Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
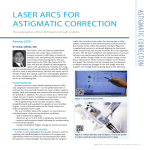
Clinical results of arcuate incisions to correct astigmatism Kurt A. Buzard, MD, Eduardo Laranjeira, MD, Bradley R. Fundingsland, BS ABSTRACT Purpose: To evaluate the effectiveness of arcuate incisions for correcting congenital, post-cataract, post-radial keratotomy, and post-trapezoidal keratotomy astigmatism. Setting: Buzard Eye Institute, Las Vegas, Nevada. Methods: In this retrospective study, 46 eyes of 29 patients had arcuate incisions to correct astigmatism. The average age of patients was 52 years. Results: Mean preoperative astigmatism was 3.51 ± 1.57 D (keratometric) and 3.41 ± 1.44 D (manifest). Mean preoperative uncorrected visual acuity was 20/80, ranging from 20/30 to 20/400. Thirty eyes had a pair of 45-degree arcuate incisions, 10 eyes had a pair of 60-degree arcuate incisions, and 6 eyes had a pair of 90-degree arcuate incisions. Mean follow-up was 6 months. Mean postoperative astigmatism was 1.46 ± 1.07 D (keratometric) and 1.05 ± 0.94 D (manifest), with a reduction of astigmatism in all operated eyes. Mean postoperative uncorrected visual acuity was 20/32, ranging from 20/20 to 20/60. The analysis of the vector astigmatic change showed that only two patients were overcorrected after the procedure. Conclusion: The predictability and safety of arcuate incisions are reflected in these results. J Cataract Refract S u r g 1996; 22:1062-1069 T he common view is that astigmatism can be easily corrected with spectacles or contact lenses. However, even when corrected by these devices, it may cause off-axis blur, eye strain, glare, and visual field restriction. Surgical correction of astigmatism has been attempted since the last century. Transverse keratotomy From the Buzard Eye Institute Las Vegas, Nevada (Buzard, Laranjeira, Fundingsland), Hospital do Servidor Publico Estadual, Department of Ophthalmology, %o Paulo, Brazil (Laranjeira), Department of Surgery-Division of Ophthalmology, University of Nevada, Reno (Buzard), and Department of Ophthalmology, Tulane University Medical Center, New Orleans, Louisiana (Buzard). The authors have no Proprietary or financial interests in any of the devices described. Reprint requests to Kurt Buzard, MD, 6020 Spring Mountain Road, Las Vegas, Nevada 89102. 1062 was suggested by Snellen 1 i n 1 8 6 9 . Lans2 and Sato3 investigated the concept of relaxing incisions. In the 1970s, Trutman and Swinger* introduced and popularized the use of cornea1 relaxing incisions and corneal wedge resection to correct postkeratoplasty astigmatism. In 1982, Ruiz described trapezoidal keratotomy,5 which was explored in a cadaver eye study performed by Lavery and Lindstrom.’ This study indicated that a simple pair of transverse incisions appeared to provide a considerable percentage of the effect of the full Ruiz procedure. Many authors7-‘* have described potential complications of trapezoidal keratotomy, such as microperforations and macroperforations, large postoperative axis shifts, glare, overcorrections, and wound dehiscence. The main disadvantage is the excessive number of incisions in a limited area of the cornea, with subsequent J CATARACT REFRACT S U R G - V O L 22, OCTOBER 1996 XRCUATE INCISIONS FOR ASTIGMATISM cornea1 instability. The same problem has been observed with other modalities of astigmatic surgery, such as the “I,” procedure’ ’ and the Binder” procedure. Arcuate incisions have become popular as a means of correcting moderate and large amounts of astigmatism. Arcuate incisions were first performed to correct astigmatism after penetrating keratoplasty. In 1985, Tchah et al.