Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
ISIE Imaging Conference
Saturday, May 3, 2014
8:30-5:30 pm
Orlando, Florida
Orange County Convention Center, South Building
Paper Sessions
S 310A - D
Posters & Exhibits
S 310E - H
Table of Contents
Program Organizers/Committee.............................................................................................1
Program Information................................................................................................................3
Conflict of Interest Disclosures…............................................................................................5
Agenda .......................................................................................................................................7
Presentations
Retinal Imaging........................................................................................................................19
Functional Retinal Imaging…………………………………………………………………31
Glaucoma / Anterior Eye……………………………………………………………………43
Novel methods for Small Animal Imaging………………………………………………..58
Posters...................................................................................................................................68
Program Organizers
James G. Fujimoto, PhD
Dept. of Electrical Engineering &
Computer Science
Massachusetts Inst of Technology
Cambridge, Mass.
Joel S. Schuman, MD, FARVO
UPMC Eye Center/Univ of Pittsburgh
Pittsburgh, Penn.
Wolfgang Drexler, PhD
Center for Medical Physics &
Biomedical Engineering
Medical University Vienna
Vienna, Austria
Program Committee Members
Bruce Berkowitz, PhD, FARVO
Anatomy/Cell Biology & Ophthalmology
Wayne State University School of
Medicine
Joachim Hornegger, PhD
Pattern Recognition Laboratory
Friedrich-Alexander University
Erlangen-Nuremberg
Joseph Carroll, PhD
Medical College of Wisconsin
Milwaukee, Wisc.
Joseph A. Izatt, PhD
Biomedical Engineering Dept
Duke University
Brad Fortune, OD, PhD
Discoveries in Sight Research
Laboratories
Legacy Research Institute
Devers Eye Institute
Jost Jonas, MD, FARVO
Faculty of Clinical Medicine
Heidelberg University
Giovanni Gregori, PhD
U Miami
Bascom Palmer Eye Institute
Fabrice Manns, PhD
Ophthalmic Biophysics Center
Bascom Palmer Eye Institute
1
Ronald Silverman, PhD
Columbia University Medical Center
Richard Spaide, MD
Vitreous Retina Macula Consultants NY
Susan Vitale, PhD, FARVO
Division of Epidemiology & Clinical
Applications
National Eye Inst/NIH
John S. Werner, PhD, FARVO
Dept. of Ophthalmology
University of California Davis Medical
Center
Yoshiaki Yasuno, PhD
Institute of Applied Physics
University of Tsukuba
Linda M. Zangwill, PhD, FARVO
Shiley Eye Center
University of California‐San Diego
2
Program information
Optical imaging is a noninvasive, non-contact technology that can image ocular structures in vivo. The
anatomic layers of the eye can be differentiated and measured, by some technologies at a cellular or
subcellular level. The resulting images can be extremely useful in basic understanding of disease and its
pathogenesis, normal physiology and the diagnosis and follow-up of diseases affecting the eye, including
glaucoma and age-related macular degeneration. Unfortunately, knowledge on imaging technologies is
limited and evolving. Needs for this course are based on recent literature and expert opinion.
Participants can expect to be exposed to the most up-to-date information regarding ocular imaging and
its applications. The objective of the course is to enhance competence in this field and to advance the
science of imaging. Clinical practice will improve through the implementation of strategies defined in
this session.
Course Format
The ARVO/ISIE Imaging conference is a forum for the presentation of current clinical and basic science
advances in glaucoma, retina, cornea, anterior segment, orbit and neuro-imaging in ophthalmology.
Didactic paper presentations will be followed by poster presentations.
Course Highlights
This is your chance to hear original research on current advances, as well as state-of-the-art technology
in ophthalmic imaging. This critical and informative research will help you further your practice and
better care for your patients.
Learn scientific principles behind ophthalmic imaging
Discuss clinical applications of imaging technologies
Explore new research and recent advances in imaging
Who Should Attend
Clinicians
Scientists
Engineers
Regulators
Learning Objectives
Upon completion of this educational activity, participants will be able to:
Review new advances in ophthalmic imaging
Describe clinical applications of imaging technologies in ophthalmology
Explain the importance of ophthalmic imaging
Discuss imaging in glaucoma, retinal disease, corneal pathologies and neuro-ophthalmology
3
Disclosure Policy
It is the policy of ARVO to ensure balance, independent objectivity, and scientific rigor in all its
sponsored educational programs. All faculty and planning committee members participating in
continuing medical education activities are required to disclose to the program audience any real or
apparent conflict of interest related to the content of their presentations.
In accordance with the ACCME's Standards for Commercial Support of Continuing Medical Education, all
faculty and planning committee members must disclose any relevant financial relationship(s) or other
relationship(s) held within the past 12 months. ARVO implements a mechanism to identify and resolve
all conflicts of interest prior to delivering the educational activity to learners.
Disclaimer
ARVO Education Courses provide a forum for the open exchange and discussion of research results and
scientific advancements in the field of ophthalmology; however, ARVO makes no representation or
warranty as to the truth, originality, or accuracy of the information presented at the courses or in
materials distributed in connection with them. Nor are the views expressed by the individual speakers
necessarily the views of ARVO. ARVO supports the ACCME’s policy on evidence-based content and
encourages faculty to adhere to these standards when planning a presentation.
Audio and Video Recording of Sessions/Workshops
Recording by any means (photographing, audiotaping or videotaping) of any presentations or sessions at
any ARVO Meeting is prohibited, except by an ARVO-authorized agent for official purposes or by First
Authors who wish to photograph their own poster presentations. Violators risk confiscation of their
equipment and/or dismissal from the meeting as deemed appropriate by ARVO.
Certificate of Attendance
Certificates of Attendance are available to all participants. Attendees must complete an online
evaluation form to receive a Certificate of Attendance. Attendees who preregistered for the conference
by Monday, April 28, 2014, can submit the evaluation upon completion of the course. All others may
access the system beginning Wednesday, May 14, 2014.
http://www.planion.com/Web.Admin/Login?Account=ARVO.
Use your ARVO ID and Password, or click “forgot your password” to log in. Select and evaluate the
course you attended, then print or email your Certificate of Attendance.
This activity does not offer AMA PRA Category 1 Credits™.
4
Financial Relationships Disclosures
It is the policy of the ARVO that all faculty and planning partners disclose conflicts of interests relating to
the topics of this educational activity. Faculty members and the planning committee are required to
disclose to the learners any relevant financial relationship(s). ARVO considers relationships of the person
involved in the CME activity to include financial relationships of a spouse or partner, or a dependent
child.
The following faculty members have stated they have no financial relationships to disclose.
Bruce Berkowitz, PhD
Joseph Carroll, PhD
John S. Werner, PhD
Susan Vitale, PhD
The following faculty members have stated their financial relationship(s):
Wolfgang Drexler, PhD- Zeiss (C)
Brad Fortune, OD, PhD- Heidelberg Engineering, GmbH, Carl Zeiss Meditec, Inc (F)
James Fujimoto, PhD- Carl Zeiss Meditec, Optovue (P); Optovue (I)
Giovannni Gregori, PhD- Carl Zeiss Meditec (F), (P)
Joachim Hornegger- Optovue Inc. (P)
Joseph Izatt- Bioptigen, Inc. (I), (P), (S)
Jost Jonas, MD- Allergan Inc., Merck Sharp & Dohme Co, Alimera Co, Boehringer Ingelheim Co,
Sanofi Co (C), CellMed AG, Alzenau, Germany (P)
Fabrice Manns, PhD- Bioptigen (F)(P)
Joel S. Schuman, MD- Carl Zeiss Meditec (P)
Ronald Silverman, PhD- Arcscan, Inc. (I)
Rick Spaide, MD- Topcon (P)(C); TEVA Pharmaceuticals (C)
Yoshiaki Yasuno- Topcon Corp. (F); Tomey Corp. (F), (P); Nidek (F)
Linda Zangwill, PhD- Carl Zeiss Meditec Inc., Heidelberg Engineering GmbH, Optovue Inc, Topcon
Medical Systems, Nidek Inc (F)
Financial Relationships Disclosure Codes Key:
F (Financial Support) Indicates if you have received through your employing institution support from a
for-profit company, or competing company, in the form of research funding, grants or research
materials or services (e.g., protein sequencing) at no cost, such support being the subject matter of your
presentation or publication.
I (Personal Financial Interest) Indicates if you are an investor in a company or competing company, other
than through a mutual or retirement fund, which provides a product, service, process or equipment that
is the subject matter of your presentation or publication.
5
E (Employment) Indicates if you are an employee of a company or competing company with a business
interest that is the subject matter of your presentation or publication.
C (Consultant) Indicates if you are, or have been within the last 24 months prior to date of submission, a
consultant for a company or competing company with a business interest that is the subject matter of
your presentation or publication.
P (Patent) Indicates if you are an inventor/developer designated on a patent, patent application,
copyright, or trade secret, whether or not the patent, copyright, etc. is presently licensed or otherwise
commercialized, which is the subject matter of your presentation or publication or could be in
competition with the technology described.
R (Recipient) Indicates if you have received gifts in kind, honoraria or travel reimbursement valued in
any amount in the last twelve months from a company or competing company which provides a
product, service, process or equipment that is the subject matter of your presentation or publication.
N (No Commercial Relationship) Indicates there is no commercial relationship relevant to the subject
matter of the abstract/article/presentation.
S (non-remunerative) Indicates you have position(s) of influence such as officer, board member, trustee,
spokesperson, etc.
6
ISIE Imaging Conference
Saturday, May 3, 2014
Orlando, Florida
Orange County Convention Center, South Building
Paper Sessions
S 310A - D
8:00am – 5:30pm
Posters & Exhibits
S 310E - H
8:00am – 4:00pm
Poster Presentations: 10:00-10:30am, 12:00-1:30pm, 3:30-4:00pm
Conference Agenda
7:00 am
Registration
7:50 am
Opening Remarks
8:00 - 10:00 am
Retinal Imaging
Moderator(s): James Fujimoto, PhD; Wolfgang Drexler, PhD; Joel Schuman,
MD
8:00 -08:15 am
Program Number 1: Improved Visualization of the Vitreous using
Swept Source Optical Coherence Tomography with Dynamic Focus
Sweeping
Richard Spaide, Charles Reisman , Zhengo Wang, Kinpui Chan
7
08:15 -08:30 am
Program Number 2: Choroidal, Haller’s and Sattler’s thickness analysis
across different age related macular degeneration phenotypes imaged
with 3D-1060nm-OCT
Marieh Esmaeelpour, Siamak Ansari-Shahrezaei, Behrooz Zabihian, Martin F
Kraus, Maximilian Gabriel, Ilse Krebs, Joachim Hornegger, Carl Glittenberg,
Wolfgang Drexler, Susanne Binder
08:30 -08:45 am
Program Number 3: Effects of optical opacity on retinal cone counts
measured by a narrow angle Heidelberg Retina Angiograph
Roger Anderson, Marketa Cilkova, Padraig Mulholland, Juliane Matlach, Nilpa
Shah, Tony Redmond, David Garway-Heath, Steven Dakin
08:45 -09:00 am
Program Number 4: Autofluorescent droplets in the sub-Retinal
Pigment Epithelium (RPE)-space of eyes with age-related macular
degeneration (AMD): ex vivo imaging
Thomas Ach, Christine A. Curcio
09:00 -09:15 am
Program Number 5: High resolution imaging of Gunn’s dots
Michel Paques, Edouard Koch, Celine Chaumette, Alexandre Leseigneur
09:15 -09:30 am
Program Number 6: Detection of Retinal Blood Flow Turbulence at
Arteriovenous Crossings using Spectral Domain Optical Coherence
Tomography
Michael Larsen
9:30 -09:45 am
Program Number 7: Ganglion Cell Analysis using High-Definition
Optical Coherence Tomography in Patients with mild cognitive
impairment and Alzheimer’s Disease
Carol Y. Cheung, Yiting Ong, M. Kamran Ikram, Christopher Chan, Tien Yin
Wong
09:45 -10:00 am
Program Number 8: Automatic Analysis of Color Retinal Images for
CMV Retinitis Screening
Sandeep Bhat, Chaithanya Ramachandra, Todd P. Margolis, Jeremy Keenan,
Kaushal Solanki
10:00-10:30 am
Break and Posters/Exhibits
10:30 - 12:00 pm
Functional Retinal Imaging
Moderator(s): Wolfgang Drexler, PhD; Richard Spaide, MD
8
10:30-10:45 am
Program Number 9: Optical Coherence Tomography Angiography of
Macular Disease
David Huang, Yali Jia, Steven T. Bailey, Thomas Hwang, Andreas K. Lauer,
Christina J. Flaxel, Mark E. Pennesi, David J. Wilson, Joachim Hornegger, James
G. Fujimoto
10:45-11:00 am
Program Number 10: En Face Visualization of Retinal Pathologies
Using Ultrahigh Speed Swept Source Optical Coherence Tomography
Woo Jhon Choi, Mehreen Adhi, Eric Moult, ByungKun Lee, Zhao Wang, Martin
F. Kraus, Jay S. Duker, Joachim Hornegger, James G. Fujimoto, Nadia K.
Waheed
11:00-11:15 am
Program Number 11: Quantitative Insights into Macular
Microvascularity using Adaptive Optics Scanning Light
Ophthalmoscopy Fluorescein Angiography
Richard Rosen, Alexander Pinhas, Moataz Razeen, Nishit Shah, Alexander Gan,
Richard Bavier, Rishard Weitz, Joseph Carroll, Alfredo Dubra, Yuen Ping T.
Chui
11:15-11:30 am
Program Number 12: Quantification of Absolute Number of
Photoreceptors from Ultra-Widefield Imaging
Daniel E. Croft, Charles C. Wykoff, David M. Brown, Jano VanHemert
11:30-11:45 am
Program Number 13: Parafoveal cone hyporeflectivity and recovery
seen by adaptive optics in posterior uveitis
Phoebe Lin, Kristin Biggee, Michael Gale, Eric Suhler, Mark Pennesi
11:45-12:00 pm
Program Number 14: Total Retinal Blood Flow Measurement with 70k
Hz Spectral Domain OCT
Ou Tan, Gangjun Liu, Yali Jia, David Huang
12:00-1:30 pm
Lunch and Posters/Exhibits
1:30 - 3:30 pm
Glaucoma / Anterior Eye
Moderator(s): Brad Fortune, PhD; Susan Vitale, PhD
1:30-1:45 pm
Program Number 15: Evaluation of the Spatial Relationship Between
Glaucoma Progression using Confocal Scanning Laser
Ophthalmoscopy (CSLO), Optical Coherence Tomography (OCT), and
Visual Field (VF)
Dingle Foote, Gadi Wollstein, Divya Narendra, Yun Ling, Richard A. Bilonick, Hiroshi
Ishikawa, Larry Kagemann, Cynthia Mattox, James G. Fujimoto, Joel S. Schuman
9
1:45-2:00 pm
Program Number 16: Identification of Glaucoma using Biomarkers of
Retinal Vascular Morphology and Blood Flow Computed from Retinal
Fundus Images
David Meadows, Rick Clark, Daniel Dickrell
2:00-2:15 pm
Program Number 17: Measurement of BMO plan-based anterior lamina
cribrosa surface depth (ALCSD) parameter using a deconvolution
approach applied to 3D spectral domain optical coherence tomography
optic nerve head images
Akram Belghith, Christopher Bowd, Zhiyong Yang, Felipe Medeiros, Robert N.
Weinreb, Linda M. Zangwill
2:15-2:30 pm
Program Number 18: Magic Angle-Enhanced MRI of Fibrous
Structures in the Eye upon Intraocular Pressure Loading
Leon C. Ho, Ian A. Sigal, Ning-Jiun Jan, Alexander Squires, Zion Tse, Ed X.
Wu, Seong-Gi Kim, Joel S. Schuman, Kevin C. Chan
2:30-2:45 pm
Program Number 19: Accuracy of a Method for Measuring MicronScale Collagen Fiber Orientation
Ning-Jiun Jan, Jonathan L. Grimm, Bo Wang, Kira Lathrop, Huong Tran, Gadi
Wollstein, Larry Kagemann, Hiroshi Ishikawa, Joel Schuman, Ian A. Sigal
2:45-3:00 pm
Program Number 20: Automated identification of Schlemm’s canal and
collector channels from spectral domain optical coherence tomography
images.
Siamak Yousefi, Amir Marvasti, Robert N. Weinreb, Christopher Bowd, Alex
Huang
3:00-3:15 pm
Program Number 21: Functional Microvascular Imaging of the
Conjunctiva: a noninvasive tool to measure and quantify subtle
variations and abnormalities in the microvasculature
Delia Cabrera DeBuc, Hong Jiang, Nicole Stuebiger, Che Liu, Tian Jing, Gabor
Mark Somfai, Janet Davis, William E. Smiddy, Jianhua Wang
3:15-3:30 pm
Program Number 22: Ultra-High Resolution Optical Coherence
Tomography for the Differentiation of Ocular Surface Squamous
Neoplasia and Melanoma
Juan Murillo, Anat Galor, Afshan A. Nanji, Madhura G. Joag, James R. Wong,
Nabeel M. Shalabi, Marwan Atallah, Ibrahim Sayed-Ahmed, Carol L. Karp
3:30-4:00 pm
Break and Posters/Exhibits
10
4:00 - 5:30 pm
Novel Methods for Small Animal Imaging
Richard Rosen, MD; Moderator(s): Yoshiaki Yasuno, PhD
4:00-4:15 pm
Program Number 23: Two-photon imaging of inner and outer retina in
the living primate eye
Robin Sharma, David R. Williams, Grazyna Palczewska, Krzysztof Palczewski,
Jennifer Hunter
4:15-4:30 pm
Program Number 24: 3D-imaging of Rat Retina Using Contrast
Enhanced X-ray Microtomography
Kalle Lehto, Ilmari Tamminen, Soile Nymark, Tanja Ilmarinen, Hannu Uusitalo,
Heli Skottman, Antti Aula, Jari Hyttinen
4:30-4:45 pm
Program Number 25: The Influence of Metabolism on Retinal OCT
Imaging: What We've Learned from a Hibernating Animal Model
Brent A. Bell, Yichao Li, Fengyu Qiao, Haohua Qian, Joe G. Hollyfield, Wei Li
4:45-5:00 pm
Program Number 26: Spatial relationship between retinal loss and
neurodegeneration of the visual system using optical coherence
tomography (OCT) and diffusion tensor MR imaging (DTI)
Bo Wang, Leon C. Ho, Ian P. Conner, Richard A. Bilonick, Hiroshi Ishikawa,
Amanda Woodside, Chieh-Li Chen, Gadi Wollstein, Joel S. Schuman, Kevin C.
Chan
Program Number 27: Engineering of Gold Nanorods for ContrastEnhanced Retinal OCT
Andrew Gordon, Jason Craft, Ashwath Jayagopal
5:00-5:15 pm
5:15-5:30 pm
Program Number 28: The Effect of Microtubule-stabilizing Agents on
the Retinal Ganglion Cell Axons Studied by Second-Harmonic
Generation Microscopy
Hyungsik Lim, John Danias
11
Poster Presentations
10:00 - 10:30 am
12:00 - 1:30 pm
3:30 - 4:30 pm
Poster Presentations
Poster Board Number P1:
Applications of photoacoustic tomography to imaging and estimation of oxygen saturation of
hemoglobin in ocular tissue of rabbits
K.Chan; Z. Tse; T.B. Pirkle; A. Squires; N. Jan; G. Wollstein; J. Schuman; S. Kim; I.A. Sigal
Poster Board Number P2:
Quantitative MRI-derived optic nerve microstructural features in a feline glaucoma model
Gillian J. McLellan, Samuel A. Hurley, Pouria Mossahebi, Norman M. Ellinwood, Aaron S. Field
Poster Board Number P3:
Analysis of the Cellular Dynamics of LysM-Positive Cells in a Corneal Suture Mouse Model
using Intravital Imaging
Mayumi Ueta, Ayaka Koga, Masaru Ishii, Shigeru Kinoshita
Poster Board Number P4:
Optical coherence tomography imaging to assist the iMvalv prototype development.
Rodrigo M. Torres, Diego Ramirez Arduh, Fabio A. Guarnieri
Poster Board Number P5:
MRI, CT, and UBM imaging after corneal and cataract surgery
Sotiria Palioura, James Chodosh, Lois Hart, Karen Capaccioli, Daniel Ginat, Suzanne Freitag
Poster Board Number P6:
Rates of Glaucoma Progression as Detected by Optical Coherence Tomography (OCT) and
Heidelberg Retinal Tomography (HRT) in a Long-Term Cohort
Divya Narendra, Gadi Wollstein, Dingle Foote, Yun Ling, Richard A. Bilonick, Hiroshi Ishikawa, Larry
Kagemann, Cynthia Mattox, James G. Fujimoto, Joel S. Schuman
Poster Board Number P7:
Estimation of Trabecular Meshwork Thickness by Area and Width Measurements
Larry Kagemann, Hiroshi Ishikawa, Gadi Wollstein, Bo Wang, Yun Ling, Richard A. Bilonick, Joel S.
Schuman
12
Poster Board Number P8:
Predicting Future Observations of Functional and Structural Measurements in Glaucoma
Using a Two-Dimensional State-based Progression Model
Yu-Ying Liu, Hiroshi Ishikawa, Gadi Wollstein, Richard A. Bilonick, James G. Fujimoto, Cynthia
Mattox, Jay S. Duker, Joel S. Schuman, James M. Rehg
Poster Board Number P9:
Assessment of retinal nerve fiber layer with color and red free images using Smartscope
Fundus Camera
Ramesh S Ve, Krithica Srinivasan
Poster Board Number 10:
Confocal microscopy for the analysis of the sub-basal corneal nerves
Madhura G. Joag, Anat Galor, Nabeel M. Shalabi, James R. Wong, Juan Murillo, Afshan A. Nanji,
Marwan Atallah, Parke Green, Mauro Campigotto, Carol L. Karp
Poster Board Number 11:
Role of Ultra High Resolution Optical Coherence Tomography (UHR-OCT) in the Diagnosis
of Ocular Surface Squamous Neoplasia (OSSN) in Complex Ocular Surface Diseases
Marwan Atallah, Guillermo Amescua, Anat Galor, Juan Murillo, Madhura G. Joag, James R. Wong,
Nabeel M. Shalabi, Afshan A. Nanji, Carol L. Karp
Poster Board Number 12:
Noncontact direct observation of the human cornea by in vivo confocal microscopy with a
high-power objective lens
Kaori Ideguchi, Eriko Abe, Taiichiro Chikama, Yuko Kadohiro, Takashi Sone, Ryotaro Toda, Sosuke
Inokawa, Yoshiaki Kiuchi
Poster Board Number P13
Analysis of the cornea densitometry using Pentacan with different illuminance
Fernando Abib, Mariele A. Maximo, Andre Heck
Poster Board Number P14:
OptoVue OCT as an imaging modality of scleral thickness following fluocinolone acetonide
implant
Kristin Biggee, Nicholas Schubach, Eric Suhler, Christina J. Flaxel
Poster Board Number P15:
Posterior capsular opacification in intraocular hydrophilic lenses compared to hydrophobic
intraocular lenses using Scheimpflug images
Arturo Olguin-Manriquez, Efrain Romo-Garcia, David Magana
13
Poster Board Number P16:
Morphologic Changes In Angle Closure Glaucoma After Iridotomies Documented by
Ultrabiomicroscopy
Efrain Romo-Garcia, Nicolas Corona-Osuna, Silvia Lizarraga, David Magaña, arturo OlguinManriquez, Miguel Piña, Felipe Esquivel, Arturo Ramirez-Mondragon, Felipe Peraza-Garay
Poster Board Number P17:
Ocular Surface Health In Patients With Rheumatoid Arthritis In India
Ramya Ravindran
Poster Board Number P18:
Improving the processing and analysis workflow of adaptive optics retinal imaging
Benjamin Sajdak, Robert F. Cooper, Kathleen Bazan, Brian Higgins, Drew Scoles, Melissa Wilk, Alfredo
Dubra, Joseph Carroll
Poster Board Number P19:
Clinical Assessment and Single Cell imaging in Unexplained Vision Loss
Philip Severn, Adam M Dubis, Robert F. Cooper, Joseph Carroll, Alfredo Dubra, Ganeshan K Ramsamy,
Fred W Fitzke, Gary Rubin, Cathy Egan, Michel Michaelides
Poster Board Number P20:
High-resolution En face images of microcystic macular edema in patients with autosomal
dominant optic atrophy
Shuhei Kameya, Kiyoko Gocho, Sachiko Kikuchi, Kei Shinoda, Atsushi Mizota, Kunihiko Yamaki, Hiroshi
Takahashi
Poster Board Number P21:
Magnetic resonance imaging findings of the subretinal space in bilateral congenital retinal
detachments in Norrie’s syndrome
Rocio I. Diaz, Eric J. Sigler, Asim F. Choudhri, Jorge I. Calzada
Poster Board Number P22:
Fluorescence Lifetime Measurement in Central Artery Occlusion
Chantal Dysli, Sebastian Wolf, Martin S. Zinkernagel
Poster Board Number P23:
Brownian Motion Imaging With Optical Coherence Tomography and Optical Coherence
Tomography Angiography
Gangjun Liu, Yan Li, Yali Jia, David Huang
Poster Board Number P24:
Histogram Matching Extends Acceptable Signal Strength (SS) Range on Optical Coherence
Tomography (OCT) Images
Chieh-Li Chen, Hiroshi Ishikawa, Gadi Wollstein, Richard A. Bilonick, Ian A. Sigal, Larry Kagemann,
JoelS.Schuman
14
Poster Board Number P25:
Effect of Scanning Incident Angle (IA) on Total Retinal Thickness (TRT) Measurement With
A Phantom Eye Using Spectral-Domain Optical Coherence Tomography (SD-OCT)
Hiroshi Ishikawa, Chieh-Li Chen, Jigesh Baxi, Anant Agrawal, Daniel X. Hammer, Gadi Wollstein,
Richard A. Bilonick, Ian A. Sigal, Larry Kagemann, Joel S. Schuman
Poster Board Number P26:
Modeling the topography of the healthy human retina
Rui Bernardes, Silvia Simão, Ana S. C.Silva, Angelina Meireles, João Figueira
Poster Board Number P27:
Preliminary evaluation of a prototype metabolic hyperspectral retinal camera in age related
macular degeneration patients
Jean-Philippe Sylvestre, Rachel Trussart, Jean Daniel Arbour
Poster Board Number P28:
Quantitative autofluorescence (qAF) in pseudophakic normal and dry Age-related macular
degeneration (AMD) patients
Camellia Nabati, Jonathan Greenberg, Dan Yoon, Elana Rosenberg, David Sackel, Roland Smith
Poster Board Number P29:
Comparison of Fundus Autofluorescence Imaging by 488 nm and 532 nm Confocal Scanning
Laser Ophthalmoscopy in Central Serous Chorioretinopathy
Seong-Woo Kim, Jaeryung Oh, Cheol Min Yun, Kuhl Huh
Poster Board Number P30:
Cone photopigment distribution measured using green autofluorescence imaging
Kanako Itagaki, Kimihiro Imaizumi, Akira Ojima, Tetsuju Sekiryu
Poster Board Number P31:
Fundus Autofluorescence to Identify Plaques and Diagnose and Follow Retinal Artery
Occlusions
Yannis M. Paulus, Aazim Siddiqui, Adrienne W. Scott
Poster Board Number P32:
Infrared and Fundus Autofluorescence Imaging in the Evaluation and Monitoring of
Peripheral Retinoschisis
Timothy Kao, Sandra R. Montezuma, Dara Koozekanani, Philip Turner, Torey Miller
Poster Board Number P33:
False Negatives in the Delineation of Age-related Geographic Atrophy by Fundus
Autofluorescence
David J. Ramsey, Carol Applegate, Janet S. Sunness
15
Poster Board Number P34:
Inexpensive 3D Telemedicine: Integrating smartphone technologies in an ophthalmological
stereoscopic evaluation
Jorge-Emmanuel Morales-León
Poster Board Number P35:
Fundus mask and lens dust detection in retinal images with applications to automated
diabetic retinopathy screening
Kaushal Solanki, Malavika Bhaskaranand
Poster Board Number P36:
Non mydriatic hand held camera -An effective screening tool for diabetic population in
hands of paramedical health workers.
