Fe 1/20 Health Plan: Non-formulary Quartette® (L-norgest-Eth Estr/Ethinyl Estradiol - tablet) • • Indication: Combination oral contraceptive to prevent pregnancy and postcoital contraception. Formulary alternatives: generic Jolessa, generic Quasense Health Plan: Non-formulary Zenzedi® (Dextroamphetamine Sulfate - tablet ) • • Indication: Treatment of ADHD and Narcolepsy Formulary alternative: generic dextroamphetamine sulfate Health Plan: Non-formulary Zubsolv® (Buprenorphine/Naloxone - sublingual tablet) • • Indication: Treatment of opioid dependence Formulary alternative: generic buprenorphine – naloxone SL tablets Health Plan: Non-formulary Kogenate® FS (Antihemophilic Factor VIII – kit) • Indication: control and prevention of bleeding episodes in adults and children (0-16 years) with hemophilia; peri-operative management in adults and children with hemophilia A; routine prophylaxis to reduce the frequency of bleeding episodes and the risk of joint damage in children with hemophilia A with no preexisting joint damage. Health Plan: Medical Benefit Page | 4 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) Trokendi XR® (Topiramate - capsule) • • Indications: o Initial monotherapy in patients 10 years of age and older with partial onset or primary generalized tonic-clonicseizures and adjunctive therapy in patients 6 years of age and older with partial onset or primary generalized tonic-clonic seizures. o Adjunctive therapy in patients 6 years of age and older with seizures associated with Lennox-Gastaut syndrome Formulary alternatives: generic topiramate immediate release, sodium valproate, clonazepam, lamotrigine Health Plan: Non-formulary Astagraf XL® (Tacrolimus - capsule) • Indication: Prophylaxis of organ rejection in patients receiving a kidney transplant with mycophenoloate motefetil and corticosteroids with or without basiliximab induction Health Plan: Formulary Valchlor® (Mechlorethamine HCL - gel) • Indication: topical treatment of Stage IA and IB mycosis fungoides-type cutaneous Tcell lymphoma in patients who have received prior skin directed therapy Health Plan: Formulary (Specialty) with PA Criteria for use • Must be prescribed by, or in consultation with, an oncologist • Trial, failure, intolerance or contraindication to one conventional therapy including, but not be limited to: tazarotene cream or gel, imiquimod, bexarotene gel or carmustine Page | 5 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) New US Food and Drug (FDA) Approvals: Pramosone® (Hydrocortisone/Pramoxine - lotion) • • Indication: For the relief of inflammatory and pruritic manifestations of corticosteroidresponsive dermatoses Formulary alternatives: Proctocream HC, Procto-pak, Proctozone HC Health Plan: Non-formulary Analpram® HC (Hydrocortisone/Pramoxine - lotion, cream, cream singles) • • Indication: For the relief of inflammatory and pruritic manifestations of corticosteroidresponsive dermatoses Formulary alternatives: Proctocream HC, Procto-pak, Proctozone HC Health Plan: Non-formulary Pediprox 4-Nail ® (Ciclopirox/Nail Lacquer/Foot Deod. - kit) • • Indication: Topical treatment in immunocompetent patients with mild to moderate onychomycosis of fingernails and toenails without lunula involvement, due to Trichophyton rubrum Formulary alternatives: oral antifungals (e.g. terbinafine, itraconazole, fluconazole) Health Plan: Non-formulary Proctofoam HC® (Hydrocortisone/Pramoxine - topical foam) • Indication: Relief of the inflammatory and pruritic manifestations of corticosteroidresponsive dermatoses of the anal region Health Plan: Formulary Page | 6 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) Other Formulary Changes: Vibramycin® (Doxycycline Monohydrate - oral suspension) • • Indication: to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. Formulary alternatives: doxycycline tablets or capsules Health Plan: Non-formulary New Generic Medications First time generics to market • Lidocaine patch (Lidoderm®) - Keep formulary with prior authorization (PA) and quantity limits • Sulfacetamide Sodium lotion (Ovace Plus®) - Benefit exclusion (non-FDA approved) • Sulfacetamide Sodium lotion (Ovace Plus Wash®) - Benefit exclusion (non-FDA approved) • Niacin (Niaspan®) - Formulary • Voriconazole (VFend®) - Add to formulary • Azacitidine (Vidaza®) - Formulary with PA • Sulfacetamide sodium/sulfur (Avar-E LS cream®) - Benefit exclusion (non-FDA approved) • Sulfacetamide sodium/sulfur (Avar LS®) - Benefit exclusion (non-FDA approved) • PNV59/IRON, carbonyl/FA/DSS/DHA (CitraNatal Harmony®) - Benefit exclusion (prenatals with DHA are not covered) • Butalbit/acetamin/caff/codeine (Fioricet with codeine®) - Keep non-formulary • Adenosine (Adenoscan®) - Medical benefit • Paricalcitol (Zemplar®) - Formulary with PA to determine Part B vs Part D benefit and step therapy • Gatifloxacin (Zymaxid®) - Add to formulary • Clonidine HCL (Kapvay ER®) Page | 7 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) • • • • • • - Formulary with PA Ceftibuten dihydrate (Cedax®) - Add to formulary PNV/FA/b6/calcium phos/ginger (B-Nexa®) - Not added to formulary – exceeds cost limit of adding new vitamins to formulary PNV NO.66/iron, carbonyl/FA/DHA (Active OB®) - Benefit exclusion (prenatals with DHA are not covered) Rabeprazole (Aciphex®) - Add to formulary, remove restrictions Dexmethylphenidate (Focalin XR®) - Add to formulary, remove PA Tobramycin (TOBI®) - Non-formulary Health Plan – Clinical Policy Updates: Policy Name Zostavax® Neupogen® Neulasta® Estrogen for Men Cimzia® Stelara® Tykerb® Oxycontin® Potiga® Colcrys® Page | 8 Criteria Changes Policy has been retired Policy has been retired Policy has been retired Policy has been retired Policy updated with the new indication (treatment of adult patients with active psoriatic arthritis and for the treatment of adult patients with active ankylosing spondylitis). Policy updated with the new indication (active psoriatic arthritis, alone or in combination with methotrexate). Policy position statement updated with the new FDA limitation of use (Patients should have disease progression on trastuzumab prior to initiation of treatment with Tykerb® in combination with capecitabine). Added “documentation of persistent pain (expected to last longer than three months)” to criteria. Also added “as needed use” to exclusion criteria Policy updated to include requirement of documentation that benefit outweighs risk and that visual function testing will be completed at baseline and every 6 months. Removed age restriction An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) Medication Safety Alerts Sept. 1, 2013 through Oct. 31, 2013 Source: US Food and Drug Administration website Tygacil® (tigecycline): Drug Safety Communication - Increased Risk of Death Posted 9/27/2013 Infectious disease, critical care, pharmacy Audience The FDA notified health professionals and their medical care Issue organizations of a new Boxed Warning describing an increased risk of death when intravenous Tygacil is used for FDA-approved uses as well as for non-approved uses. These changes to the Tygacil Prescribing Information are based on an additional analysis that was conducted for FDA-approved uses after FDA issuing a Drug Safety Communication about this safety concern in September 2010. Tygacil is FDA-approved to treat complicated skin and skin Background structure infections , complicated intra-abdominal infections , and community-acquired bacterial pneumonia . Healthcare professionals should reserve Tygacil for use in situations Recommendation when alternative treatments are not suitable. P&T Action: Providers will be notified through Medical Policy Updates. Iclusig® (Ponatinib): Drug Safety Communication - Increased Reports of Serious Blood Clots in Arteries and Veins Posted 10/11/2013, 10/31/13, 11/5/13 Health professional, oncology Audience The FDA is investigating an increasing frequency of reports of Issue serious and life-threatening blood clots and severe narrowing of blood vessels (arteries and veins) of patients taking the leukemia chemotherapy drug Iclusig (ponatinib). Data from clinical trials and postmarket adverse event reports show that serious adverse events have occurred in patients treated with Iclusig, including heart attacks resulting in death, worsening coronary artery disease, stroke, narrowing of large arteries of the brain, severe narrowing of blood vessels in the extremities, and the need for urgent surgical procedures to restore blood flow. The FDA is actively working to further evaluate these adverse events and will notify the public when more information is available. Iclusig is a prescription medicine used to treat adults diagnosed with Background chronic phase, accelerated phase, or blast phase chronic myeloid Page | 9 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) Recommendation leukemia or Philadelphia chromosome-positive (Ph+) acute lymphoblastic leukemia, who are no longer benefiting from previous treatment or who did not tolerate other treatment. At the time of Iclusig’s approval in December 2012, the drug label contained information about the risks of blood clots in the Boxed Warning and Warnings and Precautions sections. In clinical trials conducted before approval, serious arterial blood clots occurred in 8 percent of Iclusig-treated patients, and blood clots in the veins occurred in 3 percent of