‘” i’ ntroduced the bowrie procedure, which involves a four-incision radial keratotomy (RK) connected at the limbus by two arcuate incisions straddling the steep axis. This procedure was abandoned because of wound healing problems and block lift in the area in which the radial and arcuate incisions connect. The corneal topographic changes induced by arcuate incisions were first investigated in eye-bank eyes by Tripoli and coauthors.14 The first systematic use of arcuate incisions to correct congenital astigmatism was by M e r l i n , who investigated incisions ranging from 100 to 160 degrees and optical zones ranging from 5 to 7 mm. He found progressive diminished effect as the optical zone was shifted from 5 to 7 mm. The effect on spherical equivalent was null for 100 degree incisions and produced larger hyperopic effects as the incision length increased to 160 degrees. Duffey et al.16 performed a cadaver eye study to evaluate the effectiveness of arcuate incisions and found that longer paired arcuate incisions produced a predictable cornea1 flattening in the meridian centered over the incisions and a smaller cornea1 steepening 90 degrees away, making the procedure ideal for mixed astigmatism. This study presents the clinical results of arcuate incisions performed to correct congenital, post-cataract, post-RK, and post-trapezoidal kcratotomy astigmatism, using the Buzard nomogram.17,1x Few clinical studies of the effectiveness and predictability of astigmatic surgery have been published.‘9-2’ We describe a method that uses shorter and more shallow incisions in the first procedurc. This approach tends to avoid the serious problem of overcorrection while allowing for additional correction on follow-up visits, if necessary. Subjects and Methods Forty-six eyes of 23 patients (17 men and I2 women) had arcuate incisions to correct astigmatism. The surgeries were performed between October 1991 and November 1993. The average age of the pa- tients was 52 years (range 23 to 90 years). The patients had four categories of astigmatism: congenital (28 eyes), post-cataract (15 eyes), post-RK (2 eyes), and post-trapezoidal keratotomy (1 eye). The mean time of astigmatic surgery after cataract extraction was 12 months (range 3 to 36 months). The two cases of arcuate incisions after RK and the only case after trapezoidal keratotomy were performed 5 years after the original procedure. All procedures were performed by one surgeon (K.A.B.). Twenty-three were performed in the operating room and the other 23, at the slitlamp. All enhancement procedures were performed at the slitlamp. Keratometry, photokeratometry, and computed cornea1 topography were performed on all eyes at all preoperative and postoperative visits. Just prior to surgery, the eye was marked at the 12, 6,3, and 9 o’clock limbal positions with a skin marker or needle to prevent surgical problems with eye torsion at the time of the surgery. All cases were performed with topical anesthesia (tetracaine). Pachymetry was done at the locations contemplated for the incisions and the knife was set at 80% of the thinnest reading. A locking lid speculum was used to secure the lids, and an aximeter was used for patient fixation. The steep axis was verified by aligning a Mendez gauge with the previously placed major marks. The arcuatc incisions were marked with the specialized Buzard/Friedlander astigmatic arcuatc markers after they were dipped in methylene blue. The eye was stahilized using a ring fixation without teeth (a Buzard/Thornton ring). Two arcuatc incisions were performed at a 7.0 mm optical zone in all cases. Thirty patients had a pair of 45-degree arcuate incisions, 10 had a pair of 60-degree arcuate incisions, and 6 had a pair of 90-degree arcuate incisions. All surgeries were planned using the Buzard arcuate nomogram (Figure 1), placing incisions in the steep axis. In cases of doubt between two incision lengths, the smaller was chosen. The refraction was expressed in plus cylinder and the surgery performed on the plus cylinder axis. The incisions were made with a front-cutting motion of the knife, using the vertical cutting edge of the diamond. In cases of previous RK, the incisions were “jumped” or placed between the radial incisions. A Thornton 15-degree trifaceted diamond knife was used to perform the incisions. A disposable contact lens was placed on the eye after the procedure and removed that night by the patient. Postoperatively, ARCUATE INCISIONS FOR ASTIGMATISM AGE DEGREE OF ARC ; 1gj .~~~~I~~~~,~!