Sundaram Natarajan, Purva Valvekar, Deepen Sheth, Sunita Mohan, Radhika Krishnan, Pandurang
Kulkarni
Poster Board Number P37:
Hand-held non-mydriatic digital fundus imaging for the detection of diabetic retinopathy
Steven R. Cohen, Grace E. Boynton, Cagri G. Besirli, Maria A. Woodward, Paula Anne Newman-Casey
Poster Board Number P38:
Can Heidelberg MultiColor images be used interchangeably with color fundus photography
for grading age-related macular degeneration features?
Katie Graham, Patrick Larkin, Katherine Alyson Muldrew, Vittorio Silvestri, Graham Young, Philip
McIntyre, Helen McAtamney, Ruth E. Hogg
Poster Board Number P39:
Ultra high resolution imaging of subepithelial ocular pathologies
James R. Wong, Madhura G. Joag, Afshan A. Nanji, Juan Murillo, Nabeel M. Shalabi, Marwan A.
Atallah, Ibrahim Sayed-Ahmed, Anat Galor, Carol L. Karp
Poster Board Number P40:
Topographic analysis of outer retinal atrophy in type 2 idiopathic macular telangiectasia
Ferenc B. Sallo, Irene Leung, Valérie Krivosic, Vincent Rocco, Kiyoko Gocho, Michel Paques, Tunde Peto,
Alan C. Bird, Alain Gaudric
Poster Board Number P41:
Predicting Progression of Geographic Atrophy in Age-Related Macular Degeneration with
Retinal Thickness Measurements using Spectral Domain Optical Coherence Tomography
Praveena Gupta, Kevin Wells, Vincent Nguyen, Bernard F. Godley, Gibran Khurshid
16
Poster Board Number P42:
En-Face Analysis of Spectral Domain Ocular Coherence Tomography (SD-OCT) in Acute
Multifocal Placoid Pigment Epitheliopathy (AMPPE)
Kanchan Bhan, Adam Dubis, Carlos Pavesio
Poster Board Number P43:
Optical Coherence Tomography (OCT) detects epiretinal membrane formation after
intravitreal injection of anti VEGF in cases of Diabetic macular edema
Soheir Mahmoud Ali
Poster Board Number P44:
Enhanced Depth Imaging Optical Coherence Tomography of the Choroid in Chinese Normal
Highly Myopic Eyes
Fenghua Wang, Yanping Zhou, Xiaodong Sun
Poster Board Number P45:
Optical Coherence Tomography (OCT) to Detect Disease Progression in Birdshot
Chorioretinopathy (BCR) – A Novel Multi-View Approach
William R. Tucker, Gregory Short, Robert Nussenblatt, Nida Sen
Poster Board Number P46:
Inferior chiasmal syndrome diagnosed by Optical Coherence Tomography (OCT) before any
visual field defects
Shawkat S. Michel, Monica Michel
Poster Board Number P47:
Assessment of choroidal metastases with the Enhanced Depth Imaging Optical Coherence
Tomography
Efthymia Pavlidou, Amit Arora, Victoria Cohen, Mandeep S. Sagoo
Poster Board Number P48:
Development of Imaging Biomarker Algorithms to Assess Drug Efficacy and Predict
Responders
Kristie Lin, Tom Chang, Allen Ho, Rami Mangoubi, David O'Dowd, Nathan Lowry, Lei Hamilton, John
Irvine, Sicco Popma
17
Paper Presentations
8:00 AM – 5:30 PM
S 310A – D
18
Retinal Imaging
08:00 AM-10:00 AM
Moderators:
James Fujimoto, PhD
Joel Schuman, MD
Wolfgang Drexler, PhD
19
08:00 AM-08:15 AM
Program Number: 1
Improved Visualization of the Vitreous using Swept Source Optical Coherence Tomography with Dynamic
Focus Sweeping
Author(s): Richard Spaide1, Charles Reisman 2, Zhengo Wang2, Kinpui Chan2
1
Vitreous Retina Macula Consultants of NY, 2Topcon Advanced Biological Imaging Laboratory
Purpose: To modify swept source (SS) optical coherence tomography (OCT) to attempt to improve imaging of the
vitreous.
Methods: : The SS-OCT experimental setup is based on Topcon’s DRI OCT-1, which has an A-scan rate of 100
kHz, with a light source centered at 1050 nm and a bandwidth of 100 nm; the scan depth is 2.6mm in tissue.
Although the illuminating beam in conventional OCT has a low numerical aperture, it still converges to and diverges
from the waist of the beam as focused in the eye, and thus yields a significant part of the scan depth out of focus. In
this newly derived imaging method the focus of the beam is dynamically swept through the scan depth during
acquisition of sequential B-scans. A windowed averaging technique synchronized with dynamic focus sweeping is
performed. Local contrast within the resultant image is then accomplished through adaptive equalization methods .
Results: The brightness, contrast, and the intrinsic sharpness of the vitreous was improved as compared with
conventional SS-OCT. The vitreous was found to have the expected bursa premacularis and area of Martegiani
posteriorly, but additional cisternal spaces were routinely imaged anterior to these structures. The appearance of the
retina and choroid were not changed by the methodology employed.
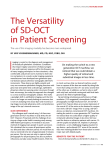
Conclusions: : Improved visualization of the vitreous is possible through modification of scanning technique and
post-processing of the image information. The vitreous is not a mass of gel; it is a complex structure as described in
the past in autopsy eyes by Worst. In vivo evaluation of this architecture may be possible using OCT.
The vitreous appearance using the modified scanning technique employing
swept source optical coherence tomography of a healthy 58 year-old.
A corresponding image from a 28 year-old. Note the presence of a cisternal
space anterior to the premacular bursa.
20
Commercial Relationships Disclosure (Abstract): Richard Spaide: Commercial Relationship(s);Topcon:Code P
(Patent) | Charles Reisman : Commercial Relationship(s);Topcon:Code E (Emplyment) | Zhengo Wang: Commercial
Relationship(s);Topcon:Code E (Emplyment) | Kinpui Chan: Commercial Relationship(s);Topcon:Code E
(Emplyment)
21
08:15 AM-08:30 AM
Program Number: 2
Choroidal, Haller’s and Sattler’s thickness analysis across different age related macular degeneration
phenotypes imaged with 3D-1060nm-OCT
Author(s): Marieh Esmaeelpour1, 2, Siamak Ansari-Shahrezaei1, Behrooz Zabihian2, Martin F Kraus3, Maximilian
Gabriel1, Ilse Krebs1, Joachim Hornegger3, Carl Glittenberg1, Wolfgang Drexler2, Susanne Binder1
1
Ludwig Boltzmann Institute for Retinolgy and Biomicroscopic Laser Surgery , 2Medical University Vienna,
3
Pattern Recognition Lab
Purpose: To examine choroidal thickness (ChT) maps and vascular structure in healthy subjects and in eyes with
age-related-macular degeneration (AMD) using a 3D-1060nm-Widefield-OCT.
Methods: Three-dimensional choroidal tomograms and vascular segmentations 95 subjects with AMD (25 with
reticular pseudodrusen, 25 with stage 2 and 3 non-neovascular and 45 with neovascular AMD), and age and axial
eye length matched healthy subjects (n=35) were recruited. Visual acuity, axial eye length, and fundus photographs
were taken. Images taken with a 3D 1060 nm OCT (512x 512 A scans at ~7 µm axial resolution over 36° angle)
were used to generate total choroidal, Haller’s and Sattler’s maps automatically. 10 healthy and AMD eyes were
imaged for a repeatability analysis of vascular layer thickness mapping.
Results: Choroidal thickness was increased below areas of reticular pseudodrusen (RPD). Between eyes with and
without RPD Sattler’s and Haller’s layer thickness differed significantly. Sattler’s layer thinning in RPD suggests a
choroidopathy of this vascular layer. In the remaining non-RPD cohort, eyes with stage 3 non-neovascular AMD
and neovascular AMD on the fellow eye had the thinnest choroid (P<0.01). Segmentation differences where above
coefficients of repeatability for healthy and AMD eyes.
Conclusions: Enhanced depth penetration of 1060 nm OCT enabled the in vivo investigation of choroidal blood
vessels and choroidal thickness. Choroidal thickness change and structural alterations may illustrate differences in
the pathogenesis of the AMD phenotypes.
Commercial Relationships Disclosure (Abstract): Marieh Esmaeelpour: Commercial Relationship: Code N (No
Commercial Relationship) | Siamak Ansari-Shahrezaei: Commercial Relationship: Code N (No Commercial
Relationship) | Behrooz Zabihian: Commercial Relationship: Code N (No Commercial Relationship) | Martin F
Kraus: Commercial Relationship(s);Optovue:Code P (Patent) | Maximilian Gabriel: Commercial Relationship: Code
N (No Commercial Relationship) | Ilse Krebs: Commercial Relationship: Code N (No Commercial Relationship) |
Joachim Hornegger: Commercial Relationship(s);Optovue:Code P (Patent) | Wolfgang Drexler: Commercial
Relationship(s);Carl Zeiss Meditec:Code C (Consultant);Femtolasers:Code C (Consultant) | Carl Glittenberg:
Commercial Relationship(s);Zeiis Meditec :Code C (Consultant) | Susanne Binder: Commercial
Relationship(s);Alcon:Code C (Consultant)
22
08:30 AM-08:45 AM
Program Number: 3
Effects of optical opacity on retinal cone counts measured by a narrow angle Heidelberg Retina Angiograph
Author(s): Roger Anderson1, 2, Marketa Cilkova1, Padraig Mulholland1, Juliane Matlach1, Nilpa Shah1, Tony
Redmond3, David Garway-Heath1, Steven Dakin1
1
Moorfields Eye Hospital & UCL Institute of Ophthalmology, 2University of Ulster, 3Cardiff University
Purpose: To evaluate the ability of a modified Heidelberg Retina Angiograph (HRA2) to visualize retinal cones in
vivo and to determine the impact of optical opacity induced by cataract-simulating filters on the resultant cone
counts.
Methods: Age-related lens changes were simulated during image acquisition using a series of white opacity filters
(Fog filters 1-5, Lee filters UK). These filters contain opaque particles and simulate wide-angle scatter similar to that
caused by certain cataracts. The induced change in intraocular stray light was determined for each filter using a CQuant Stray Light Meter (Oculus, Wetzlar, Germany). Filters 1, 2, and 3 each add the equivalent of approximately
15 years to the subject’s baseline stray light measurement. Filters 4 and 5 induce optical opacity equivalent to
significant cataract. Cone images of three healthy eyes were acquired using a scan angle of 3 degrees with a HRA2
using filter conditions ranging from “None” to “Fog 5” at a retinal eccentricity of 6 degrees. Cone counts were
generated using customized MatLab image analysis software.
Results: The average cone count within the scan window was 5006 (8,900 cells/mm2) without a filter and was not
substantially affected by Fog filters 1-4. The average cone count declined to 3967 (7,052 cell/mm2) with Fog filter 5
(approx. 20% decline from baseline).
Conclusions: Images of the retinal cones can be obtained in vivo using a modified HRA2 with minimal discomfort
to the subject. Retinal cone images acquired using the modified narrow angle HRA2 are quite robust to the effects of
simulated lens opacity. With current software, automated cone counts remain relatively unchanged until significant
lens opacity develops. This imaging modality has great potential as an aid in diagnosis and monitoring of retinal
pathologies in a clinical setting.
Appearance of raw retinal scan without filter
23
Appearance of a processed image indicating cones included in count.
Commercial Relationships Disclosure (Abstract): Roger Anderson: Commercial Relationship(s);Heidelberg
Engineering:Code F (Financial Support) | Marketa Cilkova: Commercial Relationship: Code N (No Commercial
Relationship) | Padraig Mulholland: Commercial Relationship: Code N (No Commercial Relationship) | Julian
Matlach: Commercial Relationship: Code N (No Commercial Relationship) | Nilpa Shah: Commercial Relationship:
Code N (No Commercial Relationship) | Tony Redmond: Commercial Relationship: Code N (No Commercial
Relationship) | David Garway-Heath: Commercial Relationship(s);Heidelberg Engineering:Code F (Financial
Support) | Steven Dakin: Commercial Relationship: Code N (No Commercial Relationship)
24
08:45 AM-09:00 AM
Program Number: 4
Autofluorescent droplets in the sub-Retinal Pigment Epithelium (RPE)-space of eyes with age-related
macular degeneration (AMD): ex vivo imaging
Author(s): Thomas Ach, Christine A. Curcio
University of Alabama at Birmingham
Purpose: Drusen, the best-studied sub-RPE deposit, are clinically visible only if size exceeds 30 µm in diameter.
Sub-clinical drusen, microdrusen, and entrapment sites are described in electron and light microscopy studies. Little
is known about the autofluorescence (AF) of these sub-RPE deposits. The Purpose of this study is to examine and
classify small (< 30 µm) autofluorescent deposits in flat-mounts of RPE/Bruch membrane.
Methods: Human RPE/Bruch membrane (BrM) flat-mounts were prepared from donor eyes with (n = 4) and
without (n = 4) AMD pathologies (death to preservation time: < 4 hours; previously cryo-preserved). Flat-mounts
were imaged (z-stacks; 0.4 µm intervals) at fovea and perifovea at different excitation wavelengths (390, 488 nm)
using a spinning disc confocal microscope.
Results: Autofluorescent structures were found beneath the RPE on BrM. In en face view, they are circular like a
droplet (Figure). The diameter ranges between a few microns and sub-clinical drusen size. Small droplets (≈ 2 µm
diameter) are also located in deeper layers, probably within BrM. Single droplets may merge to become larger, yet
still sub-clinical deposits, which displace and thin the overlying RPE. Because only few hyperfluorescent drusen >
30 µm were visible in donor eyes > 80 years with normal maculas, these structures may be specific for AMD eyes.
Conclusions: En face imaging of RPE/BrM flat-mounts reveals small AF droplets within AMD eyes, comparable
to the size of entrapment sites, microdrusen, and sub-clinical hard drusen, which all might be precursors of clinically
relevant drusen. The fluorophore(s) remain to be determined. One possibility is retinyl esters within BrM
lipoproteins that contribute cholesterol to drusen. Further analysis of these structures will help elucidate the
relationship of drusen formation and RPE alteration in AMD eyes.
Autofluorescent droplets on Bruch´s membrane, excited with
390 (A) and 488 nm (B). The diameter of autofluorescent droplets
ranges from a few microns (red arrowhead in B) to clinically visible
drusen (yellow arrowhead). 488 nm excitation shows heterogeneous
AF within these droplets. Few autofluorescent RPE lipofuscin
granules are also visible (white arrowhead). The RPE was
unintentionally removed during preparation of this specimen. Donor:
87 year old female, Caucasian, early AMD.
Commercial Relationships Disclosure (Abstract): Thomas Ach:
Commercial Relationship: Code N (No Commercial Relationship) |
Christine Curcio: Commercial Relationship: Code N (No Commercial
Relationship)
25
09:00 AM-09:15 AM
Program Number: 5
High resolution imaging of Gunn’s dots
Author(s): Michel Paques, Edouard Koch, Celine Chaumette, Alexandre Leseigneur
Quinze-Vingts Hospital
Purpose: In healthy fundi, glistening whitish dots (so-called Gunn’s dots) can often be seen, especially in young
subjects. They are commonly attributed to the reflectance of Müller cell’s footplates. However, despite their
potential interest as biomarkers of retinal diseases, Gunn’s dots have received little attention. Here, we analyzed the
imaging characteristics of Gunn's dots.
Methods: Scanning laser ophthalmoscope reflectance imaging and adaptive optics infrared flood imaging were
performed in 18 healthy subjects (age range, 18-58 years). The localization, density and shape of Gunn’s dots were
analyzed.
Results: Both modalities ensured accurate detection of Gunn’s dots. They were more frequently observed in the
midperiphery, although some were detected in the macula. The reflectance of Gunn’s dots showed a strong
directional variability, which paralleled that of the inner limiting membrane. The mean (±SD) diameter of Gunn’s
dots was 13.3µm (±3.5). Their density peaked at ~120/mm², and linearly decreased with age.
Conclusions: Gunn’s dots are highly anisotropic structures close to the inner limiting membrane. Their density,
size and age-related disappearance suggests that they are hyalocytes rather than Müller cells. Further studies are
necessary to progress in the determination of their origin and disease-related changes.
Adaptive optics imaging of
Gunn’s dots (arrowheads). On
the left are magnification of four
Gunn’s dots showing the
variability of their shape.
Commercial Relationships Disclosure (Abstract): Michel Paques: Commercial
Relationship(s);ImagineEye:Code C (Consultant) | Edouard Koch: Commercial Relationship: Code N (No
Commercial Relationship) | Celine Chaumette: Commercial Relationship: Code N (No Commercial Relationship)
| Alexandre Leseigneur: Commercial Relationship: Code N (No Commercial Relationship)
26
09:15 AM-09:30 AM
Program Number: 6
Detection of Retinal Blood Flow Turbulence at Arteriovenous Crossings using Spectral Domain Optical
Coherence Tomography
Author(s): Michael Larsen
University of Copenhagen
Purpose: To determine if spectral domain optical coherence tomography (SD-OCT) can distinguish turbulent from
laminar blood flow in retinal blood vessels.
Methods: Retrospective observational study of 7 arteriovenous crossings in 6 eyes from 6 patients who underwent
SD-OCT and fluorescein angiography based on suspicion of manifest or imminent branch retinal vein occlusion.
Results: Angiographic evidence of turbulence was seen at x crossings in 3 eyes whereas laminar angiographic flow
was intact at y crossings in 3 eyes . All crossings involved veins of diameter 100 µm or larger. On SD-OCT complex
or chaotic reflectivity patterns were seen at the point of crossing and downstream of it at all 3 sites with
angiographic turbulence whereas OCT reflectivity patterns consistent with laminar flow were seen behind and
downstream of the crossing site in the eyes without angiographic turbulence.
Conclusions: Patterns of abnormal intravascular reflectivity were detected by SD-OCT at arteriovenous crossings
where turbulent blood had been documented by fluorescein angiography. These proof-of-principle observations
confirm that SD-OCT enables qualitative study of retinal blood flow that may be useful for distinguishing between
branch retinal vein congestion and imminent branch retinal vein occlusion.
Above: Longitudinal SD-OCT scan along the axis of a retinal vein showing vessel wall reflexes and an intraluminal
five-layer pattern of reflectivity that presumably represents plasma-rich fluid near the endothelium, laminar shearpattern flow in the intermediate layers with the highest velocity gradients (high reflectivity), and absence of velocity
gradients centrally in the vessel with randomly oriented blood cells (low reflectivity). The scan transects a retinal
artery crosssing anterior of the vein. The flow pattern in the vein is laminar on both sides of the crossing, relative
hypoflectivity being visible where the direction of flow is not perpendicular to the instrument’s line of sight. Below:
A retinal vein and artery scanned in a manner comparable to the upper image, but differing from the former in that
the vein is anterior to the artery and in that a disrupted reflectivity pattern presents evidence of turbulent flow at and
downstream of the arteriovenous crossing.
Commercial Relationships Disclosure (Abstract): Michael Larsen: Commercial Relationship: Code N (No
Commercial Relationship)
27
09:30 AM-09:45 AM
Program Number: 7
Ganglion Cell Analysis using High-Definition Optical Coherence Tomography in Patients with mild cognitive
impairment and Alzheimer’s Disease
Author(s): Carol Y. Cheung1, 2, Yiting Ong1, M. Kamran Ikram1, Christopher Chan3, Tien Yin Wong1, 2
1
Singapore Eye Research Institute, 2Duke-NUS Graduate Medical School, 3 National University Health System
Purpose: Alzheimer disease (AD) is a neurodegenerative disorder with emerging evidence that it is associated with
retinal ganglion cell loss; however, few data exist to establish this association. We determine whether the ganglion
cell-inner plexiform layer (GC-IPL) and retinal nerve fiber layer (RNFL), as measured by non-invasive in vivo
spectral-domain optical coherence tomography (SD-OCT), are altered in patients with AD and mild cognitive
impairment (MCI).
Methods: Patients with AD and MCI were recruited from dementia/memory clinics, and cognitively normal
controls were selected from the Singapore Epidemiology of Eye Disease program. SD-OCT ( Cirrus HD-OCT,
software version 6.0.2, Carl Zeiss Meditec Inc, Dublin, CA) was used to measure the GC-IPL and RNFL
thicknesses. Analyses of covariance was performed to estimate mean GC-IPL and RNFL thicknesses in the groups
adjusted for age, gender, ethnicity, SD-OCT signal strength and additionally for hypertension, diabetes and histroy
of myocardial infarction. AUC was used to assess the ability of GC-IPL and RNFL thicknesses to discriminate AD
and MCI from cognitively normal controls.
Results: We included 100 patients with AD, 40 patients with MCI and 123 cognitively normal elderly. Compared
with the cognitively normal controls, patients with AD had significantly thinner GC-IPL thicknesses in all six
(superior, superonasal, inferonasal, inferior, inferotemporal and superotemporal) sectors (mean differences from 3.42 to -4.99µm, all p<0.05) and thinner RNFL thickness in the superior quadrant (111.1 vs. 105.1µm,
p=0.039). Patients with MCI also had significant thinner average GC-IPL thicknesses and in half of the six sectors
(superonasal, inferior and inferotemporal) compared with cognitively normal controls (mean differences from -3.62
to -5.83µm, all p<0.05). The AUC of GC-IPL were generally higher than that of RNFL to discriminate AD and MCI
from cognitively normal controls.
Conclusions: Our data strengthens the link between retinal ganglion cell neuronal and optic nerve axonal loss with
AD, and suggest that assessment of macular GC-IPL can be a test to detect neuronal injury in early AD and MCI.
Commercial Relationships Disclosure (Abstract): Carol Cheung: Commercial Relationship: Code N (No
Commercial Relationship) | Yiting Ong: Commercial Relationship: Code N (No Commercial Relationship) | M.
Kamran Ikram: Commercial Relationship: Code N (No Commercial Relationship) | Christopher Chan: Commercial
Relationship: Code N (No Commercial Relationship) | Tien Yin Wong: Commercial Relationship: Code N (No
Commercial Relationship)
28
09:45 AM-10:00 AM
Program Number: 8
Automatic Analysis of Color Retinal Images for CMV Retinitis Screening
Author(s): Sandeep Bhat1, Chaithanya Ramachandra1, Todd P. Margolis2, Jeremy Keenan3, Kaushal Solanki1
1
Eyenuk, Inc, 2 Washington University School of Medicine, 3University of California, San Francisco Medical Center
Purpose: Cytomegalovirus retinitis (CMVR), a treatable retinal infection affecting HIV/AIDS patients, is a leading
cause of blindness in many developing countries. For example, in Thailand there are less than 700 ophthalmologists
to care for over 300,000 patients at risk for vision loss from the disease. The telemedicine framework setup by the
Chiang Mai University Medical Centre, Thailand and UCSF is aiding the growing need for CMVR screening. To
further scale this telemedicine solution, we have developed novel screening tools that use advanced image analysis
techniques to automatically screen images and aid efficient triage of retinitis patients.
Methods: 7-field color retinal fundus mosaics are first denoised using edge-preserving bilateral filter. Variations in
the images, due to different lighting conditions, equipment used, technicians, and patient anatomy are “neutralized”
using a novel median filter based normalization technique that uses local background estimation to enhance the
image at every pixel. A Hessian-based interest region and “vesselness” map detection is then applied, and the
following image descriptors are computed: sum-modified Laplacian (for focus/blur), saturation measure, Michelson
contrast, color measure, local noise metric, image entropy, and local binary patterns (for texture). The descriptors are
concatenated, subjected to dimensionality reduction using PCA, and used to train a support vector classifier in a 5fold cross-validation framework.
Results: The tools were tested using 211 images, graded for CMVR, by randomly splitting them into 40 different
training-testing datasets. In each split, 75% of the images were used for training and 25% were reserved for testing.
The lesion-degraded retinitis images were flagged to be positive for CMVR by our system with an average accuracy
of 85% (average area under ROC curve = 0.93).
Conclusions: Proposed screening tool does a good job of automatically screening retinal images for signs of
CMVR. In conjunction with telemedicine frameworks, it is expected to greatly reduce the risk of blindness in
HIV/AIDS patients in developing countries.
Fig 1: CMVR screening results for 7-field retinal mosaics from a Topcon TRC-NW 6S camera. (a,b) “Normal
retina” screened as “No refer”. (c,d) “Retina with CMVR” screened as “refer”. (e,f) Images from “cannot
determine” category screened as “refer”.
29
Commercial Relationships Disclosure (Abstract): Sandeep Bhat: Commercial Relationship(s);Eyenuk Inc:Code E
(Emplyment) | Chaithanya Ramachandra: Commercial Relationship(s);Eyenuk Inc:Code E (Emplyment) | Todd
Margolis: Commercial Relationship(s);Washington University School of Medicine in St. Louis:Code E
(Emplyment) | Jeremy Keenan: Commercial Relationship(s);University of California, San Francisco:Code E
(Emplyment) | Kaushal Solanki: Commercial Relationship(s);Eyenuk Inc:Code E (Emplyment)
30
Functional Retinal Imaging
10:30 AM-12:30 PM
Moderators:
Richard Spaide, MD
Giovanni Gregori, PhD
31
10:30 AM-10:45 AM
Program Number: 9
Optical Coherence Tomography Angiography of Macular Disease
Author(s): David Huang1, Yali Jia1, Steven T. Bailey1, Thomas Hwang1, Andreas K. Lauer1, Christina J. Flaxel1,
Mark E. Pennesi1, David J. Wilson1, Joachim Hornegger2, James G. Fujimoto3
1
Oregon Health & Science University, 2University of Erlangen-Nuremberg, 3MIT
Purpose: To determine the characteristic features of common macular diseases using the novel imaging modality of
optical coherence tomography (OCT) angiography.
Methods: Healthy control subjects and subjects with a variety of macular pathologies underwent OCT angiography
in prospective observational studies. Fluorescein angiography (FA) was obtained when clinically indicated. OCT
angiography scans were obtained with a high-speed (100,000 A-scans/sec) 1050 nm wavelength swept-source OCT.