Iclusig-treated patients. In the most recent clinical trial data submitted by the manufacturer to FDA, at least 20 percent of all participants treated with Iclusig have developed blood clots or narrowing of blood vessels. Healthcare professionals should consider for each patient whether the benefits of Iclusig treatment are likely to exceed the risks of treatment. Patients taking Iclusig should seek immediate medical attention if they experience symptoms suggesting a heart attack, such as chest pain or pressure, pain in their arms, back, neck or jaw, or shortness of breath; or symptoms of a stroke, such as numbness or weakness on one side of the body, trouble talking, severe headache, or dizziness. The FDA has asked the manufacturer of the leukemia chemotherapy drug Iclusig (ponatinib) to suspend marketing and sales of Iclusig because of the risk of life-threatening blood clots and severe narrowing of blood vessels. We will continue to evaluate the drug to further understand its risks and potential patient populations in which the benefits of the drug may outweigh the risks. Patients currently receiving Iclusig should discuss with their healthcare professionals the risks and benefits of continuing treatment with the drug. ARIAD Pharmaceuticals has agreed to this request to suspend marketing and sales of Iclusig while they continue to evaluate the safety of the drug. At this time, patients and healthcare professionals should follow FDA’s new recommendations: • • Page | 10 Patients currently taking Iclusig who are not responding to the drug should immediately discontinue treatment and discuss alternative treatment options with their healthcare professionals. Patients who are currently taking Iclusig and responding to An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) • the drug and whose healthcare professionals determine that the potential benefits outweigh the risks should be treated under a single-patient Investigational New Drug (IND) application or expanded access registry program while FDA’s safety investigation continues. FDA will work with the manufacturer on a plan to quickly transition these patients to a program that will allow access under an IND or expanded access registry program Healthcare professionals should not start treating new patients with Iclusig unless no other treatment options are available and all other available therapies have failed. Upon the determination of their healthcare professional, these patients can be considered for treatment under an IND or expanded access registry program. P&T Action: Ambulatory policy has been updated. Providers will be notified through the Medical Policy Updates. Potiga (Ezogabine): Drug Safety Communication - Linked to Retinal Abnormalities and Blue Skin Discoloration Posted 4/26/2013 Health professional, neurology, patient Audience The FDA is warning the public that the anti-seizure medication Issue Potiga (Ezogabine) can cause blue skin discoloration and eye abnormalities characterized by pigment changes in the retina. The FDA does not currently know if these changes are reversible. The FDA is working with the manufacturer to gather and evaluate all available information to better understand these events. The FDA will update the public when more information is available. Potiga is approved as adjunctive (added on to other anti-seizure Background medications) treatment of partial-onset seizures in adult patients 18 years and older. Pigment changes in the retina have the potential to cause serious eye disease with loss of vision. It is not yet known whether the retinal pigment changes caused by Potiga lead to visual impairment, although several patients have been reported to have impaired visual acuity. In some cases, retinal abnormalities have been observed in the absence of skin discoloration. The skin discoloration in the reported cases appeared as blue pigmentation, predominantly on or around the lips or in the nail beds of the fingers Page | 11 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014) or toes, but more widespread involvement of the face and legs has also been reported. Scleral and conjunctival discoloration, on the white of the eye and inside eyelids, has been observed as well. The skin discoloration generally occurred after four years of treatment with Potiga, but has appeared sooner in some patients. Recommendation P&T Action: Ambulatory policies have been updated to strengthen criteria for new starts: • Require documentation that benefit outweighs risk • Require documentation that visual function testing will be completed at baseline and every six months Page | 12 An Independent Licensee of the Blue Cross Blue Shield Association 029960 (02-2014)