~,, I Figure 1. (Buzard) Buzard nomogram for arcuate incisions at a 7.0 mm optical zone. the patient used antibiotic-steroid drops four times a day and artificial tears every hour while awake. Postoperatively, the undercorrecred eyes were treated by making the incisions deeper and/or longer with enhancement surgery. Twenty-three eyes (50%) had enhancement procedures: 9 had one, 9 had two, and 5 had three. The number of reoperations was higher with longer arcuate incisions. Twelve eyes (40%) with 45-degree atcuate incisions and 6 (60%) with 60degree arcuate incisions had enhancements, but 5 of the 6 eyes (83%) with 9O-degree atcuate incisions had reoperations. Results Mean follow-up after surgery was 6 months (range 2 to 24 months). There was a reduction of both keratometric and manifest astigmatism in all eyes. The mean preoperative keratometric astigmatism was 3.5 1 ± 1.57 diopters (D) (range 1.37 to 8.75 D) and the mean manifest astigmatism, 3.41 ± 1.44 D (range 1.25 to 7.75 D). Before enhancement surgery, the mean postoperative keratometric astigmatism was 1.91 ± 1.60 D (range 0.37 to 9.50 D) and the mean postoperative manifest astigmatism, 1.30 ±1 .OO D (range 0.00 to 5.50 D). After enhancement surgery, the mean postoperative keratometric astigmatism was 1.46 ± 1.07 D (range 0.37 to 6.87 D) (Figure 2) and the mean postoperative manifest astigmatism, 1.05 ± 0.94 D (range 0.00 to 3.00 D) (Figure 3). Analysis of the change in astigmatism achieved by the incisions shows that more astigmatism is corrected with longer incisions. At last follow-up, the mean change in keratometric astigmatism for the 45-, 60-, and 90-degree arcuate incisions was 1.66 ± 0.64 D, 2.69 ± 1.24 D, and 2.83 ±1.04 D, respectively. 1064 0 0 2 4 6 8 10 Preoperative Keratometric Astigmatism (D) -- Figure 2. (Buzard) Preoperative and postoperative keratometric astigmatism. The mean difference between preoperative and final postoperative keratometric axis was 12.3 ± 16.6 degrees (Figure 4), and the mean difference between preoperative and final postoperative manifest axis, 10.7 ± 9.38 degrees [Figure 5). Two patients had axis changes greater than 25 degrees: one had an axis shift of 5 1 keratometric degrees and 50 manifest degrees after a pair of 9O-degree arcuate incisions; the other had an axis shift of 105 degrees (keratometric and manifest) after a pair of GO-degree arcuate incisions. Analysis of the vector astigmatic change (Figure 6) shows that these two patients (4%) were the only cases of overcorrection in this series. J CATARACT REFRACT SURG-VOL 22, OCTOBER 1996 ARCUATE INCISIONS FOR ASTIGMATISM 200 9 g8 0 0 I 0 2 3 4 5 6 7 8 9 0 10 Preoperative Manifest Astigmatism (D) Figure 3. (Buzard) Preoperative and postoperative manifest Figure 5. 50 150 200 100 Preoperative Manifest Axis (degrees) (Buzard) Preoperative and postoperative manifest astigmatism. - I- 0 0 Figure 4. ric axis. 200 150 50 100 Preoperative Keratometric Axis (degrees) 2 4 6 8 10 Preoperative Keratometric Astigmatism (D) (Buzard) Preoperative and postoperative keratomet- Figure 6. (Buzard) Vector astigmatic change. The patients to the right of the dark line are undercorrected and the patients to the left of the dark line are overcorrected. Vector astigmatic change was analyzed using the Holladay/Gravy/Koch formula.22 Roth cases were complicated by problems of wound dehiscence. The average uncorrected visual acuity at last follow-up was 20/32 (range 20/20 to 20/60) (Figure 7). Postoperatively before enhancement surgery, 3 1 eyes J CATARACT REFRACT SURG-VOL 22, OCTOBER 1996 1065 ARCUATF, INCISIONS FOR ASTIGMATISM 0 0 0.2 0.4 0.6 0.8 I 1.2 Preoperative Uncorrected Visual Acuity -6 -6 -4 -2 0 2 4 6 Preoperative Spherical Equivalent (D) J (Buzard) Preoperative and postoperative uncorrected visual acuity. The results are expressed in decimals to facilitate the confection of the graph. Figure 8. (67%) had 20/40 or better acuity. At last follow-up after enhancements, 35 (76%) had 20/40 or better. None of the eyes had a decrease of uncorrected visual acuity after surgery. The best corrected visual acuity remained the same or improved in all eyes. The mean preoperative spherical equivalent was - 0 . 