The scans spanned 3.5×3.5 mm and was acquired in 4.0 sec. Flow was detected using the split-spectrum amplitudedecorrelation angiography algorithm. The volumetric angiography was segmented into four layers: inner retina,
outer retina, inner choroid and outer choroid. En face maximum flow projection was used to obtain 2D angiograms
of the 4 layers.
Results: In all 5 healthy subjects, retinal capillary networks were visualized in the inner retinal layer, confluent
choriocapillaris could be visualized in the inner choroid, and no flow was detected in the outer retina. In all 8 cases
of neovascular age-related macular degeneration (AMD), OCT angiography demonstrated choroidal
neovascularization (CNV) in the outer retinal layer. The depth of CNV relative to the retinal pigment epithelium
(RPE) could be determined and the area and flow index could be quantified. The CNV area corresponded well to
FA except in 3 cases where fluorescence was blockage by hemorrhage or RPE. In 2 cases of dry AMD, OCT
angiography showed loss of choriocapillaris from the inner choroid in areas of geographic atrophy and some areas of
large drusen. In 2 cases of nonproliferative diabetic retinopathy (DR), regions of retinal capillary dropout shown by
OCT angiography agreed with FA. In 1 case of proliferative DR, OCT angiography showed retinal
neovascularization (RNV) above inner limiting membrane (Figure 1). In 2 cases of retinal dystrophy,
choriocapillaris dropout was shown on choroidal OCT angiogram.
Conclusions: OCT angiography was able to detect the presence of abnormal vessels (CNV & RNV) by their
location in the normally avascular outer retina and vitreous medium. Capillary dropout could be mapped in DR and
choriocapillaris loss could be detected in AMD and retinal dystrophy.
32
Commercial Relationships Disclosure (Abstract): David Huang: Commercial Relationship(s);Optovue:Code F
(Financial Support);Optovue:Code I (Personal Financial Interest);Optovue:Code P (Patent);Carl Zeiss Meditec:Code
P (Patent) | Yali Jia: Commercial Relationship(s);Optovue:Code P (Patent) | Steven Bailey: Commercial
Relationship: Code N (No Commercial Relationship) | Thomas Hwang: Commercial Relationship: Code N (No
Commercial Relationship) | Andreas Lauer: Commercial Relationship: Code N (No Commercial Relationship) |
Christina Flaxel: Commercial Relationship: Code N (No Commercial Relationship) | Mark Pennesi: Commercial
Relationship: Code N (No Commercial Relationship) | David Wilson: Commercial Relationship: Code N (No
Commercial Relationship) | Joachim Hornegger: Commercial Relationship(s);Optovue:Code P (Patent) | James
Fujimoto: Commercial Relationship(s);Optovue:Code P (Patent);Carl Zeiss Meditec:Code P (Patent)
33
10:45 AM-11:00 AM
Program Number: 10
En Face Visualization of Retinal Pathologies Using Ultrahigh Speed Swept Source Optical Coherence
Tomography
Author(s): Woo Jhon Choi1, Mehreen Adhi2, Eric Moult1, ByungKun Lee1, Zhao Wang1, Martin F. Kraus3, 1, Jay S.
Duker2, Joachim Hornegger3, James G. Fujimoto1, Nadia K. Waheed2
1
Massachusetts Institute of Technology, 2New England Eye Center and Tufts University, 3University of ErlangenNuremberg
Purpose: We investigate en face visualization of retinal pathologies using ultrahigh speed 400kHz swept source
optical coherence tomography (SSOCT) and OCT angiography.
Methods: Imaging was performed with an ultrahigh speed SSOCT prototype at 1um wavelengths using a vertical
cavity surface emitting laser (VCSEL) swept light source at 400kHz A-scan rate. When necessary, a 3D motioncorrection / registration algorithm was used to suppress motion artifacts and increase signal-to-noise. Volumetric
3mm×3mm and 6mm×6mm scans were acquired from patients with age related macular degeneration, diabetic
retinopathy and age matched normals. OCT angiography was performed using multiple B-scans from the same
location to generate motion contrast 3D images of retinal, choriocapillaris and choroidal vasculature. Bruch’s
membrane was segmented and en face OCT images were generated at different depths.
Results: Patients with non-exudative age-related macular degeneration (dry AMD) with and without geographic
atrophy (GA) and diabetics with and without retinopathy were imaged with ultrahigh speed SSOCT. Figure 1 shows
an example of dry AMD patient with GA. Four orthogonally-scanned volumetric data sets over a 6mm×6mm area
(shown in yellow on the fundus image) were acquired and motion-corrected. En face OCT at the RPE level shows
the locations of drusen (Figure 1C). The area of RPE atrophy can be visualized by projecting all depths below the
RPE, into the sclera (Figure 1D). The OCT angiogram of the choriocapillaris shows choriocapillaris atrophy in the
region of GA (Figure 1E).
Conclusions: Ultrahigh speed SSOCT and OCT angiography enables en face visualization of retinal / choroidal
structure and vasculature. The ability to comprehensively image structure and vasculature features, especially the
choriocapillaris, promises to be an important tool for assessing pathogenesis, early disease and disease progression.
34
Figure 1. 77 year old dry AMD patient with GA (A) Fundus photograph. (B-E) OCT fundus projection, en face OCT
at the RPE level, sub RPE intensity projection showing GA, and OCT angiogram of choriocapillaris. OCT area
marked by the yellow square in (A). 6mm×6mm field of view.
Commercial Relationships Disclosure (Abstract): Woo Jhon Choi: Commercial Relationship: Code N (No
Commercial Relationship) | Mehreen Adhi: Commercial Relationship: Code N (No Commercial Relationship) | Eric
Moult: Commercial Relationship: Code N (No Commercial Relationship) | ByungKun Lee: Commercial
Relationship: Code N (No Commercial Relationship) | Zhao Wang: Commercial Relationship: Code N (No
Commercial Relationship) | Martin Kraus: Commercial Relationship(s);Optovue, Inc. :Code P (Patent) | Jay Duker:
Commercial Relationship(s);Carl Zeiss Meditec Inc.:Code F (Financial Support);Optovue Inc.:Code F (Financial
Support);Hemera Biosciences:Code I (Personal Financial Interest) | Joachim Hornegger: Commercial Relationship:
Code N (No Commercial Relationship) | James Fujimoto: Commercial Relationship(s);Carl Zeiss Meditec Inc:Code
P (Patent);Optovue Inc:Code P (Patent);Optovue Inc:Code I (Personal Financial Interest) | Nadia Waheed:
Commercial Relationship: Code N (N Commercial Relationship)
35
11:00 AM-11:15 AM
Program Number: 11
Quantitative Insights into Macular Microvascularity using Adaptive Optics Scanning Light Ophthalmoscopy
Fluorescein Angiography
Author(s): Richard Rosen1, 3, Alexander Pinhas1, Moataz Razeen1, Nishit Shah1, Alexander Gan1, Richard Bavier1,
Rishard Weitz1, Joseph Carroll2, Alfredo Dubra2, Yuen Ping T. Chui1, 3
1
New York Eye & Ear Infirmary, Mount Sinai Health System, 2Medical College of Wisconsin, 3New York Medical
College
Purpose: Adaptive Optics Scanning Light Ophthalmoscopy (AOSLO), coupled with fluorescein angiography (FA)
, is able to resolve dynamic cellular details of human retinal microvasculature in healthy and diseased eyes. Using
quantitative image analysis, AOSLO provides a platform for characterizing retinal microvascular changes due to
age, onset of disease or response to treatment. Here, we show how foveal avascular zone (FAZ), capillary density
and lumen in diabetes (DR), central retinal vein occlusion (CRVO), and sickle cell retinopathy (SCR) are different
from those in fellow eyes and/or normal eyes.
Methods: During AOSLO FA imaging, simultaneous reflectance (790 nm) and fluorescence (488 nm) image
sequences with 1.75° field of view were stitched together to create microvascular maps of a 6° square region
centered on the fovea. AOSLO FA maps were skeletonized and divided into regions of interest (ROIs). Vessel
length (mm) and density (mm-1) were then calculated per ROI. For FAZ attribute quantification, the FAZ was
delineated manually creating an FAZ layer mask. Based on the masks, FAZ area (mm 2), effective diameter (µm,
diameter of a uniform circle derived from FAZ area), perimeter (µm) and tortuosity index (TI) were computed.
Results: Comparison of FAZ parameters of area, diameter, and perimeter in normal and vasculopathic eyes showed
large variations, with CRVO eyes having highest values followed by SCR, DR, and controls . Tortuosity Index (TI),
however, was highest in DR eyes followed by SCR, CRVO and controls . CRVO fellow eyes all showed some
capillary dropout near the FAZ with significant decrease in vessel length and density compared to control eyes.
FAZ mean capillary lumen diameter for early diabetic subjects was found to be 35% larger than that of the control
subjects.
Conclusions: Quantification of the microvascular geometry utilizing AOSLO in vivo microscopy shows significant
potential for studying complex clinical questions involving retinal vascular diseases. This approach may help direct
therapeutic interventions based upon fine numerical distinctions as opposed to clinical impressions derived from
conventional clinical imaging modalities.
AO SLO FA is assembled, skeletonized, and vascular density is measured.The FAZ is outlined to analyze tortuosity
and perifoveal intercapillary area.
36
Ischemic Diabetic FAZ capillary remodelling
Commercial Relationships Disclosure (Abstract): Richard Rosen: Commercial Relationship(s);Clarity:Code C
(Consultant);Optovue:Code C (Consultant);OD-OS:Code C (Consultant);Opticology:Code P (Patent) | Alexander
Pinhas: Commercial Relationship: Code N (No Commercial Relationship) | Moataz Razeen: Commercial
Relationship: Code N (No Commercial Relationship) | Nishit Shah: Commercial Relationship: Code N (No
Commercial Relationship)| Alexander Gan: Commercial Relationship: Code N (No Commercial Relationship) |
Richard Bavier: Commercial Relationship: Code N (No Commercial Relationship) | Rishard Weitz: Commercial
Relationship: Code N (No Commercial Relationship) | Joseph Carroll: Commercial
Relationship(s);ImagineEyes:Code C (Consultant) | Alfredo Dubra: Commercial Relationship(s);University of
Rochester:Code P (Patent) | Yuen Ping Chui: Commercial Relationship: Code N (No Commercial Relationship)
37
11:15 AM-11:30 AM
Program Number: 12
Quantification of Absolute Number of Photoreceptors from Ultra-Widefield Imaging
Author(s): Daniel E. Croft1, Charles C. Wykoff1, David M. Brown1, Jano VanHemert2
1
Retina Consultants of Houston, 2Optos plc
Purpose: To develop a methodology which facilitates estimation of the absolute number of cones and rods in
regions selected from ultra-widefield (UWF) fundus images and fluorescein angiograms, utilizing the Optos 200Tx
scanning laser ophthalmoscope (SLO) (Optos, UK).
Methods: Previously published retinal histology data sampled cone and rod density radially from the fovea at 1mm
intervals in the superior, inferior, nasal and temporal directions (Curcio C.A., Sloan K.R, Kalina R.E. The Journal of
Comparative Neurology. 1990). This data was mapped onto a 3-dimensional (3D) model eye with a 24mm diameter
and interpolated across the entire retinal surface to create a map of approximate photoreceptor densities, including
independent rod and cone density maps. To calculate retinal surface area, the location of the fovea was used to
identify the gaze angle of the UWF image and a transformation was applied to project the image to its anatomically
correct location on the 3D model eye. This was performed by ray tracing every pixel through a combined optical
model of the Optos 200Tx SLO and the Navarro UWF model eye. This completed 3D model was then mapped to a
2D stereographic projection and regions of interest were selected for quantification. Area was metrically quantified
with spherical trigonometry by projecting the selection back onto the 3D model eye. Quantification of
photoreceptors was achieved by multiplying the surface area of selected regions by the density of photoreceptors in
the selected regions. This methodology was applied to clinical examples.
Results: Two clinical examples were analyzed - one eye with diabetic retinopathy and one eye with retinal vein
occlusion. Both of these eyes demonstrated substantial areas of central and peripheral non-perfusion on UWF
fluorescein angiography. These areas of non-perfusion were selected manually. In the eye with diabetic retinopathy
194.7 mm2 of non-perfusion were selected representing 19,241,461 rods and 863,807 cones. In the case of RVO 326
mm2 of non-perfusion were selected representing 31,657,976 rods and 1,248,816 cones.
Conclusions: A method to estimate the absolute number of photoreceptors from ultra-widefield imaging was
developed by combining previously published retinal histological data with metric quantification. This methodology
was applied to clinical examples of retinal non-perfusion in diabetic retinopathy and retinal vein occlusion.
Commercial Relationships Disclosure (Abstract): Daniel Croft: Commercial Relationship: Code N (No
Commercial Relationship) | Charles Wykoff: Commercial Relationship: Code N (No Commercial Relationship) |
David Brown: Commercial Relationship: Code N (No Commercial Relationship) | Jano VanHemert: Commercial
Relationship(s);Optos plc:Code E (Emplyment)
38
11:30 AM-11:45 AM
Program Number: 13
Parafoveal cone hyporeflectivity and recovery seen by adaptive optics in posterior uveitis
Author(s): Phoebe Lin1, Kristin Biggee1, Michael Gale1, Eric Suhler1, 2, Mark Pennesi1
1
Oregon Health and Science University, 2VA hospital Portland
Purpose: The Purpose of this study was to determine if the use of adaptive optics (AO) can detect subclinical
changes in posterior uveitis affecting the outer retina.
Methods: Sequential patients who had posterior uveitis affecting the outer retina were imaged with the Rtx1 Optics
flood illumination AO camera using a field of view of 4° by 4°, and a resolution of 1 µm. These images were
compiled into a montage and macular cone densities calculated using Matlab software. AO images were compared
to SD-OCT, fluorescein angiography (FA), and fundus autofluorescence (FAF) images.
Results: Four patients with posterior uveitis affecting the outer retina were imaged with the AO camera: one with
serpiginous chorioretinitis, one with multiple evanescent white dot syndrome (MEWDS), and two patients with
multifocal choroiditis (MFC) with acute outer retinal atrophy (AORA). In all 4 cases, the affected eye showed areas
of altered photoreceptor reflectivity on AO images that corresponded to changes seen on FAF, SD-OCT, or FA. In
some cases, abnormalities that were not seen on other imaging techniques were noted on AO. In one patient with
MFC with AORA, AO images revealed abnormal parafoveal cone reflectivity in the unaffected eye that was not
noted on examination or other images. In the patient with MEWDs, multifocal areas of altered cone reflectivity
were more apparent than that expected by SD-OCT, FAF, or FA (Figure 1). In the case of serpiginous
chorioretinitis, AO images obtained five weeks after initiating treatment with high dose prednisone and azathioprine
demonstrated a reversal in the abnormal reflectivity of parafoveal cones (Figure 2).
Conclusions: AO delineates areas of altered photoreceptor reflectivity not seen on other imaging techniques and
may prove to be a useful imaging modality to gauge treatment efficacy and to monitor disease course in posterior
uveitis.
39
A 17 year-old woman with MEWDS presented with multifocal parafoveal cone hyporeflectivity on AO that recovers
upon follow up. Top panels: FAF; Middle panels, AO with cone density plot; Bottom panels, SD-OCT
A 60 year-old woman with serpiginous chorioretinitis presenting with 20/20 vision OS has cone hyporeflectivity on
AO outside the areas of involvement seen on other imaging modalities that reverses after treatment. Top panels:
FAF; Middle panels, AO with cone density plot; Bottom panels, SD-OCT
Commercial Relationships Disclosure (Abstract): Phoebe Lin: Commercial Relationship: Code N (No
Commercial Relationship) | Kristin Biggee: Commercial Relationship: Code N (No Commercial Relationship) |
Michael Gale: Commercial Relationship: Code N (No Commercial Relationship) | Eric Suhler: Commercial
Relationship: Code N (No Commercial Relationship) | Mark Pennesi: Commercial Relationship: Code N (No
Commercial Relationship)
40
11:45 AM-12:00 PM
Program Number: 14
Total Retinal Blood Flow Measurement with 70k Hz Spectral Domain OCT
Author(s): Ou Tan, Gangjun Liu, Yali Jia, David Huang
Casey Eye Institute
Purpose: To develop an automated algorithm to measure total retinal blood flow (TRBF) using 70k Hz Doppler
spectral domain OCT
Methods: One eye of each participant was scanned with a 70k Hz spectral domain OCT (RTVue-XR, Optovue,
CA). The OCT is calibrated for the transformation from Doppler shift to speed based on a flow phantom. The TRBF
scan pattern contains 5 repeated volume scans (depth=2.3mm, horizontal=1.6 mm, and vertical=2mm) obtained in 3
seconds, and centered on central retinal vessels. Each eye was scanned 3 times. Complex OCT signal was save and
both reflectance and Doppler shift computed in postprocessing using a split-spectrum algorithm. An automated
algorithm was developed for TRBF measurement using multiple plane en face Doppler summation. First, veins and
arteries were segmented and classified based on both Doppler shift and reflectance. Second, phase unwrapping was
applied to correct the Doppler shift in vessels (Figure 1). Then, for each retinal vein, blood flow was measured at an
optimal plane where the calculated flow is maximized. The TRBF was calculated by summing flow in all veins. The
algorithm tracks vascular branching so that either root or branch veins are summed, but never both. Finally, the
TRBF in 5 repeated volumes were average to reduce variation due to pulsation during the cardiac cycle. Arterial
flow was not summed because of greater noise due to pulsation and phase wrapping.
Results: A total of 14 eyes of 14 participants (9 healthy controls, 5 glaucoma participants) were enrolled. The
TRBF of healthy controls is 42.0±5.0 µl/min. The TRBF of glaucoma controls is 38.1±9.2 µl/min. The intra-visit
repeatability was 11.1% (coefficient of variation) for healthy participants and 9.2% for glaucoma participants. Four
out of 5 glaucoma participants had TRBF at least 1 standard deviation below health control group mean.
Conclusions: An automated algorithm was developed for TRBF measurement using 70KHz spectral-domain OCT.
The TRBF measured in healthy and glaucoma subjects are within the range described in literatures. The
repeatability of a single scan is acceptable.
Figure 1 (A) Color disc photograph showing volumetric Doppler scan area (green rectangular outline).
41
Figure 1 (B) En face color Doppler showing the veins (blue representing flow out of eye) and the measurement
positions for each vein (circular outlines).
Commercial Relationships Disclosure (Abstract): Ou Tan: Commercial Relationship(s);Zeiss Medtech:Code P
(Patent);Optovue:Code P (Patent);Optovue:Code F (Financial Support) | Gangjun Liu: Commercial Relationship:
Code N (No Commercial Relationship) | Yali Jia: Commercial Relationship(s);Optovue:Code P (Patent) | David
Huang: Commercial Relationship(s);Zeiss Medtech:Code P (Patent);Optovue:Code F (Financial
Support);Optovue:Code I (Personal Financial Interest);Optovue:Code P (Patent)
42
Glaucoma / Anterior Eye
01:30 PM-03:30 PM
Moderators:
Brand Fortune, PhD
Susan Vitale, PhD
43
01:30 PM-01:45 PM
Program Number: 15
Evaluation of the Spatial Relationship Between Glaucoma Progression using Confocal Scanning Laser
Ophthalmoscopy (CSLO), Optical Coherence Tomography (OCT), and Visual Field (VF).
Author(s): Dingle Foote1, Gadi Wollstein1, Divya Narendra1, Yun Ling1, 2, Richard A. Bilonick1, 2, Hiroshi
Ishikawa1, 3, Larry Kagemann1, 3, Cynthia Mattox5, James G. Fujimoto4, Joel S. Schuman1, 3
1
University of Pittsburgh Medical Center, 2Graduate School of Public Health, University of Pittsburgh,, 3Swanson
School of Engineering, University of Pittsburgh, 4Massachusetts Institute of Technology, 5Tufts Medical Center
Purpose: To evaluate the spatial relationship between structural and functional progression as measured by CSLO,
OCT, and VF.
Methods: 107 eyes of 64 glaucoma, glaucoma suspect and healthy subjects were followed for a mean of 5.5 years
(range: 1.6-8.1). Each subject had baseline and final visits within 6 months from one device to the other. Four
generations of OCT were used to perform retinal nerve fiber layer (RNFL) thickness measurements over this time
period and then standardized by applying calibration equations. Superior and inferior quadrant RNFL thicknesses,
rim areas, and VF mean sensitivities in the corresponding locations were used for analysis. Progression with each
parameter was defined as a significantly negative linear regression slope on at least two consecutive visits.
Results: Of the 107 eyes studied, 5 eyes showed global RNFL progression by OCT with 4 eyes (3 superior, 1
inferior) showing progression by quadrants. 6 eyes progressed globally by CSLO measured rim area with 10 eyes (5
superior, 5 inferior) showing regional progression. Six eyes showed global progression by VF with 5 eyes (5
superior, 0 inferior) showing regional progression. There was no agreement of global progression between CSLO
and OCT while 2 eyes (1 superior, 1 inferior) showed spatial agreement. Only 2 eyes agreed in global progression
with VF and OCT but there was no agreement between VF and CSLO and no spatial agreement between VF and
OCT or CSLO.
Conclusions: Despite a lengthy follow-up period, and large cohort there was very poor global or spatial agreement
between OCT, CSLO, and VF. No device has proven to be a superior tool and therefore no individual device can be
recommended for detection of glaucoma progression.
Commercial Relationships Disclosure (Abstract): Dingle Foote: Commercial Relationship: Code N (No
Commercial Relationship) | Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) |
Divya Narendra: Commercial Relationship: Code N (No Commercial Relationship) | Yun Ling: Commercial
Relationship: Code N (No Commercial Relationship) | Richard Bilonick: Commercial Relationship: Code N (No
Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial Relationship) |
Larry Kagemann: Commercial Relationship: Code N (No Commercial Relationship) | Cynthia Mattox: Commercial
Relationship: Code N (No Commercial Relationship) | James Fujimoto: Commercial Relationship(s);Zeiss:Code P
(Patent);Optovue:Code P (Patent);Optovue:Code I (Personal Financial Interest) | Joel Schuman: Commercial
Relationship(s);Zeiss:Code P (Patent)
44
01:45 PM-02:00 PM
Program Number: 16
Identification of Glaucoma using Biomarkers of Retinal Vascular Morphology and Blood Flow Computed
from Retinal Fundus Images
Author(s): David Meadows, Rick Clark, Daniel Dickrell
University of Florida
Purpose: To determine if morphological and blood flow characteristics based on Constructal Analysis of the retinal
vasculature provide robust biomarkers for screening glaucomatous patients.
Methods: Studies have recently reported retinal blood flow is compromised in a large percentage of glaucoma
patients. Two suggested mechanisms for vascular dysfunction are increased resistance to flow and/or reduced
perfusion pressure. A new method of automatically classifying the blood flow capacity of retinal vascular networks
into healthy or glaucoma categories has been developed (OQULUS™). Color fundus photographs are used to
characterize the morphology and geometry of arterial and venous networks followed by Constructal Analysis. Based
on connectivity and flow capacitance of individual vessel segments, the overall network flow capacities were
calculated. Arterial bifurcations were carefully characterized using metrics such as junction exponents, diameter
ratios, area ratios and branching angles. These vascular metrics define the ability for blood to pass efficiently
through the interconnected series of retinal vessels. 23 high-resolution color fundus images from 13 healthy and 10
glaucomatous patients were analysed. (http://www5.cs.fau.de/research/data/fundus-images/). Biomarkers were
identified for the arterial and venous networks from each image
Results: Results identified large differences between healthy and glaucomatous eyes for overall network flow rates.
Healthy arterial networks had average flow capacity of 1.50 ± 0.74 µL/kPa-s while the glaucomatous arterial
networks had average flow that was reduced by 70% to 0.43 ± 0.16 µL/kPa-s (ROC analysis: Area = 0.85,
Sensitivity = 0.82, Specificity = 0.85). The diminished flow capacity of retina vasculature clearly showed
glaucomatous patients had global narrowing of vessel networks. Ocular blood flow deficiency has been suggested as
a cause of optic nerve damage, either directly or indirectly through raised intraocular pressure, supporting the utility
of OQULUS™ algorithms. Other strong biomarker signals include: artery and vein diameter, artery tortuosity,
artery and vein asymmetry index, artery bifurcation angle.
Conclusions: Results for the OQULUS™ software based on Constructal Analysis algorithms clearly identified
biomarkers that enable the automated screening of glaucoma patients from color fundus imagery.
Commercial Relationships Disclosure (Abstract): David Meadows: Commercial Relationship(s);Sentinel
Diagnostic Imaging:Code I (Personal Financial Interest) | Rick Clark: Commercial Relationship(s);Sentinel
Diagnostic Imaging:Code I (Personal Financial Interest) | Daniel Dickrell: Commercial Relationship(s);sentinel
Diagnostic Imaging:Code I (Personal Financial Interest)
45
02:00 PM-02:15 PM
Program Number: 17
Measurement of BMO plan-based anterior lamina cribrosa surface depth (ALCSD) parameter using a
deconvolution approach applied to 3D spectral domain optical coherence tomography optic nerve head
images
Author(s): Akram Belghith, Christopher Bowd, Zhiyong Yang, Felipe Medeiros, Robert N. Weinreb, Linda M.
Zangwill
Hamilton Glaucoma Center
Purpose: To propose a new approach for locating the Bruch's membrane opening (BMO) and the anterior lamina
cribrosa surface (ALCS) of 3D Spectralis SD-OCT images (Heidelberg Engineering, 48 enhanced depth imaging
EDI radial B-scans centered on the optic nerve head).
Methods: We formulated the detection of the BMO and the ALCS as a missing data problem where we jointly
estimated the noise hyper-parameters and the segmented image. To deal with the overlapping of the Bruch's
membrane and the retinal pigment epithelium layers and the poor image resolution around the lamina cribrosa area,
we proposed the use of an image deconvolution approach that consists of assigning to each layer a specific shape (or
filter) and then estimating its hyper-parameters. The BMO plan-based anterior lamina cribrosa surface depth
(ALCSD) parameter was generated as the average perpendicular distance from ALCS relative to the BMO reference
plane along two of the 48 radial scans (one vertical (12:00 to 6:00) and one horizontal (9:00 to 3:00) scan. An
expert (ZY) manually marked the best 4 locations visible as the border of the ALCS on the vertical and horizontal
scan for a total of 8 points. We compared the ALCSD measurements using automated ALCS detection to those
obtained by expert manual segmentation. Glaucoma diagnostic accuracy [area under receiver operating
characteristic (AUROC)] was estimated using 20 glaucoma and 20 healthy eyes.
Results: The BMO plan-based ALCSD measurements with the new deconvolution approach using Spectralis EDI
radial scans were similar to expert measurements (Figure 1). The correlations between the manual and the automated
measurements was R2 = 0.95 (p <0.001). The diagnostic accuracy of ALCSD for differentiating between healthy and
glaucoma eyes in this limited sample was AUROC = 0.78 (0.62-0.93). Identification of the ALCS was particularly
challenging when the radial scan dissects large vessels and when there is a shallow optic cup.
Conclusions: This deconvolution segmentation method shows promise for automated identification of the
ALCS. The clinical importance of this measurement should be evaluated in a larger longitudinal sample of
glaucoma and healthy eyes.
