Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
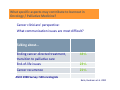
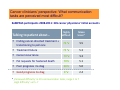
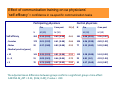
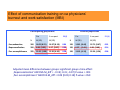
How can communication skills training ameliorate burnout and promote satisfaction at work? Monika Keller, MD, PhD Dept of General Internal Medicine & Psychosomatics University Hospital Heidelberg Burnout among cancer clinicians – what is known so far? Burnout is frequently observed among cancer clinicians: ‐ 20 – 50% high levels of emotional exhaustion (MBI) found in surveys from US, CAN, UK, Australia ‐ Burnout found to increase over time among UK cancer clinicians ‐ Oncologists‘ burnout levels equal to or lower than other specialties‘ (CH) Burnout among cancer clinicians best predicted by: ‐ ‐ ‐ High clinical workload with patient contact Insufficient institutional support Perceived need for communication skills training Shanafelt et al. 2014/15 Ramirez et al. 1995 Taylor at al. 2005 Grunfeld et al. 2000 Girgis et al. 2009 Burnout among cancer clinicians – what is known so far? Consequences of professional Burnout : ‐ Quality of patient care (medical errors, terminal sedation ) ‐ Impact on Clinician Satisfaction at work Risk of psych morbidity substance abuse, suicide, absenteism stress‐related health problems leaving oncology (early) Shanafelt et al. 2014/15 Berman et al. 2007 Taylor at al. 2005 Grunfeld et al. 2000 Girgis et al. 2009 Professional Burnout as conceptualised & assessed with Maslach Burnout Inventory (MBI) Emotional Exhaustion EE Depersonalisation* DP Burnout ‐ Personal accomplishment PA * ‚Treating patient like an object‘ What specific aspects contribute to burnout in Oncology/ Palliative Medicine? What cancer clinicians perceive as demanding & often stressful: Findings from qualitative research Breaking bad news to patients/family Discussing failure of anticancer therapy Applying highly toxic treatments to patients Grief over loss of patients Sense of helplessness, guilt, failure, sorrow Pronounced by a ‚culture of invulnerability‘ in institutions ‚doctors don‘t talk to each other‘ ‚You are not really expected to be affected by‘ ‚They see it as psychological weakness‘ Brown et al. 2009 Shaw et al. 2012 Friedrichsen 2006 Granek et al. 2012 What specific aspects may contribute to burnout in Oncology / Palliative Medicine? Cancer clinicians‘ perspective: What communication issues are most difficult? Talking about... Ending cancer‐directed treatment, transition to palliative care End‐of‐life issues Cancer recurrence 44% 23% 21% ASCO 1998 Survey: 500 oncologists Baile, Buckman et al. 2000 What specific aspects may contribute to burnout in Oncology / Palliative Medicine? Cancer clinicians‘ perspective: ‚what communication task do you find most difficult?‘ Balancing honesty with hope 55% Responding to pat‘s emotions adequately 29% ASCO 1998 Survey: 500 oncologists Baile et al. 2000 Shaw et al. 2012 Friedrichsen 2006 Cancer clinicians‘ perspective: What communication tasks are perceived most difficult? KoMPASS participants 2008‐2011: 345 cancer physicians‘ initial accounts highly difficult Mean Score* Ending cancer‐directed treatment + transitioning to pall care 76 % 5.5 Treatment failure 75 % 5.3 Cancer recurrence 70 % 5.3 Pat requests for hastened death 70% 5.1 Poor prognosis Ca diag 66% 5.0 Good prognosis Ca diag 8 % 2.4 Talking to patient about... * ‚Perceived difficulty‘ re 20 communication tasks; range 1 to 7 ‚High difficulty‘ val 5 ‐7 ‚A recipe for burnout‘: strong negative feelings when sharing bad news about a poor prognosis with patients Cancer clinicians are dealing with their own strong emotions when disclosing prognostic information to patients with advanced cancer Strong negative feelings Sadness, pain, guilt, heartbreak, stress.... 50 % 729 medical oncologists‘ answer to mailed survey (2006) Wallace et al. 2006 Baile WF 2015 ‚A recipe for burnout‘: strong negative feelings when sharing bad news about a poor prognosis with patients Cancer clinicians‘ reports how they tend to deny or avoid own strong emotions During encounters, concentrate on ‐ reducing own discomfort, ‐ less on the task and the patient (prevents empathy) Avoid uncomfortable encounters (visit length) Conceal or ‚cushion‘ bad news Clinicians‘ coping efforts strive for self‐preservation against feeling helpless and being out of control, so they don‘t get emotionally attached ‐> risk of detachment and ‚Depersonalisation‘ Baile WF 2015 Morgans & Schapira 2015 Shaw et al.2012, 2013 Stiefel et al. 2008 A recipe how communication can ameliorate or prevent burnout? ‐ Becoming aware of ... ‐ Being mindful of ... one‘s own strong emotions ‐ through non‐judgmental observation ‐ through feedback and sharing with others ‐ experiencing relief & ‚self‐efficacy‘ with alternative interactions with patients vs fear of losing control ‐ ...... Burnout among clinicians – impact of interventions Educational Program in Mindful Communication With Burnout, Empathy, and Attitudes Among Primary Care Physicians Krasner, Epstein et al. 2012 – USA N = 70 Prim care physicians attended mindfulness communication training 45 h over 12 months. Eval after 2, 12, 15 months Burnout (MBI) improved on each subscale Participation in a mindful communication program was associated with short‐term and sustained improvements in well‐being and attitudes Burnout among cancer clinicians – impact of interventions Intensive Communication Skills Teaching (CST) for Specialist Training in Palliative Medicine (PM) Clayton J et al. 2012 Australia N = 41 PM specialists/trainees attended 3‐day CST (Oncotalk model)with small group experiential learning & defined scenarios with simulated patients; 3 months post course, self‐assessed confidence in CS increased; Burnout (MBI) no sig changes observed Efficacy of a Communication & Stress Management Training on Medical Residents‘ Self‐Efficay, Stress to Communicate and Burnout‐ RCT Bragard J et al. 2010 Belgium 30‐hour communication and 10‐hour stress management skills training in small groups. Intervention group N = 49 medical residents. Significant increase in self‐efficacy and decrease in stress to communicate compared with controls Burnout (MBI) no changes, no difference between groups observed Burnout among cancer clinicians – impact of interventions Effect of a 1‐day interventional workshop on recovery from job stress for radiation therapists and oncology nurses Poulsen AA et al 2015, Australia Improved recovery skills, satisfaction with self‐care practices and perceived sleep quality. “This intervention has the potential to enhance resilience and prevent burnout ..in a cancer worker's career” Reply A Girgis: “One size doesn’t fit all” “Good communication in cancer is tough business, not for the fainthearted…” (SM Dunn, 2010) Physicians involved in the care of cancer patients and their relatives are facing numerous challenging encounters, on a daily basis where they have to deal with: conveying ‚bad news‘ of all kinds building supportive patient‐centered relationships relieving patients‘ physical and mental suffering recognizing and transforming crises reactions managing own emotional involvement striving for a balance between committed professionalism and personal integrity and well‐being How can comm skills training ameliorate burnout among cancer clinicians ? KoMPASS project Communication skills training program that aims To enhance patient‐centered communication in cancer care To foster supportive relationships between cancer patients/family and physicians involved in their care To promote cancer physicians‘ satisfaction at work and ameliorate/prevent burnout Aim of KoMPASS training courses Developing a training program that… Is relevant to physicians‘ practice Addresses and builds on their particular goals and needs Acknowledges their expertise & competence Provides protective, secure space Facilitates experiential learning Ensures transfer to physicians‘ clinical practice KoMPASS – methods Relevant to cancer physicians from any seniority and oncology specialty Intense 2 ½ days (20 hours) workshop ½ day refresher 4 months later Small groups (8 to 12 participants) 2 experienced clinician trainers; familiar with real life (psycho‐) oncology; trained psychotherapists Emphasis on experiential learning, less on ‚teaching‘ Learner‐centered approach: ensure each KoMPASS training workshops initially conducted at 8 academic sites participant practices with her/his individual issue (CIR) KoMPASS – methods I Learner‐centered approach Workshop agenda created jointly upon participants‘ needs & interest Critical incident reporting (CIR): each participant reports a case vignette of a challenging encounter with a patient/relative from his/her practice. These are shared with the group Scenarios for role plays are created from physicians‘ case vignettes Role play with trained professional patient actors (vs standardized patients) Able to take on difficult patient/relative roles Flexible: Immediate jump‐in; time‐out, variation, re‐play Authentic feedback from patient‘s perspective, responsive to physician‘s alternative interactions KoMPASS – methods II Some structured cognitive input – interactive discussions with ppt handouts Basic recommendations for patient‐centered