0 9 ± 1.60 D (range -2.50 to +4.25 D) and the mean postoperative spherical equivalent at last followup, -0.27 ± 1.30 D (range -3.00 to +2.50 D) (Figure 8). The mean preoperative keratometrywas 43.65 ± 1.60 D (range 38.18 to 47.43 D) and the mean keratometry after surgery, 43.75 ± 1.80 D (range 38.31 to 47.93 D) (Figure 9). The mean ratio of corneal flattening in the steep meridian to steepening in the flat meridian (F/S ratio) was 0.97 ± 0.9 (range 0.16 to 3.84). With 45-degree arcuate incisions the ratio was 1.05 ± 0.8. With 60- and 9O-degree arcuate incisions, the F/S ratio was 0.81 ± 0.4 and 0.70 ± 0.3, respectively. Three patients had steepening of both steep and flat meridians, and three other patients had flattening of both meridians. Two cases of wound dehiscence were observed. These patients were treated by suturing the wound with 11-O polyester fiber (Mersilene@) interrupted sutures. Final outcome data on these cases are presented after suture correction. We had no other complications such as microperforations and macroperforations, infection, or vascularization of the incisions. Figure 7. 1066 (Buzard) Preoperative and postoperative spherical equivalent. Discussion Astigmatism represents a refractive error that should be analyzed separately from myopia and hyperopia. Ruzard and coauthors” have demonstrated that manifest refraction often underestimates true keratometric astigmatism. In a related study, Lakshminarayanan et aL2* found that a tilted or displaced intraocular lens induced a maximum astigmatism of 0.50 D. These studies support our opinion that most astigmatism in the human optical system resides in the cornea and that, therefore, astigmatic surgery should bc based on keratometry, computed cornea1 topography, or both, instead of on manifest refraction, In cases in which there is a significant difference between manifest and keratometric astigmatism, it is often better to avoid the surgery, which may lead to a complex cross-cylinder effect, creating an astigmatic error at an entirely new axis. 17 J CATARACT REFRACT SURG-VOL 22, OCTOBER 1996 ARCUATE INCISIONS FOR ASTIGMATISM 36 36 38 40 42 44 46 48 50 Preoperative Mean Keratometry (D) Figure g. (Buzard) Preoperative and postoperative mean keratometty. Astigmatic surgery is distinguished from RK in many ways. In RK, the length of the incisions and optical zone are linked (i.e., the longer the incision, the smaller the optical zone), making nomograms very similar. In astigmatic keratotomy, incision length and optical zone are unlinked, resulting in many different nomograms to correct similar amounts of astigmatism. In a recent a r t i c l e 14 experts were asked to give their opinion about correcting astigmatism after cataract surgery. Each proposed a different approach, including transverse incisions, wedge resection, and resuturing the wound. Arcuate incisions have the potential for greater effect because the chord length is the same as straight transverse incisions, but the actual length is about 10% longer on the curve.” Moreover, the length of the incision is equidistant from the center of the cornea, cutting through tissue of approximately equal thickness.5’17 Arcuate incisions are, however, more difficult to perform. To avoid irregularities, the incision must be performed slowly and with a continuous movement, following the curved marks. Hanna et a1.27 have developed an arcuate keratome for performing the incisions with a more uniform and accurate depth. A multiple-puncture tech- I nique has been proposed;l’ it consists of successively deeper incisions to connect multiple punctures when creating arcuate incisions. H a n n a and coauthors28 have found that at an optical zone of 7.0 mm, arcuate transverse incisions show maximal effect at 100 degrees. Because of the potential for cornea1 instability and lack of additional effect, we do not recommend performing arcuate incisions over 100 degrees in length. Another important issue is the incision depth. We believe transverse incisions, whether straight or atcuate, should aim for significantly less than 100% of the thinnest paracentral corneal thickness to avoid the possibility of cornea1 instability, wound gape, and overcorrection. In this study we aimed for 80% depth, which could be deepened later if necessary. Finally, the effect of astigmatic incisions is dependent on age and increases 15% per decade according to the Buzard nomogram and 0.36 D per decade according to Price et aL2’ One wound dehiscence case in this series consisted of a 7O-year-old man with