46
Commercial Relationships Disclosure (Abstract): Akram Belghith: Commercial Relationship: Code N (No
Commercial Relationship) | Christopher Bowd: Commercial Relationship: Code N (No Commercial Relationship) |
Zhiyong Yang: Commercial Relationship: Code N (No Commercial Relationship) | Felipe Medeiros: Commercial
Relationship(s);Alcon Laboratories Inc.:Code F (Financial Support);Bausch & Lom:Code F (Financial Support);Carl
Zeiss Meditec Inc.:Code F (Financial Support);Heidelberg Engineering, Inc:Code F (Financial Support);Merck
Inc:Code F (Financial Support);Allergan Inc:Code F (Financial Support);Sensimed:Code F (Financial
Support);Topcon, Inc:Code F(Financial Support);Reichert, Inc:Code F (Financial Support);National Eye
Institute:Code F (Financial Support);Alcon Laboratories Inc:Code P (Patent);Allergan Inc:Code P (Patent);Carl
Zeiss Meditec Inc:Code P (Patent);Reichert Inc.:Code P (Patent);Allergan, Inc:Code C (Consultant);Carl-Zeiss
Meditec, Inc:Code C (Consultant);Novartis:Code C (Consultant) | Robert Weinreb: Commercial
Relationship(s);Aerie:Code F (Financial Support); Carl Zeiss Meditec:Code F (Financial Support); Genentech:Code
F (Financial Support);Heidelberg Engineering GmbH:Code F(Financial Support);National Eye Institute:Code F
(Financial Support);Nidek:Code F (Financial Support); Novartis:Code F (Financial Support);Optovue:Code F
(Financial Support);Topcon:Code F (Financial Support);Alcon:Code C (Consultant);Allergan:Code C
(Consultant);Amkem:Code C (Consultant);Bausch&Lomb:Code C (Consultant);Carl Zeiss Meditec:Code C
(Consultant);EyeTechCare:Code C (Consultant);Quark:Code C (Consultant);Sensimed:Code C
(Consultant);Topcon:Code C (Consultant);Solx:Code C (Consultant) | Linda Zangwill:Commercial
Relationship(s);Carl Zeiss Meditec Inc:Code F (Financial Support);Heidelberg Engineering GmbH:Code F
(Financial Support);Optovue Inc:Code F (Financial Support);Topcon Medical Systems Inc:Code F (Financial
Support);Topcon Medical Systems Inc:Code R (Recipient)
47
02:15 PM-02:30 PM
Program Number: 18
Magic Angle-Enhanced MRI of Fibrous Structures in the Eye upon Intraocular Pressure Loading
Author(s): Leon C. Ho1, 2, Ian A. Sigal1, 3, Ning-Jiun Jan1, 3, Alexander Squires4, Zion Tse4, Ed X. Wu2, Seong-Gi
Kim3, 5, Joel S. Schuman1, Kevin C. Chan1, 3
1
University of Pittsburgh, 2The University of Hong Kong, 3University of Pittsburgh, 4The University of Georgia,
5
SKKU
Purpose: The sclera and cornea are collagenous fibrous connective tissues that are central to several eye diseases
such as glaucoma and myopia. Their roles on disease pathogenesis however remain unclear, partly due to limited
non-invasive techniques to assess and monitor these fibrous structures globally, longitudinally and quantitatively.
Magic angle-enhanced MRI has been used clinically to evaluate collagenous fibers in normal and diseased tendons,
ligaments and cartilages in vivo. We hypothesized that magic angle-enhanced MRI can detect changes in
corneoscleral shell tissues due to intraocular pressure (IOP) alternation.
Methods: Seven pairs of ovine eyes were extracted and fixed. One eye from each sheep was loaded at
IOP=50mmHg to mimic ocular hypertension, and the contralateral eye was unpressurized. The sclera and cornea
were aligned at different angular orientations relative to the static magnetic field (B o) inside a 9.4Tesla MRI scanner.
T2 and T2* mapping using spin-echo (SE) and gradient-echo (GE) MRI was applied to quantify the magic angle
effect on the corneoscleral shells.
Results: SE and GE signal intensities were found to be maximal when the tissues were oriented near the magic
angle at ~55o to Bo. Such magic angle enhancement was stronger in GE than SE MRI, while higher T2- and T2*weighted signal intensities were found in loaded than unloaded ocular tissues at magic angle (Figure), suggestive of
rearrangement of the collagen fibers. Transverse relaxation times in loaded sclera (T2=31.5±4.2ms and
T2*=11.3±1.4ms) were significantly higher than unloaded sclera at the magic angle (T2= 24.5±5.2ms and
T2*=9.0±2.0ms) (p<0.05). T2 (41.9±17.7ms) and T2* (32.0±8.4ms) of loaded cornea were also significantly higher
than unloaded cornea (T2=31.6±10.5ms and T2*=24.0±12.6ms) (p<0.05).
Conclusions: Magic angle-enhanced SE and GE MRI can detect and quantify differences in ocular fibrous
structures upon IOP loading. This technique may open up new avenues for non-invasive and longitudinal
assessments of the biomechanics and biochemistry of ocular tissues in aging and in diseases involving the
corneoscleral shell.
Representative gradient-echo T2*-weighted MR images of the sclera (left) and cornea (right) with (red arrows) or
without (blue arrows) IOP loading at 50mmHg. The green boxes indicate the tissue sections oriented near the magic
angle at ~55o to Bo.
48
Commercial Relationships Disclosure (Abstract): Leon Ho: Commercial Relationship: Code N (No Commercial
Relationship) | Ian Sigal: Commercial Relationship: Code N (No Commercial Relationship) | Ning-Jiun Jan:
Commercial Relationship: Code N (No Commercial Relationship) | Alexander Squires: Commercial Relationship:
Code N (No Commercial Relationship) | Zion Tse: Commercial Relationship: Code N (No Commercial
Relationship) | Ed Wu: Commercial Relationship: Code N (No Commercial Relationship) | Seong-Gi Kim:
Commercial Relationship: Code N (No Commercial Relationship) | Joel Schuman: Commercial
Relationship(s);Zeiss, Inc.:Code P (Patent) | Kevin Chan: Commercial Relationship: Code N (No Commercial
Relationship)
49
02:30 PM-02:45 PM
Program Number: 19
Accuracy of a Method for Measuring Micron-Scale Collagen Fiber Orientation
Author(s): Ning-Jiun Jan1, 2, Jonathan L. Grimm2, Bo Wang1, 2, Kira Lathrop2, Huong Tran1, 2, Gadi Wollstein2,
Larry Kagemann2, Hiroshi Ishikawa2, Joel Schuman2, Ian A. Sigal2, 1
1
University of Pittsburgh, 2University of Pittsburgh
Purpose: Collagen fiber orientation is a critical factor in determining the biomechanical response to loading of
ocular tissues. Our goal was to determine the accuracy of a method to measure micron-scale fiber orientation.
Methods: Two cases were analyzed: a single fiber of nylon string and a region of a sheep’s lamina cribrosa (LC)
with multiple intertwining fibers. The nylon string was mounted to a glass slide, imaged using light microscopy
(Olympus BX60, 12-bit grayscale 1600x1200 pixels, 0.73 µm/pixel, 10x objective, NA 0.30), and analyzed to
determine local fiber orientation as previously described (Jan NJ, et al., ARVO E-Abstract 65, 2013). A spline trace
of the string was drawn and the interpolated orientation of the trace (Fig1A) was compared to the measured fiber
orientation (Fig1B). A sheep eye (<2 yo) was fixed in formalin (10%) within 24 hours of death. Following fixation
the optic nerve head was cryosectioned coronally (30 µm). A section through the LC was selected and imaged 17
times, as above, with the sample rotated between 0° and 80°. Fiber orientation was computed and the known sample
orientation subtracted. Accuracy was computed by comparing the “true orientation change” with the fiber angle
change measured at every pixel (Fig2A).
Results: For a single fiber, the angle differences between the spline trace and measured orientation were within ±1°
(Fig1C). For the LC, the mean angle differences between the true and measured orientation changes were within ±1°
(Fig2B).
Conclusions: Our method was highly accurate for single and multiple intertwining fibers, enabling accurate fiber
tracing and detection of fiber orientation changes. Future work will involve applying this method to measure
micron-scale biomechanics of the eye.
Measuring Accuracy in a Single Fiber A) The nylon fiber with the trace overlaid in red. B) An image of the
measured fiber orientation of the string, with the color representing the angle. C) A Bland-Altman plot of the angle
differences between the trace and measured angle. The lines above and below represent the 95 th percentile.
50
Measuring Accuracy in Tissue with Intertwining Fibers A) The region of sheep LC used for analysis. B) Box plots
of the distribution of differences between true and measured fiber orientation angle change computed at every pixel
in the image of panel A. The lines above and below represent the 95 th percentile.
Commercial Relationships Disclosure (Abstract): Ning-Jiun Jan: Commercial Relationship: Code N (No
Commercial Relationship) | Jonathan Grimm: Commercial Relationship: Code N (No Commercial Relationship) |
Bo Wang: Commercial Relationship: Code N (No Commercial Relationship) | Kira Lathrop: Commercial
Relationship: Code N (No Commercial Relationship) | Huong Tran: Commercial Relationship: Code N (No
Commercial Relationship) | Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) |
Larry Kagemann: Commercial Relationship: Code N (No Commercial Relationship) | Hiroshi Ishikawa:
Commercial Relationship: Code N (No Commercial Relationship) | Joel Schuman: Commercial Relationship: Code
N (No Commercial Relationship) | Ian Sigal: Commercial Relationship: Code N (No Commercial Relationship)
51
02:45 PM-03:00 PM
Program Number: 20
Automated identification of Schlemm’s canal and collector channels from spectral domain optical coherence
tomography images.
Author(s): Siamak Yousefi1, Amir Marvasti3, Robert N. Weinreb1, Christopher Bowd1, Alex Huang2
1
Hamilton Glaucoma Center, 2USC Eye Institute, 3Boston University
Purpose: To develop an algorithm for automated detection of human Schlemm’s canal (SC) and collector channels
(CC) from in vivo SDOCT images.
Methods: SDOCT images were collected from the right eye of a healthy subject using the Spectralis Anterior
Segment lens (Heidelberg Engineering, Heidelberg, Germany). Two separate volumes were obtained along the
temporal portion of the eye, each consisting of a sequence of 81 consecutive axial 2D slices at the limbus. Axial
resolution of each A-scan was 3.9 µm with a lateral resolution of 11 µm and distance between B-scans of
11 µm. The image processing pipeline for detecting SC, CC and outflow pathways had four main steps: 1) an
algorithm was applied to identify the region around the intersection of cornea and iris (region of interest, ROI), 2) an
algorithm was applied to the ROI to detect SC/CC, 3) an object detection algorithm was applied to identify SC/CC,
and 4) all identified SC/CC and the tissue boundaries were fused for visualization. Each image-processing step
included several preprocessing tasks including noise reduction, binarization (using minimization of intra-class
variance of the background and object pixels), morphology based object analysis, and shape analysis. Images were
then analyzed for detection rate. For each 2D slice, detection was stratified along three criteria: (a) good detection
(Fig. 1a; >50% of the visualized SC/CC was identified by the algorithm; arrow), (b) detection (Fig. 1b; ≤50% of the
visualized SC/CC was identified by the algorithm; arrow is detected portion and arrowhead is undetected portion),
and (c) no detection (Fig. 1c; failure to identify SC/CC; arrowhead).
Results: In volume 1, SC/CC were successfully identified in 93% of SDOCT 2D images with a good detection rate
of 60%. In volume 2, SC/CC were successfully identified in 91% of SDOCT 2D images with a good detection rate
of 62%. Errors in detection included failure to identify SC/CC, identification of extraneous locations (Fig. 1c), and
identification within the choroid (where pixel intensity levels paralleled that of SC/CC).
Conclusions: SC, CC, and outflow pathways from SDOCT in vivo images can be identified with great fidelity
using the proposed image processing pipeline.
52
Commercial Relationships Disclosure (Abstract): Siamak Yousefi: Commercial Relationship: Code N (No
Commercial Relationship) | Amir Marvasti: Commercial Relationship: Code N (No Commercial Relationship) |
Robert Weinreb: Commercial Relationship(s);Aerie:Code F (Financial Support);;Alcon Laboratories:Code C
(Consultant);Allergan Inc:Code C (Consultant);Bausch & Lomb Inc.:Code C (Consultant);Carl Zeiss Meditec
Inc.:Code F (Financial Support);Carl Zeiss Meditec Inc.:Code C (Consultant);Genentech:Code F (Financial
Support);Heidelberg Engineering GmbH:Code F (Financial Support);National Eye Institute:Code F (Financial
Support);Novartis:Code F (Financial Support);Optovue Inc:Code F (Financial Support);Sensimed Inc:Code C
(Consultant);Topcon Inc.:Code C (Consultant);Topcon Inc.:Code F (Financial Support) | Christopher Bowd:
Commercial Relationship: Code N (No Commercial Relationship) | Alex Huang: Commercial Relationship: Code N
(No Commercial Relationship)
53
03:00 PM-03:15 PM
Program Number: 21
Functional Microvascular Imaging of the Conjunctiva: a noninvasive tool to measure and quantify subtle
variations and abnormalities in the microvasculature
Author(s): Delia Cabrera DeBuc1, Hong Jiang1, 2, Nicole Stuebiger3, Che Liu1, Tian Jing1, Gabor Mark Somfai4,
Janet Davis1, William E. Smiddy1, Jianhua Wang1
1
University of Miami, 2University of Miami, 3Charité Universitätsmedizin Berlin, 4Semmelweis University
Purpose: To demonstrate the advantages of functional microvascular imaging of the conjunctiva for clinical
applications where understanding of microvascular pathology may provide useful information for predicting the
onset, progression and prognosis of both systemic and central nervous system (CNS) vascular diseases.
Methods: The bulbar conjunctival vasculature was imaged using a retinal function imager (RFI, Optical Imaging
Ltd, Rehovot, Israel) and a novel functional slit-lamp biomicroscopy (FSLB) imaging device. Hemoglobin in red
blood cells was used as an intrinsic motion-contrast agent in the generation of detailed noninvasive capillaryperfusion maps (nCPMs) from RFI images, noninvasive microvascular perfusion maps (nMPMs) from FSLB
images and the calculation of the blood flow velocity. Oximetric state of the bulbar conjunctiva was qualitatively
investigated from multispectral images obtained with the RFI unit.
Results: The RFI and FSLB systems were successfully used to obtain and analyze the angiography of
conjunctival blood vessels from a pool of healthy controls and patients with diabetes w/o retinopathy (see Fig. 1),
retinal vasculitis of unknown origin, Birdshot chorioretinopathy, suspicion of glaucoma, cerebral small vessel
disease (CSVD) and multiple sclerosis. The bulbar conjunctival microvascular network was also investigated in
healthy subjects before and after wearing contact lenses The nCPMs obtained with the RFI showed the conjunctival
microvasculature in exquisite detail, however nMPMs showed higher-resolution angiography of conjunctival blood
vessels obtained with the FSLB device (see Fig. 2). Perfusion deficits and abnormalities were observed as an
indication of oximetric changes occurring after several types of challenges to the bulbar conjunctiva. Variations
between normal vessels and vessels exhibiting reduced red blood cell velocity were observed in pathological eyes.
Particularly, conjunctival vessel changes occurred even before non-proliferative retinopathy develops in diabetic
patients.
Conclusions: Detection of functional microvasculature abnormalities by direct, noninvasive enhanced
visualization of conjunctival vessels may permit diagnosis of diseases and disease progression before anatomic
abnormalities become evident, allowing treatment intervention before irreversible microvasculature damage occurs.
54
Commercial Relationships Disclosure (Abstract): Delia Cabrera DeBuc: Commercial Relationship(s);NIH/NEIEY020607:Code F (Financial Support);NIH R01EY020607S:Code F (Financial Support);NIH Center Core Grant
P30EY014801:Code F (Financial Support);US 61/139,082:Code P (Patent);University of Miami:Code P (Patent) |
Hong Jiang: Commercial Relationship(s);NIH/NEI-EY020607S:Code F (Financial Support);University of
Miami:Code P (Patent) | Nicole Stuebiger: Commercial Relationship: Code N (No Commercial Relationship) | Che
Liu: Commercial Relationship: Code N (No Commercial Relationship) | Tian Jing: Commercial
Relationship(s);NIH/NEI- EY020607:Code F (Financial Support) | Gabor Mark Somfai: Commercial Relationship:
Code N (No Commercial Relationship) | Janet Davis: Commercial Relationship: Code N (No Commercial
Relationship) | William Smiddy: Commercial Relationship: Code N (No Commercial Relationship) | Jianhua Wang:
Commercial Relationship(s);University of Miami:Code P (Patent)
55
03:15 PM-03:30 PM
Program Number: 22
Ultra-High Resolution Optical Coherence Tomography for the Differentiation of Ocular Surface Squamous
Neoplasia and Melanoma
Author(s): Juan Murillo, Anat Galor, Afshan A. Nanji, Madhura G. Joag, James R. Wong, Nabeel M. Shalabi,
Marwan Atallah, Ibrahim Sayed-Ahmed, Carol L. Karp
Bascom Palmer Eye Institute - University of Miami
Purpose: To asses the use of ultra-high-resolution optical coherence tomography (UHR-OCT) as a key diagnostic
tool in distinguishing ocular surface squamous neoplasia (OSSN) from melanoma of the conjunctiva. The
establishment of the correct diagnosis is crucial. OSSN usually follows a benign course whereas melanoma has a
very aggressive behavior with high mortality rates.
Methods: In this clinical case series, one hundred and eight eyes of 108 patients with conjunctival lesions: OSSN
and biopsy proven melanomas were recorded. Clinical features, slit-lamp photographs and UHR-OCT scans (RTVue
premier, Optovue, Fremont, CA, USA) are described.
Results: We evaluated 101 OSSN and 7 melanomas with UHR-OCT. In all cases the OSSN revealed a thickened
hyperreflective (whitish) epithelial layer often with an abrupt transition from normal to hyperreflective epithelium
(Figure 1). The mean epithelial thickness in the OSSN group was 233 ± 165 μm (range 72-1170). The melanoma
group, disclosed an overall thinner epithelium, with the presence of a subepithelial mass (Figure 2). The mean
epithelial thickness was 69 ± 29 μm (range of 35-117). Differences in the measured epithelial thickness on UHROCT between the two entities were statistically significant (p-value =0.01) to such a degree that a cutoff value of
86.5 microns was able to reliably differentiate melanoma from OSSN with a sensitivity of 94% and a specificity of
86%.
Conclusions: Ultra-high resolution OCT is a noninvasive novel diagnostic tool that is helpful in evaluating ocular
surface lesions. Morphologic features displayed by the UHR OCT can be an important adjunct in evaluating OSSN
and melanoma.
Figure 1. Clinical photos and UHR-OCT scans of ocular surface squamous neoplasia (OSSN). Figure 1A and 1B
demonstrate elevated, gelatinous limbal lesions and 1C shows a papilomatous limbal lesion. Figures 1D, 1E and 1F
display UHR-OCT images with a thickened hyperreflective epithelial layer (white arrows) and an abrupt transition
from normal to hyperreflective epithelium (black arrows).
56
Figure 2. Clinical photos and UHR-OCT scans of amelanotic conjunctival melanomas. Figure 2A, 2B and 2C
demonstrate raised, mostly nonpigmented, conjunctival lesions. Figure 2D, 2E and 2F show UHR-OCT images with
subepithelial lesions (black arrows) beneath a normal to mildly thickened epithelium (white arrows).
Commercial Relationships Disclosure (Abstract): Juan Murillo: Commercial Relationship: Code N (No
Commercial Relationship) | Anat Galor: Commercial Relationship(s);Bausch & Lomb:Code C (Consultant) | Afshan
Nanji: Commercial Relationship: Code N (No Commercial Relationship) | Madhura Joag: Commercial Relationship:
Code N (No Commercial Relationship) | James Wong: Commercial Relationship: Code N (No Commercial
Relationship) | Nabeel Shalabi: Commercial Relationship: Code N (No Commercial Relationship) | Marwan Atallah:
Commercial Relationship: Code N (No Commercial Relationship) | Ibrahim Sayed-Ahmed: Commercial
Relationship: Code N (No Commercial Relationship) | Carol Karp: Commercial Relationship(s);NIH Center Core
Grant P30EY014801, RPB Unrestricted Award and Career Development Awards, Department of Defense (DODGrant#W81XWH-09-1- 0675)The Ronald and Alicia Lepke Grant, The Lee and Claire Hager Grant, The Jimmy and
Gaye Bryan Grant.:Code F (Financial Support)
57
Novel Methods for Small
Animal Imaging
04:00 PM-05:30 PM
Moderators:
Yoshiaki Yasuno, PhD
Richard Rosen, PhD
58
04:00 PM-04:15 PM
Program Number: 23
Two-photon imaging of inner and outer retina in the living primate eye
Author(s): Robin Sharma4, 1, David R. Williams1, 4, Grazyna Palczewska2, Krzysztof Palczewski5, Jennifer Hunter3,
1
1
University of Rochester, 2Polgenix, Inc, 3University of Rochester, 4University of Rochester, 5Case Western Reserve
University
Purpose: Adaptive optics assisted two-photon imaging of the retina has the potential to simultaneously provide
structural as well as functional information from individual cells in the living eye. Previously, it was deployed to
capture intrinsic fluorescence from individual cone photoreceptors in the macaque eye. Our goal is to expand the
utility of this modality by imaging in vivo a broader range of cell types.
Methods: A two-photon adaptive optics scanning light ophthalmoscope was developed for imaging living primates.
For this study, two different macaques were imaged under isofluorane anaesthesia. An ultrashort pulsed laser (~ 55
fs pulse-width) with a tunable central wavelength was used to excite two-photon fluorescence. Images were acquired
at two different central wavelength settings (730 or 920 nm) using light levels that were below the threshold for
retinal damage with each acquisition (< 7 mW average power incident on the cornea). High signal-to-noise ratio
reflectance images were simultaneously acquired to correct for eye motion.
Results: Consistent with measurements made in excised retina, fluorescence emission was detected throughout the
retina in vivo. For 730 nm excitation, the strongest autofluorescence signal originated from near the photoreceptor
layer, whereas for 920 nm excitation, the brightest intrinsic fluorescence emanated from the retinal pigment
epithelium. Two-photon images of individual cells and other recognizable structures were obtained in multiple
retinal layers such as the nerve fiber bundles (at 730 nm), individual rods as well as cones (at 730 nm) and retinal
pigment epithelial cells (at 920 nm). During light exposure, autofluorescence signal from the inner retina increased
with time in a manner that was qualitatively similar to earlier results obtained in the outer retina.
Conclusions: It is possible to resolve single cells in retinal layers other than the photoreceptors using in vivo twophoton autofluorescence imaging. This is an important step towards noninvasively monitoring functional activity in
many individual retinal layers.
Commercial Relationships Disclosure (Abstract): Robin Sharma: Commercial Relationship(s);Canon, Inc. :Code
F (Financial Support) | David Williams: Commercial Relationship(s);Canon, Inc.:Code F (Financial
Support);Polgenix, Inc. :Code F (Financial Support);Pfizer:Code C (Consultant);University of Rochester:Code P
(Patent);Pfizer:Code R (Recipient) | Grazyna Palczewska: Commercial Relationship(s);Polgenix, Inc. :Code E
(Emplyment) | Krzysztof Palczewski: Commercial Relationship(s);Polgenix, Inc.:Code I (Personal Financial
Interest);Polgenix, Inc.:Code E (Emplyment);Polgenix, Inc.:Code P (Patent) | Jennifer Hunter: Commercial
Relationship(s);Canon, Inc.:Code F (Financial Support)
59
04:15 PM-04:30 PM
Program Number: 24
3D-imaging of Rat Retina Using Contrast Enhanced X-ray Microtomography
Author(s): Kalle Lehto2, 3, Ilmari Tamminen2, 3, Soile Nymark2, 3, Tanja Ilmarinen3, Hannu Uusitalo4, 5, Heli
Skottman3, Antti Aula2, 1, Jari Hyttinen2, 3
1
Imaging Centre, Tampere University Hospital, 2Tampere University of Technology, 3University of Tampere,
4
Tampere University Hospital, 5University of Tampere
Purpose: Present methods for preclinical imaging of animal retina are mostly limited to only a part of the retina.
High-resolution X-ray microtomography (µCT), enhanced with appropriate contrast agents, has been used for
imaging various soft tissues (Metscher 2009, Pauwels et al. 2013). In this study, we further developed contrast
enhanced μCT for ex vivo eye imaging and used the method for comparison of the anatomy in healthy and RCS rat
eyes.
Methods: Control (n=3) and RCS (n=3) rats (24 weeks old) were sacrificed and the eyes harvested, fixed in
Davidson's solution and dehydrated in ethanol. Before the imaging, the eyes were immersed in 15 ml of absolute
ethanol, augmented with 1% w/v iodine, for at least 10 days. The eyes were then scanned with a Xradia MicroXCT400 with scanning parameters 75kV/133µA. The achieved voxel size was 3.1 µm. Moreover, the area around the
optic nerve bundle was imaged with 1.2 µm voxel size. Reconstructed 3D image stacks were post-processed with
Avizo Fire 8.0.1 software (FEI Visualization Sciences Group). The images were filtered with edge-preserving nonlocal means filter and segmented by semi-automatic watershed algorithm with manual correction. Thickness of the
retina was calculated by using the specific surface thickness-function.
Results: Eight anatomical layers of retina were identified. Contrast enhanced µCT allowed high-resolution
imaging, visualization and morphological analysis of most of the eye tissues (Figure 1). Dystrophic changes in the
retina can be clearly assessed from the images (Figure 2). Overall thickness of the retina was 15% lower in the RCS
eyes.
Conclusions: Morphology of the ex vivo eye structures can be assessed quantitatively in 3D using μCT. The
acquired image sets can be used for 3D histology without physically sectioning the sample. However, the data can
be virtually sectioned in silico in any direction. Contrast enhanced µCT is a promising imaging modality for
preclinical ex vivo studies of the eye.
The whole eye (A) can be examined and analysed (B) with 3.1 µm voxel size. Moreover, specified regions of
interest, for example the optical nerve (C), can be zoomed into
60
Comparison of a histological section (top) and µCT images of healthy (middle) and dystrophic (bottom) eyes
showed the potential of µCT in preclinical studies of the eye anatomy. The loss of outer segments of the
photoreceptor layer is evident in the dystrophic eye (arrows).
Commercial Relationships Disclosure (Abstract): Kalle Lehto: Commercial Relationship: Code N (No
Commercial Relationship) | Ilmari Tamminen: Commercial Relationship: Code N (No Commercial Relationship) |
Soile Nymark: Commercial Relationship: Code N (No Commercial Relationship) | Tanja Ilmarinen: Commercial
Relationship: Code N (No Commercial Relationship) | Hannu Uusitalo: Commercial Relationship: Code N (No
Commercial Relationship) | Heli Skottman: Commercial Relationship: Code N (No Commercial Relationship) |
Antti Aula: Commercial Relationship: Code N (No Commercial Relationship) | Jari Hyttinen: Commercial
Relationship: Code N (No Commercial Relationship)
61
04:30 PM-04:45 PM
Program Number: 25
The Influence of Metabolism on Retinal OCT Imaging: What We’ve Learned from a Hibernating Animal
Model
Author(s): Brent A. Bell1, Yichao Li2, Fengyu Qiao3, Haohua Qian2, Joe G. Hollyfield1, Wei Li3
1
Cleveland Clinic, 2National Eye Institute, 3National Eye Institute
Purpose: To evaluate retinal changes in active and hibernating ground squirrels using a commercially available
ultra-high resolution Spectral Domain Optical Coherence Tomography (OCT) system.