communication Patients in crises – understanding pat‘s experience & opportunities how physicians can provide support Conveying bad news – how the SPIKES model can assist Dealing with strong – patients‘ and physicians‘ ‐ emotions End of life issues KoMPASS – methods Videotaped scripted encounter with patient‐actor (Scenario: treatment failure under palliative chemo for advanced gastric cancer) Videos viewed in small groups ‐> teaching opportunities KoMPASS – methods III Small‐group role play, structured feedback & reflection Varying role play techniques ‐e.g. change of perspective through role reversal Encouraging feedback & enactment to jointly explore communication solutions adequate to the individual patient/family –physician relationship Facilitator moderates, observing the process while leaving activity with the group. Recognizes participants‘ emotional condition. Uses ‚teaching points‘ for suggesting communication ‚skills‘ as appropriate. Encourages non‐judgemental reflection and, sometimes, ‚take‐home‐message‘ KoMPASS – experience KoMPASS – experience Experience of interacting with patient‐actor in role play ‚Unexpectedly realistic scenario‘ – helps overcoming initial timidity towards role plays Opportunity to receive credible personal feedback ‐ No risk of hurting/blaming the patient Sense of relief & achievement upon patient‘s response to alternative intervention (skill, behavior) Physician experiences beneficial impact on patient /relationship ‐> experience of self‐efficacy Limitations ‐> additional methods required (Socio‐/Psychodrama – work in process guided by Dr. Baile) KoMPASS – experience Group experience Feedback from colleagues & facilitator – mutual learning experience Allows to integrate self‐perception with how one is perceived by others ‐> self‐reflective stance and confirmation Group cohesion, shared achievement & mutual support – against sense of isolation KoMPASS – participants‘ feedback ‐ at refresher 4 months later Transfer into clinical practice? „dealing with difficult encounters has become much easier“ „I reach the patient easier and within less time (!!)“ „I put myself less under pressure to do something, I leave more space to the patient“ „I feel less miserable when I have to convey those bad, mean things (bad news) to the patient“ Four months ago, I weren‘t able to have such a conversation.. The mountain has become accessible... Studienzentrum Universität Heidelberg KoMPASS – participants‘ feedback 4 months later Self‐efficacy? „...it‘s good for this patient that I‘m taking care of him“ (longtime not aware of..) „I found out again that and why this is my profession“ „I was able to face the greatest challenge during 10 years being an oncologist – medical error ‐> ‚take on responsibility, not guilt‘, maintained patient‘s trust“ Studienzentrum Universität Heidelberg Is KoMPASS communication training ‚effective‘ ? How to assess ? Physicians‘ perspective: evaluation of training and methods Physician‐rated self efficacy, work‐related stress and ‚burnout‘ ‚Experts‘ perspective ‚Objective‘ pre‐4 mo post rating of physicians‘ interaction according to validated classification system (RIAS) of video‐documented standardized scenario KoMPASS – Controlled non-randomized design 2,5 day Kompass training T1 4 months participants Self-assessment Self-efficacy ‚Empathy‘ work stress/ burnout Controls - non participants 0,5 day refresher T2 Self-assessment Self-efficacy ‚Empathy‘ work stress/ burnout KoMPASS – Measures Physicians‘ rating ‚Self-efficacy‘- confidence & difficulty → 20 Items addressing characteristic communication tasks in cancer care (expanded from previous work) ‚Maslach Burnout Inventory (MBI-D)’ (Maslach & Jackson, 1981) → work – related stress & satisfaction (‚burnout‘) ‚Jefferson Scale of Physician Empathy’ (Hojat et al., 2004) → self-assessed patient-centered attitude Studienzentrum Universität Heidelberg Effect of communication training on ca physicians’ ‘self-efficacy’ = confidence in ca-specific communication tasks Participating physicians Control physicians Pre 4 mo post ES (d) N M (SD) M (SD) Self‐efficacy 262 4.14 (0.92) 4.69 (0.88) 0.61 ‐ Females 170 4.01 (0.92) 4.61 (0.88) ‐ Males 92 4.37 (0.88) > 10 141 6–9 <5 N Pre 4 mo post M (SD) M (SD) 181 5.08 (0.91) 5.06 (0.97) 0.66 104 4.96 (0.98) 4.89 (1.02) 4.83 (0.88) 0.52 77 5.25 (0.80) 5.28 (0.88) 4.35 (0.91) 4.81 (0.88) 0.52 122 5.28 (0.88) 5.24 (0.92) 51 4.09 (0.81) 4.66 (0.84) 0.70 29 4.81 (1.0) 4.93 (1.04) 70 3.73 (0.89) 4.47 (0.89) 0.84 30 4.57 (0.68) 4.43 (0.87) ‐ Medical practice (years) The adjusted mean difference between groups confirms a significant group x time effect: ANCOVA M_diff = 0.23, [0.06; 0.40]; P‐value = .010 Effect of CST on ca physicians’ ‘self‐efficacy’ = confidence in ca‐specific communication tasks 4 months following the training, participants report higher ‚self‐efficacy‘ when dealing with challenging communication tasks whereas control physicians‘ ‚self‐efficacy‘ has not changed ‐> Closer look into details ...... Self‐efficacy to communicate: perceived improvements of initial ‚most difficult‘ tasks? 