post-cataract astigmatism. He had a pair of 90-degree arcuate incisions and had an axis shift of 50 degrees, with wound dehiscence, which was corrected in the postoperative period with suturing. Although pilocarpine has been discussed as treatment for overcorrections associated with RK,30 it has been observed to worsen astigmatic overcorrections. Because of this case and the findings of the Buzard and Price nomograms, we suggest arcuate incisions be limited to 60 degrees in length in patients older than 60 years. This conservative approach of short, shallow incisions, followed by enhancement if necessary, showed encouraging results and safety when compared with related studies. A reduction in astigmatism was observed in all operated eyes. The effectiveness of the procedure was reflected through the achievement of 20/40 ot better uncorrected visual acuity in 35 eyes (76%) at last follow-up (Figure 7). In a study of 142 eyes, Price et a1.29 achieved a mean postoperative refractive cylinder of 1.22 ± 0.85 D, whereas we achieved 1.30 ± 1.00 D before any enhancement surgery and 1.05 ± 0.94 D after enhancements. With this technique, the majority of patients showed a tendency toward undercorrection. Undercorrection can be managed by enhancing the original surgical procedure-making the incisions deeper, longer, or both-which can be performed at the slitlamp. These J CATARACT REFRACT SURG-VOL 22, OCTOBER 1986 1067 ARCUATE INCISIONS FOR ASTIGMATISM enhancements differ from traditional reopcrations in that no new incisions are made. This enhancement philosophy follows that of the RK “tickle”13 in which incisions are reopened or lengthened for postoperative precision and to avoid overcorrections. Our results demonstrate that the enhancement procedures correct an additional 12% of keratometric astigmatism and an additional 7% of manifest astigmatism without additional complications. Overcorrection is a much more serious problem. It leads to diminished best corrected vision, glare, diurnal variation, and wound dchisccnce. A new set of incisions in the opposing axis must be made to correct significant overcorrections. Analysis of the vector astigmatic change in this study revealed two patients (4%) with overcorrections (Figure 6). The overcorrections were due to the two large axis shifts of 50 and 105 degrees, complicated by wound dehiscence problems. This 4% incidence is lower than the 18% reported by Price et a1.29 and 19% reported by Neumann and coauthors.“z In addition, the mean coupling ratio of 0.97 (F/S) demonstrates less flattening than the 1.47 ratio reported by Duffey et al.,33 the 1.0 reported by Merlin,15 and the 2.0 reported by Lundergan and Rowsey.“* Arcuate incisions couple in a more unpredictable manner, preserving spherical equivalent in some cases and making the patient more myopic or hyperopic in other cases (Figures 8 and 9). At a 7.0 optical zone with longer arcuate incisions (60 and 90 degrees), there is a tendency to make the cornea slightly steeper, which is supported by coupling ratio data in this and other studies.28S34 For this reason, we recommend that astigmatic corrections larger rhan 3.00 D be performed prior to RK to determine the actual spherical correction needed after astigmatic surgery. In summary, arcuatc incisions may be an effective treatment of astigmatic patients who do not have satisfactory results with spectacles or contact lenses. A conservative approach, making the incisions shallow and short, and deepening or extended later, eliminates a large amount of corneal astigmatism and tends to avoid the number of overcorrections observed with other techniques. References 1. Snellen H. Die richtung der Haupcmcridiane des astigmatischen Auges. Albrecht von Graefe Arch Ophthalmol 1869; 15(II):199-207 1068 2. Lans LJ. Experimentelle Untersuchungen über Entstehung von Astigmatismus durch nicht-perforirende Corneawunden. Albrecht von Graefe Arch Ophthalmol 1898; 45:117-152 .3 . Sato T. Posterior half-incision of the cornea for astigmatism; operative procedures and results of the improved tangent method. Am J Ophthalmol 1953; 36:462-466 4. Troutman RC, Swinger C. Relaxing incision for control of postoperative astigmatism following keratoplasty. Ophthalmic