Methods: Thirteen-lined ground squirrels (n=13) were imaged prior to, during, and after hibernation using a
Bioptigen Envisu R2200 UHR system with theoretical axial resolution <2µm. Post-mortem imaging was performed
on euthanized animals for comparison. Horizontal and vertical B-scans (20 frames by 1000 A-scans/B-scan) were
acquired ventral to the visual streak. Scans were coregistered and averaged in linear signal units. Absolute (ABS)
and ratiometric (RM) changes were analyzed from in-depth signal amplitudes of retinal lamina. Retinal morphology
was compared to published (Reme & Young, 1977) and acquired histomorphology data.
Results: Non-hibernating animals showed well-defined retinal lamina that correlated well with retinal histology.
Morphology appearance was identical in either B-scan orientation. Hibernation resulted in dramatic changes to
signal amplitude and image contrast, with no significant changes to thicknesses of any outer retinal layer relative to
non-hibernating conditions. Measurements of photoreceptor inner (20.8±1.5µm) and outer segments (6.5±1.1µm), as
well as dimensions of the myoid (~12µm) and ellipsoid (~8µm) regions were similar to published data. Choroidal
thickness was significantly reduced (44%, p=.0008) during torpor, but returned to normal by 1 hr posthibernation. Signal magnitude for a band at the ellipsoid (a region with high density of mitochondria) location
showed the greatest change (ABS-55%/RM-70%; p<.0001). On average, signal magnitudes were partially and fully
restored to pre-hibernation levels after 1-3 & 24 hours of recovery, respectively. Results from post-mortem animals
were similar to those observed in animals under awake and hibernating states.
Conclusions: The ground squirrel is a unique model for understanding the influence of metabolic activity on OCT
imaging. Retinal signal amplitude is substantially altered during hibernation yet rapidly returns post-hibernation.
The most dramatic changes occurred in the photoreceptor ellipsoid, which suggests that OCT is capable of
discerning differences in mitochondrial architecture, number or volume as a result of changing metabolic activity in
animals undergoing circannual hibernation.
62
Commercial Relationships Disclosure (Abstract): Brent Bell: Commercial Relationship: Code N (No Commercial
Relationship) | Yichao Li: Commercial Relationship: Code N (No Commercial Relationship) | Fengyu Qiao:
Commercial Relationship: Code N (No Commercial Relationship) | Haohua Qian: Commercial Relationship: Code
N
63
04:45 PM-05:00 PM
Program Number: 26
Spatial relationship between retinal loss and neurodegeneration of the visual system using optical coherence
tomography (OCT) and diffusion tensor MR imaging (DTI)
Author(s): Bo Wang1, 2, Leon C. Ho1, 3, Ian P. Conner1, 2, Richard A. Bilonick1, 4, Hiroshi Ishikawa1, 2, Amanda
Woodside1, Chieh-Li Chen1, Gadi Wollstein1, Joel S. Schuman1, 2, Kevin C. Chan1, 2
1
University of Pittsburgh School of Medicine, 2University of Pittsburgh, 3The University of Hong Kong, 4University
of Pittsburgh
Purpose: Recent studies have indicated the early involvement of degeneration along both anterior and posterior
visual pathways in ocular diseases and injuries. However, the spatial relationship between retinal damage and
neurodegeneration in the posterior visual pathway is not fully elucidated. In this study, we use OCT and DTI to
investigate the effects of retinal loss on neurodegeneration of the visual system in an N-methyl-D-aspartate
(NMDA)-induced rat model.
Methods: Four Sprague-Dawley rats (6 week old) were intravitreally injected with NMDA in the right eye, with the
left eye serving as an internal control. One month later, OCT volume scans centered on the optic nerve head were
taken and automatically segmented to determine total retinal thickness (TRT) along a band with inner and outer radii
of 0.39 and 0.49mm, respectively. DTI scans were taken in a 9.4 Tesla horizontal MRI scanner to assess the
microstructural integrity at the optic nerve and optic tract via 4 DTI parameters: fractional anisotropy (FA), axial
diffusivity (λ||), radial diffusivity (λ┴), and mean diffusivity (MD). Paired t-tests were used to determine the
difference between parameters in the visual pathways projected from injured and control eyes, and linear mixed
effects model was used to determine the relationships between NMDA treatment, TRT and DTI parameters.
Results: Mean TRT was 223±16μm for control eyes and 174±13μm for NMDA-injured eyes (p<0.01). TRT was
positively correlated with FA in both optic nerve and optic tract (p<0.05) and with λ|| in optic tract (p<0.05). TRT
was negatively correlated with λ┴ in optic nerve and optic tract (p<0.05) (Figure E). In general, correlation plots
between TRT and DTI parameters showed steeper slopes in optic nerve than in optic tract, with λ ┴ being
significantly steeper in optic nerve than optic tract (p<0.05).
Conclusions: OCT and DTI findings suggested that with retinal injury, there is 1) compromise of overall
microstructural integrity (decreased FA), 2) axonal damage (decreased λ ||) and 3) demyelination (increased λ┴) along
the visual pathway. Our results demonstrated the linear relationship between excitotoxic retinal injury and the
microstructural changes occurring in the brain in vivo, with more pronounced changes in DTI parameters closer to
the site of insult.
64
Commercial Relationships Disclosure (Abstract): Bo Wang: Commercial Relationship: Code N (No Commercial
Relationship) | Leon Ho: Commercial Relationship: Code N (No Commercial Relationship) | Ian Conner:
Commercial Relationship: Code N (No Commercial Relationship) | Richard Bilonick: Commercial Relationship:
Code N (No Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial
Relationship) | Amanda Woodside: Commercial Relationship: Code N (No Commercial Relationship) | Chieh-Li
Chen: Commercial Relationship: Code N (No Commercial Relationship) | Gadi Wollstein: Commercial
Relationship: Code N (No Commercial Relationship) | Joel Schuman: Commercial Relationship(s);Zeiss:Code P
(Patent) | Kevin Chan: Commercial Relationship: Code N (No Commercial Relationship)
65
05:00 PM-05:15 PM
Program Number: 27
Engineering of Gold Nanorods for Contrast-Enhanced Retinal OCT
Author(s): Andrew Gordon1, Jason Craft2, Ashwath Jayagopal1, 2
1
Vanderbilt University Medical Center, 2Vanderbilt Eye Institute
Purpose: Biocompatible exogenous contrast agents based on gold nanorods (GNR) were synthesized and
characterized for applications in retinal optical coherence tomography (OCT). Cell culture and animal models were
used to detect GNR uptake in specific retinal cell types.
Methods: GNR were synthesized with a surface plasmon resonance (SPR) within the 800-900 nm band, tuned to
interact with the light wavelengths emitted by the Bioptigen OCT system to generate image contrast. The monolayer
of cetyltrimethylammonium bromide (CTAB) found residually on the surface of GNR after their fabrication was
substituted with relatively biologically inert polyethylene glycol (PEG) monolayer to render them fully
biocompatible with ocular tissue. The PEG layer was modified to include an amine moiety that is amenable to
conjugation with GNR targeting ligands for targeting GNR to retinal cells in vivo. Surface modification of GNR and
GNR size were verified by electron microscopy, dynamic light scattering, mass spectrometry, and nuclear magnetic
resonance (NMR) spectroscopy. Retinal cells were analyzed in vitro for GNR binding and uptake, and C57BL/6J
mice were imaged in vivo following intraocular injection of GNR to image contrast enhancement of retinal layers
exhibiting GNR uptake.
Results: GNR size and PEG functionalization was verified, and GNR uptake into retinal cells in vitro was
confirmed using the aforementioned characterization technologies. Following intraocular injection of the PEGylated
GNR in mice, retinal contrast enhancement was observed using OCT. Targeting ligands enabled the detection of
retinal ganglion cell and endothelial cell biomarkers in animal models.
Conclusions: Previous work on fabricating OCT contrast agents for use in the eye also relied on GNR, but
encountered major limitations related to degradation of image quality secondary to the contrast agents’ cytotoxic and
inflammatory properties. In this report, a method for removing the cytotoxic CTAB layer from GNR provides a
route for clinically translatable OCT contrast agents used for detection of disease biomarkers and specific cell types
in the retina.
Commercial Relationships Disclosure (Abstract): Andrew Gordon: Commercial Relationship: Code N (No
Commercial Relationship) | Jason Craft: Commercial Relationship: Code N (No Commercial Relationship) |
Ashwath Jayagopal: Commercial Relationship: Code N (No Commercial Relationship)
66
05:15 PM-05:30 PM
Program Number: 28
The Effect of Microtubule-stabilizing Agents on the Retinal Ganglion Cell Axons Studied by SecondHarmonic Generation Microscopy
Author(s): Hyungsik Lim1, John Danias2
1
Hunter College, CUNY, 2SUNY Downstate Medical Center
Purpose: To demonstrate the utility of second-harmonic generation microscopy (SHGM) for evaluating the
efficacy of pharmacological treatments to stabilize and rescue the major cytoskeleton of axonal transport in the
retinal ganglion cells (RGCs)
Methods: A couple of common fixatives as well as microtubule-stabilizing agent (Taxol) were tested using the
retina of 4-week old Sprague-Dawley rats. The retinal flatmounts were prepared and treated with agents, while timelapse SHGM imaging was performed with circularly polarized excitation beam. The recorded microtubular SHG
(MT-SHG) emission was analyzed to examine the structural changes.
Results: The SHG signal from the retinal nerves gradually decreased due to postmortem dissociation of MTs and
the rate depended on the ambient conditions. Most chemical fixatives including 4% paraformaldehyde failed to
preserve the MT-SHG signal, whereas the retina treated with Taxol exhibited the arrest of signal reduction or even
increase in the MT-SHG emission at room temperature as well as 37 degree C.
Conclusions: We have demonstrated that the intensity of MT-SHG signal is sensitive only to the form of MT
structure that is physiologically active. Our results also show that the ensemble kinetics of MTs in the RGC axon
can be examined in the living tissue by SHGM without exogenous labeling, thus providing a practical means to test
the feasibility of MT recovery for restoring axonal transport which is known to be implicated in the progression of
glaucoma.
(Left) Topographic SHG imaging of the rat retina. (Right) SHG intensity from the fresh retinal nerves (N=4) when
Taxol is introduced at T=0.
Commercial Relationships Disclosure (Abstract): Hyungsik Lim: Commercial Relationship: Code N (No
Commercial Relationship) | John Danias: Commercial Relationship: Code N (No Commercial Relationship)
67
Poster Presentations
10:00 AM-10:30 AM
12:00 – 1:30 PM
3:30 – 4:00 PM
S 310E - H
68
201 Anterior Eye / Glaucoma
Poster Board Number: P1
Applications of photoacoustic tomography to imaging and estimation of oxygen saturation of hemoglobin in
ocular tissue of rabbits
Author(s): Stella Hennen1, 5, Wenxin Xing2, Ying-Bo Shui3, Yong Zhou2, Jennifer Kalishman 4, Lisa AndrewsKaminsky4, Michael Kass3, David Beebe3, Konstantin Maslov2, Lihong Wang2
1
Hennepin County Medical Center, 2School of Engineering and Applied Science, Washington University in St.
Louis, 3School of Medicine, Washington University in St. Louis, 4School of Medicine, Washington University in St.
Louis, 5School of Medicine, University of Minnesota
Purpose: To evaluate imaging capabilities and safety of measurements of oxygen saturation of hemoglobin (sO2) of
ocular tissue obtained with photoacoustic tomography (PAT) modality in rabbits in vivo.
Methods: Photoacoustic tomography (PAT) was used to collect images from the iris and ciliary body vasculature
(arteries and veins) of seven New Zealand White rabbits. The sO2 measurements were obtained under conditions of
relative hyperoxia, normoxia, or hypoxia. Systemic sO2 was monitored by pulse oximetry. Following imaging,
histological analysis of ocular tissue was conducted to evaluate for possible structural damage caused by the PAT
imaging.
Results: PAT was able to resolve anatomical structures of the anterior segment of the eye. Histological studies
revealed no ocular damage. On average, sO2 values obtained with PAT were lower than sO2 values obtained with
pulse oximetry (all p<0.001): 86.28±4.16 versus 99.25±0.28, 84.09±1.81 vs. 95.3±2.6, and 64.49±7.27 vs.
71.15±10.21 for hyperoxia, normoxia and hypoxia respectively.
Conclusions: PAT imaging modality is capable of providing in vivo sO2 measurements in rabbits. Further studies
are needed to modify the PAT modality specifically for use in humans. Having a safe non-invasive method of in
vivo imaging of sO2 is important to studies evaluating the role of oxidative damage in pathogenesis of ocular
diseases.
Commercial Relationships Disclosure (Abstract): Stella Hennen: Commercial Relationship: Code N (No
Commercial Relationship) | Wenxin Xing: Commercial Relationship: Code N (No Commercial Relationship) | YingBo Shui: Commercial Relationship: Code N (No Commercial Relationship) | Yong Zhou: Commercial Relationship:
Code N (No Commercial Relationship) | Jennifer Kalishman : Commercial Relationship: Code N (No Commercial
Relationship) | Lisa Andrews-Kaminsky: Commercial Relationship: Code N (No Commercial Relationship) |
Michael Kass: Commercial Relationship: Code N (No Commercial Relationship) | David Beebe: Commercial
Relationship: Code N (No Commercial Relationship) | Konstantin Maslov: Commercial
Relationship(s);Microphotoacoustics, Inc. and Endra, Inc.:Code P (Patent) | Lihong Wang: Commercial
Relationship(s);Microphotoacoustics, Inc. and Endra, Inc.:Code P (Patent)
69
Poster Board Number: P2
Quantitative MRI-derived optic nerve microstructural features in a feline glaucoma model
Author(s): Gillian J. McLellan1, 2, Samuel A. Hurley3, Pouria Mossahebi4, Norman M. Ellinwood6, Aaron S. Field5
1
University of Wisconsin-Madison, 2McPherson Eye Research Institute, 3University of Wisconsin-Madison,
4
University of Wisconsin-Madison, 5University of Wisconsin-Madison, 6Iowa State University
Purpose: To determine if quantitative MRI-derived microstructural features can detect optic nerve damage in a
feline glaucoma model
Methods: 6 adult cats (3 normal, 3 with primary congenital glaucoma[PCG]) were anesthetized with ketamine and
xylazine. Magnetic resonance imaging (MRI) was performed on a 3T GE Discovery MR750 (GE Healthcare,
Waukesha, WI) with an HD transmit/receive knee coil, with approval by the Institutional Animal Care and Use
Committee. Optic nerve images were acquired using a T2-weighted CUBE fast spin echo sequence (TR/TEeff = 3000
/ 80 ms, voxel dim = 234 x 234 x 800 µm3). Images were then rotated obliquely along each nerve, and crosssectional area measurements were performed using Jim 6.0 (Xinapse Systems, Colchester, UK). Microstructural
features were quantified using two spoiled gradient recalled echo (SPGR) images (TR = 30 ms, α = [4 24]°, dim =
375 x 375 x 800 µm3) and one magnetization transfer (MT)-weighted SPGR image (θ = 850°, ∆ = 4 kHz).
Correction for non-uniform RF transmit field was obtained using actual flip-angle imaging. These images were
analyzed using two different techniques: MTSat was used to quantify T1 [s] (a measure related to bulk water content
and microstructural integrity); simplified cross-relaxation imaging (CRI) was used to measure bound pool fraction f
[%] (a measure related to macromolecular content). Regions of interest (ROI) were drawn on each optic nerve just
anterior to the optic chiasm . The outer edge of pixels within the ROI were eroded to minimize partial volume
effects, and the average value of each parameter was computed. Comparisons between normal and PCG groups
were made by unpaired t-test, with p<0.05 considered significant.
Results: With the exception of T1 the parameters evaluated, including optic nerve cross sectional area, MTSat (%)
and f (%) were significantly lower in PCG relative to normal cats (see figure1)
Conclusions: Our findings indicate that MRI may be of value in the quantification of glaucomatous optic nerve
damage in vivo in this large animal glaucoma model but further studies will be necessary to determine inter-session
repeatability.
Figure 1: Magnetization transfer percentage saturation (MTSat; p=0.013) and bound pool fraction (f; p=0.015) were
significantly lower in glaucomatous (GL) than normal (CTRL) cats.
Commercial Relationships Disclosure (Abstract): Gillian McLellan: Commercial Relationship: Code N (No
Commercial Relationship) | Samuel Hurley: Commercial Relationship: Code N (No Commercial Relationship) |
Pouria Mossahebi: Commercial Relationship: Code N (No Commercial Relationship) | Norman Ellinwood:
Commercial Relationship: Code N (No Commercial Relationship) | Aaron Field: Commercial Relationship: Code N
(No Commercial Relationship)
70
Poster Board Number: P3
Analysis of the Cellular Dynamics of LysM-Positive Cells in a Corneal Suture Mouse Model using Intravital
Imaging
Author(s): Mayumi Ueta1, 2, Ayaka Koga1, 2, Masaru Ishii3, Shigeru Kinoshita1
1
Kyoto Prefectural University of Medicine, 2Faculty of Life and Medical Sciences, Doshisha University, 3Graduate
School of Medicine and Frontier Bioscience, Osaka University
Purpose: Corneal suture is a surgical procedure used to treat corneal trauma or for cases of corneal transplantation.
However, suture-related inflammatory cell infiltration (dynamics) in the cornea has yet to be analyzed in detail. In
LysM-eGFP mice, which are gene-targeted mice expressing enhanced green fluorescent protein (EGFP) under the
control of the endogenous lysozyme M promoter, myeloid granulocyte cells are labeled with GFP in vivo, and the
resulting endogenous neutrophils are brightly labeled. On the other hand, intravital imaging is a technique used to
analyze cellular and molecular dynamics stereoscopically and time-dependently in an in vivo animal model. In this
study, we analyze the dynamics of neutrophils in vivo in a LysM-eGFP corneal suture mouse model using intravital
imaging.
Methods: A 1-mm 10-1 nylon suture was surgically inserted through all layers in the center of the cornea of a
LysM-eGFP mouse. Dynamics of the LysM-positive granulocytes (neutrophils) were then analyzed in vivo using
intravital imaging. We also study the effect of steroid eye drops to infiltration of neutrophils due to the corneal
suture using fluorescence microscopy; after suture placement, each mouse was administered 5μL of phosphate
buffered saline (PBS) or steroid eye drops (0.1% betamethasone sodium phosphate ) 4 times daily. Moreover, we
study the alteration of dynamics of neutrophils due to suture removal.
Results: In the unsutured normal cornea (0 hours) of the LysM-eGFP mouse model, neutrophils were present in the
corneal stroma of only the limbal region. At 2 hours after insertion of the corneal suture, neutrophils migrated from
the limbal capillary loop to the cornea and conjunctiva, and reached the corneal suture at 6 hours after insertion. The
number of neutrophils then increased and peaked at 48 hours after insertion of the suture. At 72 hours after insertion,
infiltration of the neutrophils continued, yet decreased. Steroid eye-drop instillation produced no inhibitory effect on
neutrophil infiltration into the cornea. Neutrophils disappeared post suture removal.
Conclusions: Corneal suturing is a necessary procedure in some situations. In this study, we found that a corneal
suture causes infiltration of neutrophils into the cornea. It is important to understand that due to placement of a
corneal suture, inflammatory cells such as neutrophils will infiltrate into the cornea.
Commercial Relationships Disclosure (Abstract): Mayumi Ueta: Commercial Relationship: Code N (No
Commercial Relationship) | Ayaka Koga: Commercial Relationship: Code N (No Commercial Relationship) |
Masaru Ishii: Commercial Relationship: Code N (No Commercial Relationship) | Shigeru Kinoshita: Commercial
Relationship: Code N (No Commercial Relationship)
71
Poster Board Number: P4
Optical coherence tomography imaging to assist the iMvalv prototype development
Author(s): Rodrigo M. Torres1, 3, Diego Ramirez Arduh1, Fabio A. Guarnieri2
1
Centro de Ojos Dr. Lódolo, 2Facultad de Ingenieria, Universidad Nacional de Entre Ríos, 3Facultad de Ingenieria,
Universidad Nacional de Entre Ríos
Purpose: The iMvalv is a new concept to modulate and control the ocular fluids dynamics. The main potential
function is for glaucoma, as a micro-valve, but with an active mechanism (increase or decrease aqueous humor
outflow) based on MEMS technology. The Purpose of this study is to evaluate the potential usefulness of the optical
coherence tomography (OCT) as another tool for designing the iMvalv prototype.
Methods: An experimental in-vitro surgery was performed to implant the iMvalv in a porcine-eye. Basically, after
the conjunctiva and tenon were opened at the limbus to create a pocket, the device was placed in and the tube was
introduced in the anterior chamber. The iMvalv was built with silicone multiple layers. A Stratus OCT was utilized
to take the images captures, with the anterior segment mode (3.0 scan length). A second experiment was performed
with a sole iMvalv prototype (non implanted valve), which was OCT scanned to evaluate his plate.
Results: The OCT could show the tube and lumen of the iMvalv (Image 1). It could be observed into the anterior
segment porcine-eye, as well as the cornea and the iris, with great detail. To evaluate the iMvalv plate, the OCT
images were obtained from the non-implanted micro-valve, where anterior chamber tube, plate and drainage tube
could be observed (Image 2); inside this plate reside his MEMS technology to increase or decrease aqueous humor
flow.
Conclusions: The OCT anterior segment scan was useful to obtain images from the iMvalv different parts. The
iMvalv device design is in evolution and the OCT technology is another tool to evaluate it, as this study shows. To
evaluate his internal active mechanism, OCT evaluation will be added for a future in-vitro experimental set-up
study.
Image 1.
72
Image 2.
Commercial Relationships Disclosure (Abstract): Rodrigo Torres: Commercial Relationship: Code N (No
Commercial Relationship) | Diego Ramirez Arduh: Commercial Relationship: Code N (No Commercial
Relationship) | Fabio Guarnieri: Commercial Relationship: Code N (No Commercial Relationship)
73
Poster Board Number: P5
MRI, CT, and UBM imaging after corneal and cataract surgery
Author(s): Sotiria Palioura1, James Chodosh1, Lois Hart1, Karen Capaccioli1, Daniel Ginat2, Suzanne Freitag1
1
Massachusetts Eye and Ear Infirmary, 2The University of Chicago
Purpose: To report on the imaging characteristics of intraocular changes and complications after corneal and
cataract surgery as seen in computed tomography (CT) and magnetic resonance imaging (MRI) scans of the orbits
and correlate them with ultrasound biomicroscopy (UBM) images of the anterior segment.
Methods: CT and MRI images were collected from the records of the Massachusetts Eye and Ear Infirmary and
Massachusetts General Hospital neuroradiology departments. UBM images were obtained at the ultrasonography
suite of the Massachusetts Eye and Ear Infirmary. Only images of post-surgical changes or complications were
included.
Results: CT images include complications after penetrating keratoplasty and after Boston keratoprosthesis type I or
II implantation such as expulsive suprachoroidal hemorrhage, endophthalmitis, vitreous hemorrhage, and inclusion
cyst formation under surgically closed eyelids. The normal appearance of the Boston keratoprosthesis type I and II
devices on CT and UBM imaging is also discussed. Complications after cataract surgery including lens dislocation,
retained lens cortex, pseudophakic angle closure, and dystrophic calcification of the lens implant are presented as
seen in CT, MRI and UBM images. Finally, MRI images of a normal lens, a posterior chamber intraocular lens
implant, and absence of a lens (aphakia) are discussed.
Conclusions: We correlate imaging features of changes or complications after corneal or cataract surgery as seen
via various imaging modalities (CT, MRI, UBM) and aim to familiarize radiologists and ophthalmologists with such
findings.
Commercial Relationships Disclosure (Abstract): Sotiria Palioura: Commercial Relationship: Code N (No
Commercial Relationship) | James Chodosh: Commercial Relationship: Code N (No Commercial Relationship) |
Lois Hart: Commercial Relationship: Code N (No Commercial Relationship) | Karen Capaccioli: Commercial
Relationship: Code N (No Commercial Relationship) | Daniel Ginat: Commercial Relationship: Code N (No
Commercial Relationship) | Suzanne Freitag: Commercial Relationship: Code N (No Commercial Relationship)
74
Poster Board Number: P6
Rates of Glaucoma Progression as Detected by Optical Coherence Tomography (OCT) and Heidelberg
Retinal Tomography (HRT) in a Long-Term Cohort
Author(s): Divya Narendra1, Gadi Wollstein1, Dingle Foote1, Yun Ling1, 2, Richard A. Bilonick1, 2, Hiroshi
Ishikawa1, 3, Larry Kagemann1, 3, Cynthia Mattox4, James G. Fujimoto5, Joel S. Schuman1, 3
1
UPMC Eye Center, Eye and Ear Institute, Ophthalmology and Visual Science Research Center, Department of
Ophthalmology, University of Pittsburgh School of Medicine, 2Department of Biostatistics, Graduate School of
Public Health, University of Pittsburgh, 3Department of Bioengineering, Swanson School of Engineering, University
of Pittsburgh, 4New England Eye Center, Tufts Medical Center, 5Department of Electrical Engineering and
Computer Science, Massachusetts Institute of Technology
Purpose: Mean retinal nerve fiber layer (RNFL) thickness and neuroretinal rim area are commonly used parameters
in OCT and HRT, respectively, for assessing glaucoma progression. Prior studies comparing these devices have
typically been limited by short duration of follow-up in a slowly progressing disease. The Purpose of this study is to
examine, in a long-term cohort, the correspondence between OCT and HRT in regards to progression events and
rates of change as determined by mean circumpapillary RNFL and rim area.
Methods: 90 eyes (23 healthy (H), 20 glaucoma suspect (GS), 47 glaucoma (G)) from 52 subjects with at least five
reliable tests for each OCT and HRT. Measurements from four generations of OCT were standardized by applying
calibration equations. OCT and HRT progression was defined as significant negative slope on two consecutive
visits. Mean RNFL and rim area values were standardized as proportions to that eye’s baseline measurements to
allow direct comparison. Mean rates of change for these parameters were computed and compared for H, GS, and G
subjects, as well as for OCT and HRT progressors.
Results: Median follow-up time for the cohort was 6.9 years (range 3.3-13.0). 15 eyes showed OCT progression
and 19 eyes showed HRT progression. Of these, 6 eyes showed progression by both Methods . Of these dual
progressors, 5 eyes progressed by OCT then by HRT with median lag time of 2.9 years (range 1.1-5.6), and 1 eye
progressed by HRT then by OCT with lag time of 1.7 years. Among G subjects, slope for rim area was steeper than
that for RNFL (-0.015, -0.004; p<0.05). There was no difference in rim area and RNFL slopes among GS (0.0001,
0.002; p>0.5) and H subjects (-0.002, -0.002; p>0.5). Among HRT progressors, slope for rim area was steeper than
that for RNFL (-0.019, -0.002; p<0.05). However, for OCT progressors, there was no difference in rim area and
RNFL slopes (-0.023, -0.019; p>0.05).