262 training participants before and 4 months after CST highly confident* T0 highly confident T1 Ending cancer‐directed treatment + transitioning to pall care 32 % 47% Treatment failure 35 % 53% Cancer recurrence 37 % 60% Pat requests to hasten death 38% 53% Poor prognosis Ca diag 34% 60% Providing sufficient emotional support 45 % 69% Discussing with patient about... * ‚High confidence‘ val 5 ‐7 (range 1 to 7) Physician‐rated ‚self efficacy‘: impact of comm training Übergang zu palliativer Behandlung Transition to pall care Tell pat how long to live Angaben zur Lebenszeit Responding to pat‘s strong emotions Emotionale Reaktionen Mitteilung Therapiemisserfolg Treatment failure Item Wunsch sinnloser Tumortherapie Wish for futile ca treatments 5‐7 T0 5‐7 T1 Conveying ca recurrence Mitteilung Tumorrezidiv Conveying ca poor prognosis Mitteilung Krebs ungünstige Prognose Conveying ca good prognosis Mitteilung Krebs günstige Prognose 0 10 20 30 40 50 Prozent 60 70 80 90 100 Effect of communication training on ca physicians’ burnout and work satisfaction (MBI) Participating physicians Pre 4 mo post N M (SD) M (SD) ‐ Emo exhaustion 260 18.02 (8.23) 18.37 (8.18) ‐ Depersonalisation 260 6.46 (3.92) ‐ Pers accomplishment 205 31.62 (4.90) Control physicians ES(d) Pre 4 mo post N M (SD) M (SD) 0.04 181 19.81 (8.44) 19.73 (8.67) 0.01 6.17 (3.87) 0.08 181 6.37 6.86 (3.68) 0.14 32.91 (4.44) 0.28 181 33.05 (4.19) 33.28 (4.26) 0.06 (3.41) Adjusted mean difference between groups: significant group x time effect: ‚Depersonalisation‘ ANCOVA M_diff = ‐ 0.19 [‐0.31; ‐0.07] P‐value = .003 ‚Pers accomplishment‘ ANCOVA M_diff = 0.09 [0.00; 0.18] P‐value =.059 ES (d) Effect of communication training on ca physicians’ Burnout and work satisfaction (MBI) intervention control ANCOVA Emotional exhaustion ‐ ‐ n.s. Depersonalisation P= .003 Personal accomplishment ‐ P= .059 Four months following the KoMPASS training, intervention physicians show No effect on ‚Emotional Exhaustion‘ Slightly less signs of ‚Depersonalisation‘ vs an increase among controls Higher sense of ‚Personal accomplishment‘ = work satisfaction Effect of communication training on ca physicians’ Burnout and work satisfaction (MBI) Empirical support from findings: qualified communication skills training in fact does ameliorate and prevent burnout in cancer physicians sustained effect after 4 months + CST outside clinical study (bias less likely) Large sample size broad range of specialty and seniority Controlled design ? Bias due to highly motivated participants? Small group of experienced & engaged trainers ? Impact on patients‘ outcomes? How ?? By reducing physicians‘ fears Effect of communication training on ca physicians’ Burnout and work satisfaction (MBI) communication skills training does ameliorate and prevent burnout How ?? ‐> By reducing physicians‘ fears ‐> awareness of own emotional involvement ‐> awareness of professional competence –‘self‐efficacy‘ ‐> From lived experience of satifying interactions ‐> From facilitative environment to integrate behaviors learnt ‐> From group experience ..... ‐> many questions & tasks for future research Effect of communication training on ca physicians’ Burnout and work satisfaction (MBI) communication skills training does ameliorate and prevent burnout Where do we go from here? ‐ Refining, improving and differentiating training methods ‐ Research into training process (vs outcomes) ‐ Re‐thinking existing research paradigms & methods ‐ Ensuring benefit for patients‘ experience ........ Patients in crisis ‐ helpful interactions ‘Prescribing the doctor’ ( YOU) can be a powerful tool for giving that support in times of crisis of cancer For patients who are distressed several simple techniques can make your relationship with the patient and family “therapeutic” Patients will be grateful for your support which will also make you feel better Walter Baile Where do we go from here? Without Walter Baile and his dedicated, continued support and effort The KoMPASS group‘s achievements would look quite different We gratefully appreciate his inspiring engagement for our work Looking forward to continuing our fruitful and enjoyable collaboration Thanks for your attention ! www.kompass-o.org