Surg 1380; 1 1 : I I 7-I 20 5. Binder PS, Waring GO III. Keratotomy for astigmatism. In: Refractive Keracotomy for Myopia and Astigmatism. St Louis, Mosby Yearbook, 1992; 1090-l 134 6. Lavery CW, Lindstrom RL. Trapezoidal astigmatic keratotomy in human cadaver eyes. J Refract Surg 1985; 1:18-24 Villasefior RA, Stimac GR. Clinical results and compli7. cations of trapezoidal keratotomy. J Refract Surg 1988; 4:125-131 8. Buzard KA, Haight D, Troutman R. Ruiz procedure for post-keratoplasty astigmatism. J Refract Surg 1987; 3:40-45 9. Merck MP, Williams PA, Lindstrom RL. Trapezoidal keratotomy; a vector analysis. Ophthalmology 1986; 93: 719-726 10. Lavery GW, Lindstrom RL. Clinical results of trapezoidal astigmatic ketatotomy. J Refract Surg 1385; 1.70-74 11. Schachar RA. Indications, techniques, and complications of radial keratotomy. Int Ophthalmol Clin 1983; 23(3): 119-128 12. Franks JU, Binder 1’s. Keratotomy procedures for rhc correction of astigmatism. J Refract Surg 1985; 1:l l-17 13. Tchah H, Hofmann RF, Duffey RJ, et al. Delimited peripheral arcuate kcratoromy for asrigmarism: “bowcie” configuration. J Refract Surg 1388; 4: 1 X3-1 90 14. Tripoli NK, Cohen KL, Holman KE. Cornea1 topographic response to circumferential keratotomies. J Refract Surg 1987; 3:129-136 Merlin U. Curved keratotomy procedure for congenital 15. astigmatism. J Refract Surg 1987; 3:92-97 16. Duffey RJ, Jain VN, Tchah H, et al. Paired arcuate keratotomy; a surgical approach to mixed and myopic astigmatism. Arch Ophthalmol 1988; 1 O&l 130-l 135 17. Troutman RC, Ruzard KA. Cornea1 Astigmatism; Etiology, Prevention, and Management. St Louis, Mosby Yearbook, 1992; 11 X-l 36 18. Ruzard KA. Prevention of post-cataract astigmatism. Highlights of Ophthalmology Letter 1992; 20(8):56-62 19. Lindstrom KL. The surgical correction of astigmatism: a clinician’s perspective. Refract Cornea1 Surg 1990; 6:441-454 20. Buzard KA. Paired relaxing incisions for the control of astigmatism. Cornea 1991; 10:3X-43 21. Buzard KA, The surgical management of astigmatism. In: T CATARACT REFRACT SI!RG--vOI. 22. 0C~C)kX.K 1996 ARCUATE LNCISIONS FOR ASTIGMATISM 22. 23. 24. 25. 26. 27. 28. Selser RE Jr, ed, Medical Cornea: Corneal and Refractive Surgery (Proceedings of the 42nd Annual Symposium of the New Orleans Academy of Ophthalmology). Amsterdam, New York, Kugler 1993; 87-99 Holladay JT, Cravy TV, Koch DD. Calculating the surgically induced refractive change following ocular surgery. J Cataract Refract Surg 1992; 18:429-443 Buzard K, Shearing S, Relyea R. Incidence of astigmatism in a cataract practice. J Refract Surg 1988; 4:173-178 Lakshminarayanan V, Enoch JM, Raasch T, et al. Refractive changes induced by intraocular lens tilt and longitudinal displacement. Arch Ophthalmol 1986; 104:90-92 Thornton SP. Correction of astigmatism after cataract surgery. Refract Cornea1 Surg 1990; 6:131-136 Thornton SP. Astigmatic keratotomy: a review of basic concepts with case reports. J Cataract Refract Surg 1990; 16:430-435 Hanna KD, Hayward JM, Hagen KB, et al. Keratotomy for astigmatism using an arcuate keratome. Arch Ophthdmol1993; 111:998-1004 Hanna KD, Jouve FE, Waring GO III, Ciadet PG. Com- I puter simulation of arcuate keratotomy for astigmatism. Refract Corneal Surg 1992; 8: 152-l 63 29. Price FW, Grene RB, Marks RG, et al. Astigmatism reduction clinical trial: a multicenter evaluation of the predictability of arcuate keratotomy; evaluation of surgical nomogram predictability. Arch Ophthalmol 1995; 113: 277-282 30. Laranjeira E, Buzard KA. Pilocarpine in the management of overcorrection after radial keratotomy. J Refract Surg 1996; 12:382-390 3 1. Buzard KA. Deepening of incisions after radial keratntomy using the “tickle” technique. Refract Corneal Surg 1991; 7:348-355 32. Neumann AC, McCarty GK, Sanders DR, Raanan MG. Refractive evaluation of astigmatic keratotomy procedures. J Cataract Refract Surg 1989; 15:25-31 33. Duffey RJ, Jain VN, Tchah H, et al. Paired arcuate keratotomy; a surgical approach to mixed and myopic astigmatism. Arch Ophthalmol 1988; 106:1130-l 135 34. Lundergan MK, Rowsey JJ. Relaxing incisions; cornea1 topography. Ophthalmology 1985; 92: 1226-1236 J CATARACT REFRACT SURG-VOL 22, OCTOBER 1996 1069