Conclusions: Despite long-term follow-up with OCT and HRT, there were conflicting outcomes in regards to eyes
defined as progressing and rates of change among progressors. More eyes progressed by HRT than by OCT, but of
eyes that progressed by both, most progressed initially by OCT. Additionally, HRT progressors had a steeper slope
for rim area compared with mean RNFL, but for OCT progressors there was no difference in the slopes for the two
parameters.
Commercial Relationships Disclosure (Abstract): Divya Narendra: Commercial Relationship: Code N (No
Commercial Relationship) | Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) |
Dingle Foote: Commercial Relationship: Code N (No Commercial Relationship) | Yun Ling: Commercial
Relationship: Code N (No Commercial Relationship) | Richard Bilonick: Commercial Relationship: Code N (No
Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial Relationship) |
Larry Kagemann: Commercial Relationship: Code N (No Commercial Relationship) | Cynthia Mattox: Commercial
Relationship: Code N (No Commercial Relationship) | James Fujimoto: Commercial Relationship(s);Zeiss:Code P
(Patent);Optovue:Code P (Patent);Optovue:Code I (Personal Financial Interest) | Joel Schuman: Commercial
Relationship(s);Zeiss:Code P (Patent)
75
Poster Board Number: P7
Estimation of Trabecular Meshwork Thickness by Area and Width Measurements
Author(s): Larry Kagemann1, 2, Hiroshi Ishikawa1, 2, Gadi Wollstein1, Bo Wang1, 2, Yun Ling1, 3, Richard A.
Bilonick1, 3, Joel S. Schuman1, 3
1
University of Pittsburgh, 2University of Pittsburgh, 3University of Pittsburgh
Purpose: Irregularities in the morphology of the inner wall of Schlemm’s canal (SC) create challenges when
measuring trabecular meshwork (TM) thickness. A series of linear measurements may be obtained throughout the
various thicknesses of TM and averaged, though this is an arduous time-consuming process. A faster estimate of
TM thickness may be obtained by measuring TM area and dividing by width. The Purpose: of the present study was
to compare a calculation of trabecular meshwork thickness from an area measurement with direct linear
measurements.
Methods: The temporal limbus of six eyes (3 subjects) was imaged by spectral-domain optical coherence
tomography (Cirrus HD-OCT, Zeiss, USA) at baseline and at three intraocular pressure (IOP) levels. Additionally,
3 of the 6 eyes were imaged after dilation. TM thickness in 10 randomly selected B-scans in each of the 28 volumes
was measured by two techniques: 1- linear samples between the SC and anterior chamber were obtained and
averaged, and 2- TM area between SC and the anterior chamber was measured, as was the width (Figure, left and
right, respectively). TM thickness was estimated as the area divided by the width. The time required to measure
and record TM thickness for each method was measured and recorded for a subset of 30 B-scans. TM thickness
measurements by the two techniques were compared by linear mixed-effects modeling and Pearson’s correlation
coefficient.
Results: Analysis times of the area and linear techniques 27±3 and 42±6 seconds per B-scan. There was no
significant difference between TM thickness measurements obtained by the two Methods. Measurements obtained
by the line sample and area Methods were highly correlated (figure).
Conclusions: The analysis time for TM thickness measurements can be reduced using the area and diameter
technique with no appreciable difference in the estimate of TM thickness.
76
Commercial Relationships Disclosure (Abstract): Larry Kagemann: Commercial Relationship: Code N (No
Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial Relationship) |
Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) | Bo Wang: Commercial
Relationship: Code N (No Commercial Relationship) | Yun Ling: Commercial Relationship: Code N (No
Commercial Relationship) | Richard Bilonick: Commercial Relationship: Code N (No Commercial Relationship) |
Joel Schuman: Commercial Relationship(s);Zeiss, Inc:Code P (Patent)
77
Poster Board Number: P8
Predicting Future Observations of Functional and Structural Measurements in Glaucoma Using a TwoDimensional State-based Progression Model
Author(s): Yu-Ying Liu1, Hiroshi Ishikawa2, 3, Gadi Wollstein2, Richard A. Bilonick2, 4, James G. Fujimoto5,
Cynthia Mattox6, Jay S. Duker6, Joel S. Schuman2, 3, James M. Rehg1
1
Georgia Institute of Technology, 2UPMC Eye Center, Eye and Ear Institute, Ophthalmology and Visual Science
Research Center, Department of Ophthalmology, University of Pittsburgh School of Medicine, 3Department of
Bioengineering, Swanson School of Engineering, University of Pittsburgh, 4Department of Biostatistics, Graduate
School of Public Health, University of Pittsburgh, 5Department of Electrical Engineering and Computer Science,
Massachusetts Institute of Technology, 6New England Eye Center, Tufts Medical Center
Purpose: To evaluate the predictive performance of a novel progression analysis method based on two-dimensional
(2D) state-based longitudinal models accounting for both structural and functional components.
Methods: 81 glaucomatous eyes from 46 patients were followed for an average of 12.4 +- 4.3 years, and each eye
has at least 6 visits (average 8.5 +- 2.9 visits). Visual field index (VFI; Humphrey Field Analyzer; Zeiss) and optical
coherence tomography (OCT) global mean circumpapillary retinal nerve fiber layer (RNFL) thickness from multiple
generation of OCT (proprietary prototype OCT, OCT 1 and 2, Stratus OCT, Cirrus OCT (Zeiss)) were measured at
every visit. Calibration equations were employed to normalize RNFL thickness measurements across OCT machines
as a one-parameter continuum. A 2D continuous-time Hidden Markov Model using VFI and mean RNFL thickness
for 2D disease state definition was employed to model progression. In evaluating predictive performance, 10-fold
cross validation was used for model training and testing. In testing, the first 5 visits data were used to decode the
underlying disease states. Then, prediction for the future observations was based on the learned model. The same
setting was done for conventional linear regression estimates, where the slopes from the first 5 visits were used for
prediction. The mean absolute error (MAE) between the predicted values and the actual measurements along the
future follow-up period was used for performance assessment.
Results: The 2D state-based method performs significantly better than linear regression in predicting future VFI
(MAE: 4.88 +- 8.44 vs. 5.95 +- 9.79, respectively; t-test, P<0.001) and RNFL thickness values (MAE: 8.25 +- 7.89
vs. 16.34 +- 19.65, respectively; t-test, P<0.001).
Conclusions: The proposed novel 2D state-based progression analysis integrating structural and functional
information and modeling their temporal dynamics resulted in more accurate estimates of future observations (VFI
and RNFL thickness) compared to the conventional linear regression method.
78
Examples of prediction results using the 2D CT-HMM method
Commercial Relationships Disclosure (Abstract): Yu-Ying Liu: Commercial Relationship: Code N (No
Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial Relationship) |
Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) | Richard Bilonick: Commercial
Relationship: Code N (No Commercial Relationship) | James Fujimoto: Commercial Relationship(s);Zeiss:Code P
(Patent);Zeiss:Code C(Consultant) | Cynthia Mattox: Commercial Relationship: Code N (No Commercial
Relationship) | Jay Duker: Commercial Relationship: Code N (No Commercial Relationship) | Joel Schuman:
Commercial Relationship(s);Zeiss:Code P (Patent);Zeiss:Code C (Consultant) | James Rehg: Commercial
Relationship: Code N (No Commercial Relationship)
79
Poster Board Number: P9
Assessment of retinal nerve fiber layer with color and red free images using Smartscope Fundus Camera
Author(s): Ramesh S Ve, Krithica Srinivasan
Department of Optometry, School of Allied Health Sciences, Manipal, Karnataka, India.
Purpose: Smartscope (Optomed Oy, Finland) is a handheld non-mydriatic fundus camera using an IR-LED system
and 5MPixel image sensor to image central 30°of retina. We compared the retinal nerve fiber layer (RNFL) based on
color and red free images taken on single exposure using Smartscope Fundus Camera.
Methods: 56 pairs of retinal images of 38 patients were enrolled from the eye clinic at Dr TMA Pai hospital,
Udupi, India. All subjects underwent a comprehensive eye examination including retinal imaging using retinal
module EY3-Optomed SmartscopeM5. Subjects with visually significant cataract, history of trauma and ocular
surgery were excluded. Images with poor centration and artifacts were also excluded. RNFL appearance in both
Color and Redfree (RF) images was graded based on reflectance into 1. Inferior, Superior, Nasal and Temporal
(ISNT) pattern and 2. Split nerve fiber layer (SpNFL) pattern (in any quadrant). The disc area (DA) and RNFL area
(Superior, inferior) was measured based on reflectivity using image analyzing software (Cy-Pacs, Cynaptix Pvt Ltd,
India) in both sets of images. Measurements were made by a blinded observer and the color or redfree images were
randomly presented.
Results: 112 retinal images (56 pairs) with the mean DA of 2.57 mm2 (SD 0.52, min 1.49, max 4.43) were
analysed. The mean difference in DA (0.04, SD 0.46) mm2 between color and RF images was not statistically
significant (p=0.558, 95% CI of diff -0.08 to 0.16). Appearance of ISNT pattern between the color and RF images
matched in 91% of eyes. SpNFL pattern was observed in 20 (35.71%, 95 CI 23.68 to 49.70) images. The mean DA
for color and RF images were 2.56 (SD 0.52) and 2.53 (0.49) respectively, this was not statistically significant
(p=0.558, 95% CI of diff -0.08 to 0.16). There was no significant difference in the RNFL thickness across superior
RNFL (mean diff 0.17, SD 0.95, p=0.185, 95% CI of diff -0.08 to 0.42) and inferior RNFL (mean diff 0.23, SD
1.10, p=0.130, 95% CI of diff -0.07 to 0.52) regions between the images types.
Conclusions: Retinal nerve fiber assessment with color images and red-free images showed good agreement taken
using retinal module EY3 of Optomed Smartscope camera.
Commercial Relationships Disclosure (Abstract): Ramesh S Ve: Commercial Relationship: Code N (No
Commercial Relationship) | Krithica Srinivasan: Commercial Relationship: Code N (No Commercial Relationship)
80
Poster Board Number: P10
Confocal microscopy for the analysis of the sub-basal corneal nerves
Author(s): Madhura G. Joag1, Anat Galor2, 1, Nabeel M. Shalabi2, 1, James R. Wong1, Juan Murillo1, Afshan A.
Nanji1, Marwan Atallah1, Parke Green3, Mauro Campigotto4, Carol L. Karp1
1
Bascom Palmer Eye Institute, University of Miami, Miller School of Medicine, 2Miami Veterans Affairs Medical
Center, 3Nidek Inc, 4Nidek Technologies Srl
Purpose: To evaluate a new software technology that can quantify sub-basal nerve plexus parameters in confocal
microscopy. Using the ConfoScan 4 (Nidek Technologies Srl, Padova, Italy)
Methods: Eight healthy volunteers with no prior ocular diseases or surgeries were scanned using the 40x lens on
the ConfoScan 4. A single good quality image was then run through the Corneal Nerve Analysis tool, a new
automated nerve analysis software program.
Results: Median patient age was 58.5 years (range 34-77). The median length density (μm/mm2) in our 8 patients
was 11389.82 μm/mm2 (range 9278.36- 16232.29). No relationship was found between density and age (r=0.126) A
manual inspection of the images demonstrated that the software was able to detect and capture the sub-basal nerves
in each scan accurately. The median length density is similar to the three previous studies in which the manually
calculated mean nerve density was found to be 11415 μm/mm2 (range 8404- 14,731) (n=139).
Conclusions: The Nerve Analysis Tool is a potentially valuable tool for analysis of sub-basal nerves. Future study
is needed to assess reliability and repeatability of this software technology and its application to ocular surface
pathologies.
Figure1: (A) Preprocessing Image of subbasal nerves. (B) Post processing Image of subbasal nerves (C) Output
parameters of Image B
Commercial Relationships Disclosure (Abstract): Madhura Joag: Commercial Relationship: Code N (No
Commercial Relationship) | Anat Galor: Commercial Relationship: Code N (No Commercial Relationship) | Nabeel
Shalabi: Commercial Relationship: Code N (No Commercial Relationship) | James Wong: Commercial
Relationship: Code N (No Commercial Relationship) | Juan Murillo: Commercial Relationship: Code N (No
Commercial Relationship) | Afshan Nanji: Commercial Relationship: Code N (No Commercial Relationship) |
Marwan Atallah: Commercial Relationship: Code N (No Commercial Relationship) | Parke Green: Commercial
Relationship(s);Nidek Inc:Code E (Emplyment) | Mauro Campigotto: Commercial Relationship(s);Nidek
Technologies Srl, Padova, Italy:Code E (Emplyment) | Carol Karp: Commercial Relationship: Code N (No
Commercial Relationship)
81
Poster Board Number: P11
Role of Ultra High Resolution Optical Coherence Tomography (UHR-OCT) in the Diagnosis of Ocular
Surface Squamous Neoplasia (OSSN) in Complex Ocular Surface Diseases
Author(s): Marwan Atallah, Guillermo Amescua, Anat Galor, Juan Murillo, Madhura G. Joag, James R. Wong,
Nabeel M. Shalabi, Afshan A. Nanji, Carol L. Karp
Bascom Palmer Eye Institute
Purpose: Co-existence of OSSN with non-neoplastic ocular surface pathologies can mask the typical features of
OSSN on conventional examination. The Purpose of this study is to evaluate whether UHR-OCT could detect and
differentiate OSSN from co-existing ocular surface pathologies.
Methods: Eleven patients with known ocular surface diseases presenting with lesions suspicious for OSSN were
evaluated. UHR-OCT images of the lesions were taken at presentation. Biopsies were performed in all cases of
suspected OSSN by UHR-OCT. Follow up using UHR-OCT was done after appropriate treatment. The images were
compared to histological findings.
Results: Ten patients were found to have OSSN by UHR-OCT and confirmed by subsequent biopsy. Three patients
had OSSN within pterygia, 2 rosacea, 2 limbal stem cell deficiency, 1 Salzmann’ nodular degeneration, 1 vernal
keratoconjunctivitis, and 1 ocular cicatricial pemphigoid (Fig 1,2). In 1 case, OSSN was ruled out in the setting of
anterior scleritis in favor of pingueculum. In the 10 cases UHR-OCT images revealed epithelial layer thickening and
an abrupt transition in epithelium suggestive of OSSN. These findings were confirmed by pathology in all
cases. Follow up images detected resolution of the disease (8 cases) or recurrence (2 cases).
Conclusions: UHR-OCT can be used to non-invasively detect the presence of OSSN in patients with co-existing
complex ocular conditions.
(a) Severe rosacea with a thickened area at 5 o’clock. (b) UHR-OCT along the white line revealed a hyper
reflective thickened epithelium with an abrupt transition from normal to abnormal (arrow). (c) Pterygium with focus
of leukoplakia (arrow). (d) UHR-OCT along the white line showed thickened hyper reflective epithelium. (e)
Salzmanns nodular degeneration presenting with an area of opaque epithelium near the limbus at 4 o’clock. (f)
UHR-OCT along the white line showed Salzmann nodule (arrow) but also epithelial thickening. Biopsy confirmed
OSSN in all cases.
82
(a) Limbal stem cell deficiency (LSCD) with corneal scarring. (b) UHR-OCT done at 4 o’clock reveals epithelial
thickening with marked hyper reflectivity. (c) Patient with vernal keratoconjunctivitis and LSCD with corneal
scarring. (d) UHR-OCT reveals a thickened hyperreflective area.Biopsy confirmed OSSN in both cases.
Commercial Relationships Disclosure (Abstract): Marwan Atallah: Commercial Relationship: Code N (No
Commercial Relationship) | Guillermo Amescua: Commercial Relationship: Code N (No Commercial Relationship)
| Anat Galor: Commercial Relationship: Code N (No Commercial Relationship) | Juan Murillo: Commercial
Relationship: Code N (No Commercial Relationship) | Madhura Joag: Commercial Relationship: Code N (No
Commercial Relationship) | James Wong: Commercial Relationship: Code N (No Commercial Relationship) |
Nabeel Shalabi: Commercial Relationship: Code N (No Commercial Relationship) | Afshan Nanji: Commercial
Relationship: Code N (No Commercial Relationship) | Carol Karp: Commercial Relationship: Code N (No
Commercial Relationship)
83
Poster Board Number: P12
Noncontact direct observation of the human cornea by in vivo confocal microscopy with a high-power
objective lens
Author(s): Kaori Ideguchi, Eriko Abe, Taiichiro Chikama, Yuko Kadohiro, Takashi Sone, Ryotaro Toda, Sosuke
Inokawa, Yoshiaki Kiuchi
Hiroshima University
Purpose: In vivo confocal microscopy with a Heidelberg Retina Tomograph III–Rostock Cornea Module (HRTIIIRCM) allows noninvasive observation of corneal structures and cells layer by layer in high resolution by a contact
applanating procedure in which the cornea is separated from a TomoCap with gel. We evaluated noncontact direct
observation of the human cornea by in vivo confocal microscopy with a high-power objective lens.
Methods: A new adapter was developed for a high-power (×200) noncontact objective lens. Two normal volunteers
were recruited into the study and noncontact in vivo confocal microscopy was performed.
Results: Under the default condition for imaging, keratocytes and nerves in the corneal stroma as well as the
corneal endothelium were observed in both subjects. However, the superficial layer of the corneal epithelium
including the tear film was not observable because of high reflectivity. Adjustment of the imaging conditions
allowed observation of the superficial corneal epithelium and tear film with or without modification.
Conclusions: Noncontact in vivo confocal microscopy with a high-power (×200) objective lens allows the
observation of corneal cells and structures at higher magnification (×1.6) compared with contact in vivo confocal
microscopy. Further improvement of this procedure should allow the collection of high-quality images with easy
handling.
Commercial Relationships Disclosure (Abstract): Kaori Ideguchi: Commercial Relationship: Code N (No
Commercial Relationship) | Eriko Abe: Commercial Relationship: Code N (No Commercial Relationship) |
Taiichiro Chikama: Commercial Relationship: Code N (No Commercial Relationship) | Yuko Kadohiro:
Commercial Relationship: Code N (No Commercial Relationship) | Takashi Sone: Commercial Relationship: Code
N (No Commercial Relationship) | Ryotaro Toda: Commercial Relationship: Code N (No Commercial Relationship)
| Sosuke Inokawa: Commercial Relationship: Code N (No Commercial Relationship) | Yoshiaki Kiuchi:
Commercial Relationship: Code N (No Commercial Relationship)
84
Poster Board Number: P13
Analysis of the cornea densitometry using Pentacan with different illuminance
Author(s): Fernando Abib, Mariele A. Maximo, Andre Heck
Federal University of Parana
Purpose: To know the room lighting effect on corneal densitometry (CD) performed by Pentacan.
Methods: Thirty three normal patients from an Ophthalmological Clinic - Curitiba, Brazil. Age: 32±8 years. CD
performed with Pentacam high resolution software 1.20r10 (Oculus Optikgeräte GmbH, Germany). To measure the
illuminance (Il) of the examination room (ER), the digital LuxMeter 1.1 for I-phone (Application manufactory,
USA) was utilized. The CD was performed with two different room lighting: fluorescent lamp is on (27-30 lux) and
is off (0-1 lux) with GE compact fluorescent lamp Triple 15W 120-127V~60Hz 197mA 15W (Uberlandia, Brazil).
The CD was measured in the anterior corneal layer (120µm), posterior corneal layer (60 µm) and central layer at 0-2
mm, 2-6mm, 6-10mm, 10-12mm and total area. Step 1: The results of 33 CD are compared in only one eye per
patient, with the light on and off. Step 2: The results of 19 CD, with the light on and off in both eyes, are studied in
order to compare the range of the results between the eyes of the same patient. The results are reported by
descriptive statistics and the analysis will be performed with t Student, calculated by Microsoft Office Excel 2007
and GraphPad software.
Results: The figures report: 1.The results; 2.The analysis of the CD of the different annulus and layers performed in
room with light on and off ; 3.The range of the CD between the eyes of the same patient of the different annulus and
layers and their analysis.
Conclusions: The comparison of the CD of the 0-2 mm and 2-6mm annulus, for all corneal layers, were extremely
statistically significant with a different Il. The CD increases with the increase of the Il. There is no difference of
the CD range between the eyes of the same patient in the same Il of the 0-2 mm, 2-6 mm and 6-10 mm annulus, for
all corneal layers. The Il of the ER significantly altered the results of the corneal densitometry, thus increasing their
values. Whereas, Pentacan often must be repeated in the same patient, and its reproducibility is compromised if the
Il of the ER changes. It is suggested that Pentacan incorporates a luxmeter to establish a new reliability index for the
examination, so that their results of the examined cornea become more reproducible and representative. The required
minimum Il for the examination should be objectively defined by the manufacturer with this suggested luxmeter and
reliability index.
85
Commercial Relationships Disclosure (Abstract): Fernando Abib: Commercial Relationship: Code N (No
Commercial Relationship) | Mariele Maximo: Commercial Relationship: Code N (No Commercial Relationship) |
Andre Heck: Commercial Relationship: Code N (No Commercial Relationship)
86
Poster Board Number: P14
OptoVue OCT as an imaging modality of scleral thickness following fluocinolone acetonide implant
Author(s): Kristin Biggee1, 2, Nicholas Schubach1, Eric Suhler1, Christina J. Flaxel1
1
Casey Eye Institute, 2Devers Eye Institute
Purpose: To report the use of OptoVue OCT imaging of scleral thickness following fluocinolone acetonide (FA)
implant
Methods: Prospective case series. Repeat measurements of scleral thickness were performed using 3mm line scans
in multiple quadrants of the pars plana region in 3 patients with noninfectious posterior uveitis requiring FA
implant. Results were compared between implanted and fellow, non-implanted eyes or in the same eye before and
after implant insertion.
Results: Case 1 involved a 33yo woman with two previous FA implants in her right eye placed 8 years and then 3
years prior to imaging. Her overall mean scleral thickness in the right eye compared to her fellow, non implanted
eye was 455 (SD 148) vs 644.5μm (SD 11), P <0.005. A striking anatomical variance was noted in the inferonasal
(IN) and inferotemporal (IT) quadrant, which were the sites of her previous implants. Although anatomical
landmarks were less defined, estimates in the IN/IT quadrants showed a mean thickness of 269 (SD 53)/372μm
(SD52) in the implanted eye vs 645 (SD 4)/644μm (SD 16) in the fellow eye, P=0.006/0.07. Case 2 involved a 45yo
woman who received implants in the IN quadrant of both eyes placed 4 weeks apart. The mean scleral thickness in
the IN quadrant of the left eye increased from a baseline of 662 (SD 12) to 713μm (SD 3) at postoperative week one,
P<0.005. At postoperative week five, the right eye showed an insignificant change in overall mean scleral thickness
from a baseline of 614 (SD 35) to 606μm (SD 43). The IN quadrant showed the largest decrease from 641 (SD 22)
to 608μm (SD 22), P=0.18. Case 3 involved a 33yo female who received an implant in the IN quadrant of the left
eye. Scleral thickness was measured preoperatively and at postoperative week five and showed an overall mean
decrease from 663 (SD 31) to 629μm (SD 27) P=0.007. Each quadrant showed a similar decrease in thickness, with
a mean change of 35μm (SD 5).
Conclusions: OptoVue OCT may be a useful imaging modality to follow scleral thickness following FA
implant. It can be used to highlight potential dramatic scleral thinning as seen in the first select case in this
study. Longer follow up with a larger cohort of patients is needed to determine the utility and reproducibility of this
high resolution imaging following FA implant.
Case 1 IN quadrant implanted eye
87
Case 1 IN quadrant nonimplanted eye
Commercial Relationships Disclosure (Abstract): Kristin Biggee: Commercial Relationship: Code N (No
Commercial Relationship) | Nicholas Schubach: Commercial Relationship: Code N (No Commercial Relationship) |
Eric Suhler: Commercial Relationship: Code N (No Commercial Relationship) | Christina Flaxel: Commercial
Relationship: Code N (No Commercial Relationship)
88
Poster Board Number: P15
Posterior capsular opacification in intraocular hydrophilic lenses compared to hydrophobic intraocular
lenses using Scheimpflug images
Author(s): Arturo Olguin-Manriquez, Efrain Romo-Garcia, David Magana
hospital civil de culiacan
Purpose: To determine the visual outcomes and posterior capsule opacification (PCO) in acrylic intraocular lenses
(IOL).
Methods: Prospective analysis of 38 eyes of 19 patients who had uneventful phacoemulsification with implantation
of a IOL Akreos MI60 or a IOL Acrysof IQ from February 2013 to January 2014. Patients from a single single
surgeon, the protocol included the determination logMAR best corrected visual acuity (BCVA), spherical
equivalent, contrast sensitivity assessed by the Freiburg Visual Acuity test and PCO scoring using the Evaluation of
Posterior Capsular Opacification System (EPCO2000) by digital retroillumination photography and high resolution
tomograms from Scheimpflug reconstructions analyzed using ImageJ freeware.
Results: The mean follow up was 6.2 months ± 1.4(SD). Contrast Sentivity and BCVA were similar between the
lenses. Mean pixel intensity value using EPCO2000 software for Akreos MI60 was 1.08U and 1.08U for Acrysof IQ
(p=0.785). Using ImageJ mean value in pixels for Akreos MI60 was 1.76U and for Acysof IQ was 2.56U (p=0.027).
There were no significant correlationship between EPCO2000 and Pscheimpflug images (r=.141, p=.412).
Conclusions: This study found that the results of visual function were comparable between both lenses. The
posterior capsular opacification was seen to be lesser extent with the Akreos MI60 IOL when measured by
Scheimpflug images, probably due to the very design of the lens which showed no correlation compared to the
digital retroillumination photoghaphy.
89
Commercial Relationships Disclosure (Abstract): Arturo Olguin-Manriquez: Commercial Relationship: Code N
(No Commercial Relationship) | Efrain Romo-Garcia: Commercial Relationship: Code N (No Commercial
Relationship) | David Magana: Commercial Relationship: Code N (No Commercial Relationship)
90
Poster Board Number: P16
Morphologic Changes in Angle Closure Glaucoma After Iridotomies Documented By Ultrabiomicroscopy
Author(s): Efrain Romo-Garcia1, 2, Nicolas Corona-Osuna1, Silvia Lizarraga1, David Magaña1, arturo OlguinManriquez1, Miguel Piña1, Felipe Esquivel1, Arturo Ramirez-Mondragon1, Felipe Peraza-Garay1
1
CIDOCS / UAS, 2BuenaVista Foundation
Purpose: To describe changes in patients with angle closure glaucoma after performing Nd:YAG Laser
iridotomies documented by
ultrabiomicroscopy (UBM).
Methods: We include 20 eyes (10 patients) were a close angle was detected during gonioscopy. UBM was
performed before and 2 weeks after Nd:YAG Laser iridotomies. Follow up include full ophthalmological
examination.
Results: Anterior chamber central amplitude showed a significant increment (p=.26); peripheral anterior chamber
amplitude increment was documented but with no significant changes (p=.07). During follow up gonioscopy a
significant difference was detected (p=.000) after iridotomies with Nd:YAG laser.
Conclusions: Ultrabiomicroscopy is a useful study to mesure anterior chamber amplitude after treatment with
Nd:YAG Laser iridotomy and document changes in the iridocorneal angle.
Commercial Relationships Disclosure (Abstract): Efrain Romo-Garcia: Commercial Relationship: Code N (No
Commercial Relationship) | Nicolas Corona-Osuna: Commercial Relationship: Code N (No Commercial
Relationship) | Silvia Lizarraga: Commercial Relationship: Code N (No Commercial Relationship) | David Magaña:
Commercial Relationship: Code N (No Commercial Relationship) | arturo Olguin-Manriquez: Commercial
Relationship: Code N (No Commercial Relationship) | Miguel Piña: Commercial Relationship: Code N (No
Commercial Relationship) | Felipe Esquivel: Commercial Relationship: Code N (No Commercial Relationship) |
Arturo Ramirez-Mondragon: Commercial Relationship: Code N (No Commercial Relationship) | Felipe PerazaGaray: Commercial Relationship: Code N (No Commercial Relationship)
91
Poster Board Number: P17
Ocular Surface Health In Patients With Rheumatoid Arthritis In India
Author(s): Ramya Ravindran
SRMC AND RI
Purpose: The Purpose of this study was to evaluate the ocular surface of the eyes of patients suffering from
Rheumatoid Arthritis in India and look for potential problems that can affect these patients.
Methods: This is a prospective,non interventional observational study conducted at a multi specialty urban hospital.
forty patients suffering from Rheumatoid arthritis were included in this study. Patients with any other local or
systemic disease affecting the ocular surface were excluded as were patients with previous history of ophthalmic
surgery. These patients were assesed based on ocular surface staining and tear film break up time.Rose bengal was
used to stain the ocular surface and the van Bijsterveld staining score was used to estimate the surface viability.
Results: Out of the 80 eyes tested for TBUT 63 eyes was found to be lower than normal TBUT score ((78.75%). 48
eyes had a staining score of greater than 3(60%)Out of these 32 eyes had a score between 4-6 and 16 eyes had
severe OSD with a score of 7-9. . Out of these one patient had peripheral corneal melt and six patients presented
with SPK s. Out of the 40 patients 15 patients only presented with complaints discomfort, tearing, pain and burning
sensation. All others were asymptomatic.
Conclusions: This study was undertaken to show the importance of ocular surface health in Rheumatoid patients
as this disease is rather uncommon in our part of the world and the ocular surface is one of the most under-treated
parts of the eye due to a lack of awareness among patients and their primary care physicians. This study proves that
ocular surface dysfunction is a serious and morbid problem in patients who are suffering from Rheumatid arthritis.
Hence evaluation of the ocular surface, treatment of it's problems and management of the disease should all be
undertaken holistically.Missing these problems can lead to serious sight threatening complications like a corneal
melt as well as having implications in the quality of life for these patients.
Commercial Relationships Disclosure (Abstract): Ramya Ravindran: Commercial Relationship: Code N (No
Commercial Relationship)
92
201 Retinal Imaging
Poster Board Number: P18
Improving the processing and analysis workflow of adaptive optics retinal imaging
Author(s): Benjamin Sajdak1, Robert F. Cooper2, Kathleen Bazan3, Brian Higgins1, Drew Scoles4, Melissa Wilk5,
Alfredo Dubra1, 2, Joseph Carroll1, 2
1
Medical College of Wisconsin, 2Marquette University, 3Milwaukee School of Engineering, 4University of
Rochester, 5Medical College of Wisconsin
Purpose: While adaptive optics (AO) retinal imaging enables high-resolution, in vivo, visualization of retinal
pathology, the time required to process and analyze images is prohibitive for widespread adoption of this
technology. Here, we sought to expedite two of the more time-intensive aspects of the workflow: image montaging
and selecting regions of interest (ROIs) for subsequent density analyses.
Methods: Six subjects with normal vision and 3 subjects with albinism were imaged using an AO scanning light
ophthalmoscope (AOSLO). Sets of 18-26 partially overlapping images were aligned manually in Adobe Photoshop
(San Jose, CA) and also semi-automatically with i2k Retina (DualAlign LLC, Clifton Park, NY) montaging
software. We selected 100 x 100µm ROIs both manually and with custom software at 9-12 parafoveal locations.
Montaging and ROI selection methods were timed to evaluate efficiency of manual and semi-automated techniques.
For each ROI, cone density was measured to evaluate the accuracy of the semi-automated workflow.
Results: Using i2k Retina reduced montaging time by 7-53 minutes, or 25-79%. The semi-automated ROI selection
software reduced processing time by between 18-63 minutes, or 76-90%. Therefore, the semi-automated workflow
resulted in a combined reduction of 29-75 minutes, or 50-80%. Cone density measurements obtained from the semiautomated workflow were on average 2,563 cones/mm2 less than those obtained using the manual workflow (95%
CI = -9,465 to 4,339 cones/mm2, or 11 to 23%).
Conclusions: While the time-saving benefits of automated image processing methods are appealing, accuracy
appears to suffer. A current limitation of i2k Retina is that montages need to be assembled in piecemeal; further time
savings could be realized if no user oversight was required. The ROI selection software was used for comparison of
montaging techniques, and greatly improved the speed of the workflow process. The semi-automated workflow
greatly reduced the time required for analysis, however, the discrepancy in cone density measurements may be too
large to enable immediate adoption in its' current form. This study demonstrates the potential for an automated
workflow, and identifies important design improvements needed in future iterations of automated montaging
approaches.
Commercial Relationships Disclosure (Abstract): Benjamin Sajdak: Commercial Relationship: Code N (No
Commercial Relationship) | Robert Cooper: Commercial Relationship: Code N (No Commercial Relationship) |
Kathleen Bazan: Commercial Relationship: Code N (No Commercial Relationship) | Brian Higgins: Commercial
Relationship: Code N (No Commercial Relationship) | Drew Scoles: Commercial Relationship: Code N (No
Commercial Relationship) | Melissa Wilk: Commercial Relationship: Code N (No Commercial Relationship) |
Alfredo Dubra: Commercial Relationship: Code N (No Commercial Relationship) | Joseph Carroll: Commercial
Relationship: Code N (No Commercial Relationship)
93
Poster Board Number: P19
Clinical Assessment and Single Cell imaging in Unexplained Vision Loss
Author(s): Philip Severn4, Adam M Dubis4, Robert F. Cooper1, Joseph Carroll3, Alfredo Dubra2, Ganeshan K
Ramsamy5, Fred W Fitzke4, Gary Rubin4, Cathy Egan4, Michel Michaelides4
1
Marquette University , 2Medical College of Wisconsin Departments of Ophthalmology, 3Medical College of
Wisconsin , 4Moorfields Eye Hospital and University College London Institute of Ophthalmology, 5Barts and The
London School of Medicine
Purpose: Current clinical practice involves gross visual inspection and functional analysis to assess the causes of
visual impairments and deficit. While these tests can define most clinical diagnoses, some remain unresolved. Here
we applied cellular resolution imaging to examine retinal structure in a patient with an unexplained visual deficit.
Methods: Standard clinical assessment including dense Spectralis optical coherence tomography (OCT), extensive
electrophysiology (full field ERGs, multifocal ERGs, diffuse flash stimulation, EOG, high contrast pattern reversal,
photopic ON and OFF responses including S-cone ERG and colour contrast sensitivity analysis), psychophysics
(Nidek MP1 photopic microperimetry and photopic 30-2 Visual Field on a modified Humphrey) were applied to
assess visual symptoms. Blood tests were also used to assess potential autoimmune involvement. Cellular imaging
was completed using custom built adaptive optics scanning light ophthalmoscopes (AOSLO) at the Medical College
of Wisconsin and Moorfields Eye Hospital.
Results: Extensive clinical evaluation revealed no abnormalities to explain the patient’s visual symptoms. Single
test microperimetry showed normal or only subtle abnormalities that were inconsistent on retest. ERG results were
normal for all tests. AOSLO imaging showed small areas reminiscent of small sub-clinical drusen (1). Examples of
these structures are shown in Figure A&B.
Conclusions: While a few abnormalities were shown with AOSLO, they did not completely explain the visual
complaints. However, these structures were more reproducible and conclusive than standard clinical measures.
Figure A & B: Adaptive Optics Scanning Light Ophthalmoscope images taken from 3º (A) and 5º (B) temporal to
fixation. The arrows delineate regions of abnormal cone patterning, which may be the result of visual complaints.
Scale bar is 50 µm.
94
1.Godara, P., Siebe, C., Rha, J., Michaelides, M., Carroll, J. “Assessing the photoreceptor mosaic over drusen using
adaptive optics and spectral-domain optical coherence tomography” Ophthalmic Surgery, Lasers, & Imaging, 41(6):
S104-S108 (2010).
Commercial Relationships Disclosure (Abstract): Philip Severn: Commercial Relationship: Code N (No
Commercial Relationship) | Adam M Dubis: Commercial Relationship(s);Patent 8,226,236, (C) Canon USA
Inc:Code P (Patent) Robert Cooper: Commercial Relationship: Code N (No Commercial Relationship) | Joseph
Carroll: Commercial Relationship: Code N (No Commercial Relationship) | Alfredo Dubra: Commercial
Relationship: Code N (No Commercial Relationship) | Ganeshan K Ramsamy: Commercial Relationship: Code N
(No Commercial Relationship)| Fred W Fitzke: Commercial Relationship: Code N (No Commercial Relationship) |
Gary Rubin: Commercial Relationship: Code N (No Commercial Relationship) | Cathy Egan: Commercial
Relationship: Code N (No Commercial Relationship) | Michel Michaelides: Commercial Relationship: Code N (No
Commercial Relationship)
95
Poster Board Number: 20
High-resolution En face images of microcystic macular edema in patients with autosomal dominant optic
atrophy
Author(s): Shuhei Kameya1, Kiyoko Gocho1, Sachiko Kikuchi1, Kei Shinoda2, Atsushi Mizota2, Kunihiko Yamaki1,
Hiroshi Takahashi3
1
Chiba Hokusoh Hosp Nippon Med Sch, 2Teikyo University School of medicine, 3Nippon Medical School
Purpose: To investigate the characteristics of microcystic macular edema (MME) determined from the en face
images obtained by an adaptive optics (AO) fundus camera in patients with autosomal dominant optic atrophy
(ADOA) and to try to determine the mechanisms underlying the degeneration of the inner retinal cells and RNFL by
using the advantage of AO.
Methods: Six patients from 4 families with ADOA underwent detailed ophthalmic examinations. Ophthalmic
examinations including spectral domain optical coherence tomography (SD-OCT) were performed. Mutational
screening of all coding and flanking intron sequences of the OPA1 gene was performed by DNA sequencing. Highresolution en face images of the fundus were obtained with a flood-illuminated AO fundus camera.
Results: All 6 patients had reduced visual acuity and palor of the temporal disc. SD-OCT showed a severe
reduction in the retinal nerve fiber layer thickness. A new splicing-defect and two new frameshift mutations with
premature termination of the Opa1 protein were identified in three families. A reported nonsense mutation was
identified in one family. SD-OCT of one patient showed MME in the inner nuclear layer of the retina. AO images
showed microcysts in the en face images of the inner retinal layer. Another patient also had similar microcystic
structures in the AO images despite their absence in the SD-OCT images.
Conclusions: Our findings implicate the possibility that MME is the results of retrograde trans-synaptic
degeneration of cells in the inner nuclear layer of the retina. Our data indicate that AO is a useful method to identify
MME in neurodegenerative diseases and may also help determine the mechanisms underlying the degeneration of
the inner retinal cells and retinal nerve fiber layer.
Commercial Relationships Disclosure (Abstract): Shuhei Kameya: Commercial Relationship: Code N (No
Commercial Relationship) | Kiyoko Gocho: Commercial Relationship: Code N (No Commercial Relationship) |
Sachiko Kikuchi: Commercial Relationship: Code N (No Commercial Relationship) | Kei Shinoda: Commercial
Relationship: Code N (No Commercial Relationship) | Atsushi Mizota: Commercial Relationship: Code N (No
Commercial Relationship) | Kunihiko Yamaki: Commercial Relationship: Code N (No Commercial Relationship) |
Hiroshi Takahashi: Commercial Relationship: Code N (No Commercial Relationship)
96
Poster Board Number: P21
Magnetic resonance imaging findings of the subretinal space in bilateral congenital retinal detachments in
Norrie’s syndrome
Author(s): Rocio I. Diaz2, 4, Eric J. Sigler2, 4, Asim F. Choudhri1, 3, Jorge I. Calzada2, 4
1
LeBonheur Children's Hospital, 2Charles Retina Institute, 3University of Tennessee Health Science Center,
4
University of Tennessee Health Science Center
Purpose: To characterize the magnetic resonance imaging findings in the subretinal space in patients with bilateral
congenital retinal detachment (RD)
Methods: Retrospective case-series of infants with an abnormal red-reflex who were further studied with orbital
MRI, using T1, T2-weighted and FLAIR modalities. All patients underwent examination under anesthesia, visual
evoked potentials, electroretinograms and pars plana vitrectomy
Results: Three male infants were included in the study. The MRI of orbits consistently demonstrated bilateral RD
with a gravity-dependent fluid level in the subretinal space. These bilateral subretinal effusions demonstrated T1
shortening and T2 prolongation, likely due to layering of blood products (hemosiderin, methemoglobin, and
proteinaceous contents). All infants presented bilateral optic nerve hypoplasia and microphthalmia. Genetic testing
of one of the infants’ DNA revealed a deletion of exon 1 in the ND gene. All patients underwent examination under
anesthesia and the diagnosis of tractional RD was confirmed in all cases. Visual evoked potentials were recordable
in some eyes, while electroretinograms were unrecordable in all cases. Pars plana vitrectomy and lensectomy was
performed in the eye with the best visual potential
Conclusions: Congenital RD associated to Norrie’s syndrome can present a typical fluid level in the subretinal
space on MRI. This can help differentiate this syndrome from other causes of infantile RD, like persistent fetal
vasculature, Coats’ disease and retinoblastoma
Image 1. MRI findings in a 5-month-old male with bilateral RD. A. Axial T1 FLAIR demonstrating bilateral RD,
bilateral microphthalmia, and a hypointense collection on the subretinal space of the left eye (arrow). B. Axial T2weighted orbital MRI of the same infant reveals a distinct hypointense deposit, corresponding to layering of blood
products (arrow)
97
Image 2. MRI fluid level characteristics in infants with congenital bilateral RD. A. Axial T1-weighted orbital MRI
of a one-week-old male revealing total bilateral RD, and a discrete hypointensity on the posterior pole, compatible
with a fluid level in the subretinal space. B. T2-weighted MRI of a 8-month- old male demonstrating an area of
hypointensity corresponding to bilateral subretinal effusions. The gravity-dependent level, compatible with layering
of blood products, is more visible on the left eye
Commercial Relationships Disclosure (Abstract): Rocio Diaz: Commercial Relationship: Code N (No
Commercial Relationship) | Eric Sigler: Commercial Relationship: Code N (No Commercial Relationship) | Asim
Choudhri: Commercial Relationship: Code N (No Commercial Relationship) | Jorge Calzada: Commercial
Relationship: Code N (No Commercial Relationship)
98
Poster Board Number: P22
Fluorescence Lifetime Measurement in Central Artery Occlusion
Author(s): Chantal Dysli, Sebastian Wolf, Martin S. Zinkernagel
Ophthalmology
Purpose: Fluorescence Lifetime Imaging Ophthalmoscopy (FLIO) is used more recently for non invasive in vivo
measurement of lifetimes of natural retinal fluorophores upon laser excitation. Fluorescence lifetimes are dependent
of the metabolic environment such as the oxygenation level and the pH concentration. Therefore we aim to
characterize fluorescence lifetimes of the retina after central artery occlusion.
Methods: A Spectralis® FLIO system (Fluorescence Lifetime Imaging Ophthalmoscope; Heidelberg Engineering,
Germany) was used for fluorescence lifetime measurement of the ocular fundus. Fluorescence was excited using a
picosecond laser at 473 nm wavelength. Decay times were measured in a short (498–560 nm) and in a long (560–
720 nm) spectral channel. FLIO was performed in eyes after central retinal artery occlusion (CRAO) and compared
to the contra lateral healthy eyes. Mean lifetimes were averaged within ETDRS grid areas (center, inner ring, outer
ring).
Results: In the short spectral channel, mean fluorescence lifetime values in the central area of the ETDRS grid were
296 ± 65 picoseconds (ps) (mean ± standard error of the mean) in eyes after CRAO and 231 ± 26 ps in the healthy
control eyes (p=0.01). In the inner ETDRS ring, mean lifetimes were 455 ± 61 ps after CRAO and 323 ± 23 ps in
control eyes (p=0.0006). In the long spectral channel, mean lifetimes in the central area were 357 ± 27 ps after
CRAO and 341 ± 21ps in the control eyes (p=0.0006). In the inner ETDRS ring, mean lifetimes were 429 ± 26 ps
after CRAO and 379 ± 22 ps in control eyes (p=0.0001).
Conclusions: Central retinal artery occlusion led to disease associated changes in fluorescence lifetimes of retinal
fluorophores. Significantly longer lifetimes were observed in all ETDRS areas, potentially caused by altered cellular
metabolism after retinal ischemia. In future, fluorescence lifetime measurement might be used for diagnostic
Purpose , disease and therapy monitoring, and might even have prognostic value.
Commercial Relationships Disclosure (Abstract): Chantal Dysli: Commercial Relationship(s);Heidelberg
Engineering:Code F (Financial Support) | Sebastian Wolf: Commercial Relationship(s);Heidelberg
Engineering:Code F (Financial Support);Heidelberg Engineering:Code C (Consultant) | Martin Zinkernagel:
Commercial Relationship(s);Heidelberg Engineering:Code F (Financial Support)
99
Poster Board Number: P23
Brownian Motion Imaging With Optical Coherence Tomography and Optical Coherence Tomography
Angiography
Author(s): Gangjun Liu, Yan Li, Yali Jia, David Huang
Oregon Health & Science University
Purpose: Investigate the possibility of imaging and quantifying the Brownian motion of particles and red blood
cells with Optical Coherence Tomography and Optical Coherence Tomography Angiography. Here, we use splitspectrum amplitude decorrelation angiography (SSADA) method for the angiography analysis.
Methods: A custom-built OCT system with a central wavelength of 1050 nm and a speed of 100 thousand A-lines
per second is used in this study. Suspensions of microspheres of different diameters (800nm, 3um, 5um and 10um)
and different concentration in Borate Buffered Saline (BBS) solution are studied. The suspensions of fresh porcine
red blood cells (RBCs) in porcine plasma stabilized with sodium citrate are also investigated. Continuous time
sequence B-scan OCT images are obtained from these sample and then processed SSADA.
Results: The OCT system can detect single particle in the suspensions when the microsphere concentration is low.
OCT signal slope (signal attenuation with depth) changes with the microsphere concentration. Time sequence Bscan OCT images enable us to see fast movement of the microsphere in the suspensions. The microsphere Brownian
motion is able to be detected with the SSADA. Imaging of the Brownian motion of RBC in plasma is demonstrated.
Conclusions: Optical Coherence Tomography enables us see single small particle and split-spectrum amplitude
decorrelation OCT angiography is able to image Brownian motion of RBC in plasma.
The OCT structure (1a-1d) and split-spectrum amplitude decorrelation OCT angiography (1e-1h)images of 3um
particle suspension with concentration of 0.17% (1a,1e), 0.042% (1b, 1f), 0.005% (1c, 1g) and 0.001% (1d, 1h).
100
The OCT structure (2a-2d) and split-spectrum amplitude decorrelation OCT angiography (2e-2h) images of RBC in
plasma suspension with RBC vs plasma ratio of 1:1 (2a, 2e), 1:10 (2b, 2f), 1:100 (2c, 2g) and 1:1000 (2d, 2h).
Commercial Relationships Disclosure (Abstract): Gangjun Liu: Commercial Relationship: Code N (No
Commercial Relationship) | Yan Li: Commercial Relationship(s);Optouve, Inc. :Code F (Financial Support);Carl
Zeiss Meditec, Inc.:Code P (Patent);Optouve, Inc. :Code P (Patent) | Yali Jia: Commercial Relationship(s);Optouve,
Inc. :Code P (Patent)| David Huang: Commercial Relationship(s);Optouve, Inc. :Code F (Financial
Support);Optouve, Inc. :Code P(Patent);Optouve, Inc. :Code I (Personal Financial Interest); Carl Zeiss
Meditec:Code P (Patent)
101
Poster Board Number: P24
Histogram Matching Extends Acceptable Signal Strength (SS) Range on Optical Coherence Tomography
(OCT) Images
Author(s): Chieh-Li Chen1, 2, Hiroshi Ishikawa1, 2, Gadi Wollstein1, Richard A. Bilonick1, 3, Ian A. Sigal1, 2, Larry
Kagemann1, 2, Joel S. Schuman1, 2
1
UPMC Eye Center, Eye and Ear Institute, Ophthalmology and Visual Science Research Center, Department of
Ophthalmology, University of Pittsburgh School of Medicine, 2Department of Bioengineering, Swanson School of
Engineering, University of Pittsburgh, 3Department of Biostatistics, Graduate School of Public Health, University of
Pittsburgh
Purpose: SS strongly correlates with OCT thickness measurements. This relationship limits the range of acceptable
SS, which also limits the applicability of OCT measurements to older/diseased subjects because they tend to have
lower best-achievable SS than young/healthy subjects. The Purpose of this study was to minimize the influence of
SS variability on OCT measurements using histogram matching (HM).
Methods: Seven eyes from seven healthy subjects were scanned with Cirrus HD-OCT (Zeiss, Dublin, CA; Optic
Disc Cube 200x200 scan). A series of OCT images with a wide range of SS (maximal range 1 to 10) was acquired
from each eye at the same visit. For each cube scan, one circumpapillary B-scan image was resampled along the
3.45-diameter circle centered to the optic nerve head. For each series, the histogram of a resampled image with the
highest SS was set as the reference. HM was applied to the other images with lower SS. The process of HM involves
minimizing the difference in intensity at each percentile of the histogram between the reference and the target
image. The circumpapillary retinal nerve fiber layer thickness (RNFLT) was automatically measured using
segmentation software of our own design (HM measurement), which was then compared to the device output
(Device measurement). Non-linear mixed effects models were constructed to analyze the relationship between
RNFLT and SS across various SS range. In addition, the coefficient of variation (CoV) of the Device measurements
within the manufacturer recommended acceptable SS range (SS 6 to 10) was calculated on each case. The lowest SS
that achieved similar Device CoV on HM measurements was detected on each case.
Results: Two segments of linear relationships were detected on both Device and HM measurements (Figure). The
second segment, which represents the linear relationship in the higher half of the SS range, of the HM measurements
had flatter slope (less variable) than the Device measurements (0.6 vs. 1.6 μm), while the breaking point was higher
with the HM than the Device measurements (4.1 vs. 3.1). The mean Device CoV was 0.025, while HM
measurements showed similar CoV with wider SS range (0.022, SS 4 to 10).
Conclusions: HM successfully extends the acceptable SS range on OCT images. This broadens the OCT
measurement application to subjects whose images are excluded from the quantitative analysis with the conventional
method.
102
Commercial Relationships Disclosure (Abstract): Chieh-Li Chen: Commercial Relationship: Code N (No
Commercial Relationship) | Hiroshi Ishikawa: Commercial Relationship: Code N (No Commercial Relationship) |
Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) | Richard Bilonick: Commercial
Relationship: Code N (No Commercial Relationship) | Ian Sigal: Commercial Relationship: Code N (No
Commercial Relationship) | Larry Kagemann: Commercial Relationship: Code N (No Commercial Relationship) |
Joel Schuman: CommercialRelationship(s);Zeiss:Code P (Patent)
103
Poster Board Number: P25
Effect of Scanning Incident Angle (IA) on Total Retinal Thickness (TRT) Measurement With A Phantom Eye
Using Spectral-Domain Optical Coherence Tomography (SD-OCT)
Author(s): Hiroshi Ishikawa1, 2, Chieh-Li Chen1, 2, Jigesh Baxi3, Anant Agrawal3, Daniel X. Hammer3, Gadi
Wollstein1, Richard A. Bilonick1, 4, Ian A. Sigal1, 2, Larry Kagemann1, 2, Joel S. Schuman1, 2
1
Department of Ophthalmology, University of Pittsburgh School of Medicine, 2University of Pittsburgh, 3Food and
Drug Administration, 4University of Pittsburgh
Purpose: To investigate the effect of scanning IA on SD-OCT TRT measurement using a phantom eye.
Methods: A water-filled phantom eye, mimicking a healthy human retina and optic nerve head with dilated 7 mm
pupil, was scanned using a commercially-available clinical OCT instrument (raster volume scan centered at the optic
nerve head). The scanning beam was positioned through the center of the pupil, and the retinal image appeared flat
on the screen, which was considered to be 0 degree reference angle. To generate different IAs between the scanning
beam and the retinal surface, the phantom eye was rotated temporally (defined as positive direction) and nasally
(negative direction) up to 12 degrees with 3-degree increments. Five scans were obtained at each IA. The quality
index (QI) and TRT (the thickness between the inner and outer borders of the simulated retina, Figure A) were
measured automatically on each scan using a software program of our own design. The mean QI and the mean TRT
of five scans at each IA were calculated. In order to compensate the interaction between signal strength and TRT, an
additional series of scans at the 0-degree position with various signal strengths were obtained to model the
relationship between TRT and QI.
Results: TRT showed significant correlation with QI (R2=0.83, p=0.004, Figure B). The QI decreased as IA
increased in both directions (showing a Λ-shape against IA, Figure C), while the quality compensated TRT
increased along with the IA (showing a V-shape against IA, Figure D).
Conclusions: Different IAs may add considerable measurement variability for device calibration. However, the
variation in TRT measurements due to different IAs was within expected measurement variability, and thus not
clinically significant.
Figure. A) Cross-sectional image of the phantom eye, the total retinal thickness (TRT) is defined as the distance
between the inner and outer borders of the simulated retina; B) Linear correlation between quality index (QI) and
TRT; C) and D) Effects of incident angle (IA) on QI and TRT.
104
Commercial Relationships Disclosure (Abstract): Hiroshi Ishikawa: Commercial Relationship: Code N (No
Commercial Relationship) | Chieh-Li Chen: Commercial Relationship: Code N (No Commercial Relationship) |
Jigesh Baxi: Commercial Relationship: Code N (No Commercial Relationship) | Anant Agrawal: Commercial
Relationship: Code N (No Commercial Relationship) | Daniel X. Hammer: Commercial Relationship: Code N (No
Commercial Relationship) | Gadi Wollstein: Commercial Relationship: Code N (No Commercial Relationship) |
Richard Bilonick: Commercial Relationship: Code N (No Commercial Relationship) | Ian Sigal: Commercial
Relationship: Code N (No Commercial Relationship) | Larry Kagemann: Commercial Relationship: Code N (No
Commercial Relationship) | Joel Schuman: Commercial Relationship(s);Zeiss:Code P (Patent);Zeiss:Code C
(Consultant)
105
Poster Board Number: P26
Modeling the topography of the healthy human retina
Author(s): Rui Bernardes1, 2, Silvia Simão3, Ana S. C.Silva2, Angelina Meireles4, João Figueira3,5
1
AIBILI - Association for Innovation and Biomedical Research on Light and Image, 2IBILI- Institute for Biomedical
Imaging and Life Sciences, 3AIBILI - Association for Innovation and Biomedical Research on Light and Image,
4
Porto Hospital Center, 5Coimbra University Hospital
Purpose: To model the topography of the healthy human retina and derive fitting parameters aiming to monitor
changes due to retinal traction.
Methods: Optical coherence tomograms of a population of 23 healthy controls aged from 46 to 79 yrs (avg/sd:
58.2/10.1 yrs) were acquired by the SD-OCT (Cirrus OCT, Carl Zeiss Meditec, Dublin, CA, USA), in a total of 43
eyes (22 left and 21 right eyes). Retinal thickness maps from these scans were co-registered to the RT-Atlas
previously developed by our research group (OCT Thickness Mapping of the Human Macula, IOVS, May 2008, Vol.
49, No. 5, pp 2046-2052 ) aiming to correct the location and orientation of all scans to a common reference. In this
reference, the center of the map (0,0) corresponds to the location of the fovea and the horizontal axis connects the
center of the fovea to the center of the optic disc (positive increasing values towards the nasal side and negative
values towards the temporal side). Each retinal thickness map was interpolated to a common grid and the data
distribution analyzed at each grid point. Extreme values were removed at each grid point and the average retinal
thickness was computed. A set of well-known functions were tested to mimic the topography of the resulting
surface. Among others, combination of Gaussian and Cauchy distribution curves and a modified second-order
quadratic surface were tested and the root mean-square error computed as the measure of the goodness of the fit.
Results: A combination of 4 functions, in a total of 23 parameters, were determined allowing to mimic the average
topography of the healthy human retina. The distribution of individual parameters, resulting from the fit of the
mathematical model to each retina, presents an approximately normal distribution with an average kurtosis of -1.38
and an average skewness of 0.13.
Conclusions: A mathematical model of the healthy human retina topography was determined based on a set of 4
functions in a total of 23 parameters. These parameters can be used to compare individual retina's topography to the
healthy distribution for classification Purposes.
Commercial Relationships Disclosure (Abstract): Rui Bernardes: Commercial Relationship: Code N (No
Commercial Relationship) | Silvia Simão: Commercial Relationship: Code N (No Commercial Relationship) | Ana
S. C.Silva: Commercial Relationship: Code N (No Commercial Relationship) | Angelina Meireles: Commercial
Relationship: Code N (No Commercial Relationship) | João Figueira: Commercial Relationship: Code N (No
Commercial Relationship)
106
Poster Board Number: P27
Preliminary evaluation of a prototype metabolic hyperspectral retinal camera in age related macular
degeneration patients
Author(s): Jean-Philippe Sylvestre1, Rachel Trussart2, Jean Daniel Arbour2
1
Optina Diagnostics, 2Université de Montréal
Purpose: The aim of this preliminary study is to compare a novel hyperspectral retinal imaging modality, using a
prototype metabolic hyperspectral retinal camera (MHRC), with conventional color fundus and optical coherence
tomography (OCT) imaging in patients with wet-ARMD to establish early correlations between the spectral
information and the known anatomical landmarks of the disease.
Methods: Fourteen volunteers with diagnosed wet ARMD (10 females, average age 75 ± 7 yrs, no intra-ocular
lens) had retinal images captured between 470-850 nm using a prototype MHRC (Optina Diagnostics, Montreal,
Canada). The MHRC is based on a tunable laser source that permits the selection of a specific wavelength from a
supercontinuum source with a spectral bandwidth of 2 nm (FWHM) and a precision < 1 nm. Typical acquisitions
were obtained at a rate of 2-3 wavelengths per second. For comparison Purposes, a color fundus image and an
optical coherence tomography (OCT) scan were also obtained using a 3D OCT-1000 (Topcon, Tokyo, Japan).
Results: High definition retinal imaging at multiple wavelengths was obtained for all subjects. Spectral information
could therefore be extracted from the datasets when sufficient quality images obtained at different wavelengths were
available and registered satisfactorily. Pathological changes such as hyperplasia and atrophy of the retinal pigment
epithelium (RPE) are enhanced when the retina is illuminated with red of near-infrared (NIR) light compared to
color fundus images. Similarly, anatomical changes visible with OCT such as intraretinal and sub-RPE fluid,
undetected with color fundus, were successfully highlighted at specific wavelengths with the MHRC. Drusen and
lipid exudates are characterized by hypereflectance under visible and NIR illumination.
Conclusions: The MHRC based on a tunable laser filter can provide anatomical and spectral information from the
retina which could help in the automatic recognition of landmarks related to wet ARMD and ultimately contribute to
the early detection and optimal management of the disease. Improvements to the prototype MHRC and analysis
software are currently underway to significantly increase the acquisition speed (up to 27 wavelengths per second)
and registration precision to permit extraction of spectral-rich information from all collected datasets.
Commercial Relationships Disclosure (Abstract): Jean-Philippe Sylvestre: Commercial Relationship(s);Optina
Diagnostics:Code E (Emplyment);Optina Diagnostics:Code I (Personal Financial Interest) | Rachel Trussart:
Commercial Relationship: Code N (No Commercial Relationship) | Jean Daniel Arbour: Commercial
Relationship(s);Optina Diagnostics:Code I (Personal Financial Interest)
107
Poster Board Number: P28
Quantitative autofluorescence (qAF) in pseudophakic normal and dry Age-related macular degeneration
(AMD) patients
Author(s): Camellia Nabati1, Jonathan Greenberg2, Dan Yoon1, Elana Rosenberg1, David Sackel1, Roland Smith1
1
Department of Ophthalmology New York University School of Medicine, 2Columbia University
Purpose: Lipofuscin accumulates normally in the retinal pigment epithelium (RPE) with age, but its role in AMD is
debated. We measured lipofuscin accumulation with qAF in vivo in elderly normal and AMD patients to shed light
on this question.
Methods: qAF was calibrated to the internal fluorescent reference in the Heidelberg Spectralis as previously
described [Delori et al, Quantitative measurements of AF with the SLO. IOVS. 2011:9379-90.]. All patients were
pseudophakic with clear posterior capsules and were dilated to >6.5mm. The transmission spectrum of the
intraocular lens (IOL) was then used to calculate an integrated two-pass excitation and emission transmission
relative to that of a 20 year-old phakic eye. qAF correction factors were typically 0.955 for blue light filtering IOLs
and 0.825 for clear IOLs.
Results: Mean (+/- SD) qAF units in 6 zones superotemporally in 22 eyes of 22 pseudophakic patients, ages 61 to
89, 1 late, 7 early AMD, 14 normal was 341 +/- 137 in normals and 277 +/- 32 (P = 0.10) in 8 AMD subjects of
similar ages (Figure: normal, early, late). Interestingly, three zone qAF close to geographic atrophy (GA), (mean,
243) in an early GA patient, (arrow,E), was similar to three zone qAF close to GA (mean, 261) in the patient with
established GA (arrow, F).
Conclusions: In this small sample, a trend towards lower qAF in dry AMD subjects than in normals was observed,
with a wide variability in both groups. A large study, with all pertinent environmental and genetic risk factors, is
clearly warranted.
Top row, original AF images, acquired with reference in place superiorly; bottom row, calibrated qAF images. A, 67
y/o F, normal; B, 86 y/o F with reticular pseudodrusen (RPD) and early signs of geographic atrophy (GA); C, 76 y/o
F with established multilobular GA and RPD. Note that although the original AF image in C is brighter, when it is
calibrated to the reference, also brighter, to give the qAF image, F, the qAF levels are now lower than the other two,
D, E. The mean qAF in the 6 outer superior and temporal analysis zones are: 411, 357, and 269, respectively. The
normal patient, although youngest, has the highest qAF; the oldest patient, with early GA and RPD is less, and the
patient with established GA, the lowest qAF. Note that qAF in zones near GA in two subjects are similar (arrows,
E, F).
Commercial Relationships Disclosure (Abstract): Camellia Nabati: Commercial Relationship: Code N (No
Commercial Relationship) | Jonathan Greenberg: Commercial Relationship: Code N (No Commercial Relationship)
| Dan Yoon: Commercial Relationship: Code N (No Commercial Relationship) | Elana Rosenberg: Commercial
108
Relationship: Code N (No Commercial Relationship) | David Sackel: Commercial Relationship: Code N (No
Commercial Relationship) | Roland Smith: Commercial Relationship: Code N (No Commercial Relationship)
109
Poster Board Number: P29
Comparison of Fundus Autofluorescence Imaging by 488 nm and 532 nm Confocal Scanning Laser
Ophthalmoscopy in Central Serous Chorioretinopathy
Author(s):Seong-Woo Kim2, Jaeryung Oh3, Cheol Min Yun1, Kuhl Huh1
1
Korea University, Guro Hospital, 2Korea Univeristy, Ansan Hopsital, 3Korea University, Medical center
Purpose: To compare lesion characteristics between blue-light (488 nm) and green-light (532 nm) confocal
scanning laser ophthalmoscopy (cSLO) autofluorescence (AF) of central serous chorioretinopathy (CSC).
Methods: The lesion characteristics were compared between 488 nm and 532 nm cSLO fundus autofluorescence
(FAF) images in acute CSC. The mean disease duration and subretinal fluid (SRF) height in the spectral domain
optical coherence tomography were compared according to the FAF image characteristics.
Results: The study included 63 eyes of 61 patients; 63 pairs of FAF images were compared before CSC resolution
and 31 pairs of FAF images were compared after CSC resolution. Before CSC resolution, 48 (76.2%) images of
acute CSC were hypo-AF to no change, 3 (4.8%) were hyper-AF, and 12 (19.0%) were mixed-AF in 488 nm FAF
images whereas 9 (14.3%) images were hypo-AF to no change, 44 (69.8%) were hyper-AF, and 10 (15.9%) were
mixed-AF in 532 nm FAF images (p<0.0001). There was no significant difference in the lesion composite pattern
between the two FAF image wavelengths. Patients with lesions that were hyper-AF in 532 nm AF and hypo-AF in
488 nm AF had a shorter disease duration and greater SRF height than those who were hyper-AF in both 532 nm
and 488 nm images.
Conclusions: The two types of FAF image showed similar lesion characteristics in CSC. However, 532 nm AF
imaging showed increased background AF in detached retina, whereas 488 nm AF imaging showed decreased
background AF in acute CSC.
110
Commercial Relationships Disclosure (Abstract): Seong-Woo Kim: Commercial Relationship: Code N (No
Commercial Relationship) | Jaeryung Oh: Commercial Relationship: Code N (No Commercial Relationship) | Cheol
Min Yun: Commercial Relationship: Code N (No Commercial Relationship) | Kuhl Huh: Commercial Relationship:
Code N (No Commercial Relationship)
111
Poster Board Number: P30
Cone photopigment distribution measured using green autofluorescence imaging
Author(s): Kanako Itagaki, Kimihiro Imaizumi, Akira Ojima, Tetsuju Sekiryu
fukusima medical univeicity
Purpose: To evaluate the feasibility of using green autofluorescence imaging to measure cone photoreceptor's
pigment distribution in normal subjects and patients with central serous chorioretinopathy (CSC).
Methods: Twelve normal eyes of 12 subjects and 9 eyes with CSC were studied using autofluorescence imaging
obtained using a confocal scanning laser ophthalmoscope (F-10, Nidek, Gamagori, Japan). Green autoflurescence
was used (excitation :532 nm , Emi. > 555 nm), the angular field was 40°, and images were acquired at 6/images per
second (corneal irradiance: 110 microW). Autofluorescence images for the light adapted state were obtained after 20
minutes of light adaptation in the room light. 60 images were taken continuously during 10 second. The
photopigment topographical distribution was calculated from the difference of logarithms the averaged 5 images at
the beginning and the end of image acquisition. The square area (300x300 pixels) centered at the fovea on the
fundus image was evaluated. The photopigment density was normalized by the value at the adjucent healthy area in
the eyes with CSC to compare the changes of the photopigment distribution during the course of the disease.
Results: The distribution of the photopigment showed a concentric pattern in all of normal eyes. The mean density
at the center of the fovea (0.23 log unit) was highest in the square. The mean photopigment density decreased
gradually toward the edge of the area. The photopigment density at the center of the fovea in the eyes with serous
retinal detachment was ranged -0.02 to 0.2 log unit. That incresed in 5 of 9 eyes (55%) after reattachment, whereas
that decrease in the remaining 4 eyes (45%).
Conclusions: The distribution of the photopigment showed a concentric pattern in all of normal eyes. The mean
density at the center of the fovea (0.23 log unit) was highest in the square. The mean photopigment density
decreased gradually toward the edge of the area. The photopigment density at the center of the fovea in the eyes with
serous retinal detachment was ranged -0.02 to 0.2 log unit. That incresed in 5 of 9 eyes (55%) after reattachment,
whereas that decrease in the remaining 4 eyes (45%).
Commercial Relationships Disclosure (Abstract): Kanako Itagaki: Commercial Relationship: Code N (No
Commercial Relationship) | Kimihiro Imaizumi: Commercial Relationship: Code N (No Commercial Relationship) |
Akira Ojima: Commercial Relationship: Code N (No Commercial Relationship) | Tetsuju Sekiryu: Commercial
Relationship: Code N (No Commercial Relationship)
112
Poster Board Number: P31
Fundus Autofluorescence to Identify Plaques and Diagnose and Follow Retinal Artery Occlusions
Author(s): Yannis M. Paulus, Aazim Siddiqui, Adrienne W. Scott
Wilmer Eye Institute, Johns Hopkins University
Purpose: Retinal artery occlusions can require invasive testing with fluorescein angiography for diagnosis. The
associated etiologic plaques are often difficult to identify. We examine the role of fundus autofluorescence (FAF) as
a noninvasive imaging modality to identify plaques, diagnose, and follow-up of patients with retinal artery
occlusions.
Methods: A series of four patients who presented to a single tertiary care referral center were diagnosed with
retinal artery occlusions. Fundus autofluorescence was performed along with conventional imaging and FAF
characteristics were evaluated over time.
Results: In all three patients who presented acutely, fundus autofluorescence demonstrated a sharply-demarcated
region of hypoautofluorescence in the distribution of nonperfused retina in branch retinal artery occlusions that
occured on initiation of symptoms. This region of hypoautofluorescence normalized and disappeared by 1 to 1.5
months after onset in all patients with long-term follow-up. In two patients without discernable plaques on
examination or fundus photography, fundus autofluorescence showed a very bright hyperautofluorescent plaque that
persists for at least a couple months and likely indefinitely for the duration of the plaque (Figures 1 and 2). The third
patient had a visible plaque on physical exam that was not hyperautofluorescent. The fourth patient with a remote
history of central artery occlusion had no identifiable plaque or hyper or hypoautofluorescence on FAF.
Conclusions: In all three cases who presented acutely, FAF showed initial sectoral hypoautofluorescence of the
nonperfused retina which resolves over 1 month. The etiology of the hypoautofluorescence may be secondary to
inner retinal or ganglion cell thickening blocking the RPE autofluorescence, or the emission spectra of oxygenated
and deoxygenated NADH and FAD. This is the first description of hyperautofluorescence of the arterial plaques in
retinal artery occlusions that persists to at least 1.5 months later. Plaque components, such as calcium or cholesterol,
could determine the plaque's autofluorescence characteristics. This technique could be a non-invasive alternative to
fluorescein angiography to document retinal non-perfusion in retinal artery occlusions in patients without an easily
identifiable plaque and may direct the embolic work-up to identify plaques, diagnose, and clinically follow retinal
artery occlusions.
Commercial Relationships Disclosure (Abstract): Yannis Paulus: Commercial Relationship: Code N (No
Commercial Relationship) | Aazim Siddiqui: Commercial Relationship: Code N (No Commercial Relationship) |
Adrienne Scott: Commercial Relationship: Code N (No Commercial Relationship)
113
Poster Board Number: P32
Infrared and Fundus Autofluorescence Imaging in the Evaluation and Monitoring of Peripheral Retinoschisis
Author(s): Timothy Kao, Sandra R. Montezuma, Dara Koozekanani, Philip Turner, Torey Miller
University of Minnesota
Purpose: To describe the previously unreported appearance of peripheral retinoschisis with infrared (IR) and
fundus autofluorescence (FAF) imaging.
Methods: Patients at the University of Minnesota found to have peripheral retinoschisis underwent IR and FAF
imaging in addition to color fundus photography and optical coherence tomography (OCT). IR and FAF images
were obtained using a Heidelberg Spectralis HRA + OCT with 102 and 55 degree non-contact lenses, respectively.
Retinoschisis was confirmed by clinical exam and OCT.
Results: Five eyes of five patients with peripheral retinoschisis underwent peripheral IR imaging, and four also had
peripheral FAF imaging. Peripheral OCT confirmed the presence of retinoschisis in all eyes. IR and FAF imaging in
all but one eye showed retinoschisis as clearly demarcated areas of elevation with hypoautofluorescence,
respectively. Subtler changes were seen in the last eye, which had more shallow retinoschisis. In most cases, IR and
FAF imaging enabled better visualization of the retinoschisis borders compared to color photos, especially relative
to retinal vascular landmarks and with media opacity, as demonstrated in one case with a cataract. Inner retinal holes
were well visualized on IR imaging. In one case, the retinoschisis had a hyperautofluorescent border.
Conclusions: Peripheral IR and FAF imaging are useful modalities that can supplement traditional Methods of
evaluating and monitoring peripheral retinoschisis. This case series demonstrates how IR and FAF imaging may
allow better discrimination of retinoschisis borders relative to retinal landmarks compared to color photos alone,
especially in the presence of media opacities. As the collection of IR and FAF images in retinoschisis grows, further
work will be done to identify features that correspond to chronicity and stability of retinoschisis.
A. FAF image showing superotemporal hypoautofluorescence at site of retinoschisis with hyperautofluorescent
border B. IR image showing clear edge of retinoschisis and inner retinal hole C. Color photo showing bullous
retinoschisis D. OCT confirms retinoschisis
114
A. FAF image showing hypoautofluorescence inferotemporally at site of retinoschisis
B. IR image showing clear edge of retinoschisis
C. Retinoschisis is difficult to visualize on color photos
D.OCT confirms retinoschisis
Commercial Relationships Disclosure (Abstract): Timothy Kao: Commercial Relationship: Code N (No
Commercial Relationship) | Sandra Montezuma: Commercial Relationship: Code N (No Commercial Relationship) |
Dara Koozekanani: Commercial Relationship: Code N (No Commercial Relationship) | Philip Turner: Commercial
Relationship: Code N (No Commercial Relationship) | Torey Miller: Commercial Relationship: Code N (No
Commercial Relationship)
115
Poster Board Number: P33
False Negatives in the Delineation of Age-related Geographic Atrophy by Fundus Autofluorescence “
Author(s): David J. Ramsey1, Carol Applegate2, Janet S. Sunness2
1
Massachusetts Eye & Ear Infirmary, 2Greater Baltimore Medical Center
Purpose: To demonstrate instances where, paradoxically, geographic atrophy (GA) is present on color photographs,
but is not visible on fundus autofluorescence (FAF) images.
Methods: Color fundus photographs and FAF images were analyzed for the study eye for each of 71 participants in
a clinical trial for GA. Baseline, year 1, and year 2 images were analyzed. GA was outlined in the best macular
image for each modality, and the findings were compared.
Results: As is common, FAF often helped to distinguish small areas of GA from drusen, and often gave sharper
borders of GA. Color fundus images were useful for defining the extent of foveal involvement, since blockage by
xanthophyll darkens the foveal region and may mask the presence of spared areas. Color fundus images were also
useful for determining that small areas with loss of FAF were indeed GA and not drusen. For 2 patients, there was
atrophy in the foveal region that was not identified in the FAF image because of the pre-existing darkness of the
central region. Surprisingly, for 3 patients (4%), there were significant areas of what appeared to be definite
extrafoveal GA on color images that was not identified on FAF images. At baseline, these measured 3.3 mm2 in one
patient and 3.0 mm2 in the second. The third patient had 2 areas, measuring 1.8 mm2 and 2.5 mm2. Over the followup, FAF began to show evidence of GA in these areas, but there was not complete agreement between FAF and the
color even at 2 years. For 3 of the 5 patients, infrared reflectance images were available and they showed the GA
that was missed on the FAF images.
Conclusions: FAF is extremely sensitive for the presence of GA, but rarely there are regions that would clinically
be considered GA and yet the FAF does not show loss of autofluorescence. Some complement to FAF is thus
needed, and the IR reflectance image is likely to perform nearly as well as color images for delineating GA in
difficult cases.
Commercial Relationships Disclosure (Abstract): David Ramsey: Commercial Relationship: Code N (No
Commercial Relationship) | Carol Applegate: Commercial Relationship: Code N (No Commercial Relationship) |
Janet Sunness: Commercial Relationship(s);Acucela:Code C (Consultant);Advanced Vision Therapies:Code C
(Consultant);Alcon:Code C (Consultant);Cell Cure:Code C (Consultant);Eyetech:Code C
(Consultant);Genentech:Code C (Consultant);GSK:Code C (Consultant);Health Advances, LLC:Code C
(Consultant);Jerini:Code C (Consultant);Johnson & Johnson:Code C (Consultant);Merck:Code C
(Consultant);Neurotech:Code C (Consultant);Novartis:Code C (Consultant);Ophthotech:Code C
(Consultant);Othera:Code C (Consultant);Pfizer:Code C (Consultant);Potentia:Code C (Consultant);Shire:Code C
(Consultant);Sucampo:Code C (Consultant);ReVision:Code C (Consultant)
116
Poster Board Number: P34
Inexpensive 3D Telemedicine: Integrating smartphone technologies in an ophthalmological stereoscopic
evaluation
Author(s): Jorge-Emmanuel Morales-León
Instituto de Oftalmologia Fundacion Conde de Valenciana IAP
Purpose: To present a novel method of capturing and viewing stereoscopic ophthalmological pictures and videos
of anterior and posterior segment using inexpensive smartphone technology applied to a common slit lamp.
Methods: Smartphone slit lamp adapters have turned common slit lamps into powerful photographic devices. By
using two simple smartphone adapters attached to slit lamp oculars and combining these with a voice-trigger
application and a prism stereoscopic viewer, we can obtain high defintion state-of-the-art images of ophthalmic
examination for different clinical applications using simple applied technology.
Results: We were able to adapt this system to almost every kind of slit lamp available in our hospital and to send
and recieve images taken with that method and viewing them in 3D. We will discuss the different clinical
applications and implications of this kind of imaging.
Conclusions: It is possible to obtain quality stereoscopic imaging of anterior and posterior segment by combining
everyday technology props and mobile devices and applications.
Commercial Relationships Disclosure (Abstract): Jorge-Emmanuel Morales-León: Commercial Relationship:
Code N (No Commercial Relationship)
117
Poster Board Number: P35
Fundus mask and lens dust detection in retinal images with applications to automated diabetic retinopathy
screening
Author(s): Kaushal Solanki, Malavika Bhaskaranand
Eyenuk, Inc.
Purpose: Retinal images contain retinal information only in certain regions that can be identified by a fundus mask.
Therefore it is essential that fundus masks are computed accurately to constrain further automated DR analysis to
only regions with retinal information. Furthermore, lens dust artifacts are common in real-life retinal images and in
many cases can be mistaken for lesions by both human readers and image analysis algorithms, possibly leading to
incorrect diagnoses. These artifacts are caused either due to improperly cleaned lenses or light flares/reflections. In
this work, we propose fully automatic algorithms to compute fundus masks and detect lens dust artifacts.
Methods: We recognize that for all images captured during an encounter (given visit of a given patient), the fundus
masks are identical and the lens dust manifest as persistent artifacts. We utilize these facts to compute the fundus
mask and detect lens dust using computationally simple algorithms. The fundus mask is computed by first taking the
differences between each pair of the images within the encounter, and then thresholding the median of differences.
Lens dust detection is performed after normalizing the images using novel local background estimation to enhance
the image. Differences of pairs of the normalized images are computed and a pixel is declared to be due to lens dust
if the differences are small-valued and lie within a small interval.
Results: The test image set consists of 836 images belonging to 165 encounters each with 4-8 images. Our fundus
mask algorithm achieves high accuracy across this test set and Fig. 1 shows results for 3 encounters. The lens dust
detection algorithm identifies artifacts ranging from prominently visible to faint as shown in Fig. 1. The algorithm
parameters have been chosen so that true lesions are not mistakenly marked as lens dust.
Conclusions: The proposed algorithms for detecting the fundus mask and lens dust artifacts in retinal images are
accurate and computationally inexpensive. They can be used to inform automated DR analysis algorithms for
improved performance.
118
Fig. 1: Fundus masks and lens dust masks for different encounters. The fundus mask is accurately detected. Various
types of lens dust artifacts (indicated by arrows in images) are detected: lens flare (encounter A); large, dark artifact
(encounter B); and faint lesion-like artifact (encounter C).
Commercial Relationships Disclosure (Abstract): Kaushal Solanki: Commercial Relationship(s);Eyenuk,
Inc.:Code E (Emplyment) | Malavika Bhaskaranand: Commercial Relationship(s);Eyenuk, Inc.:Code E (Emplyment)
119
Poster Board Number: P36
Non mydriatic hand held camera -An effective screening tool for diabetic population in hands of paramedical
health workers
Author(s): Sundaram Natarajan1, 2, Purva Valvekar1, Deepen Sheth1, Sunita Mohan2, Radhika Krishnan2, Pandurang
Kulkarni1
1
Aditya Jyot Eye Hospital, 2Aditya Jyot Foundation for Twinkling Little Eyes
Purpose: To bridge the gap between health care personnel through hand held camera for screening of diabetic slum
population.
Methods: Study design -Cross sectional Study period – 1 month Sample size- 100 known type 2 diabetic patients.
Source of patients- Known Type 2 diabetic patients from the slum areas of Dharavi Research material- Hand held
non mydriatic camera {Optomed Smartscope M5 , Optomed Oy (Ltd.), Oulu, Finland} and trained health care
paramedical workers. Awarness among the slum population about diabetic retinopathy and its resulting visual loss
was emphasized using fundus photographs. 100 known type 2 diabetic patients from the slum areas of Dharavi were
screened by trained paramedical health workers. Data was analyzed by retina specialist for diagnosis & grading of
diabetic retinopathy. Patients who required treatment were called to base hospital for further evaluation and
management.
Results: Prevalence of diabetic retinopathy was 14%. Around 3 % had sight threatening diabetic retinopathy
requiring treatment.
Conclusions: Diabetic retinopathy screening with a compact handheld non-mydriatic fundus camera improved the
quality of care for diabetic patients in slums of Dharavi. This screening method was cost effective, easy tool to
identify patients requiring prompt referral to the ophthalmologist for further complete eye examination and
treatment. It was found possible to extend this screening to the door step through community health workers.
Commercial Relationships Disclosure (Abstract): Sundaram Natarajan: Commercial Relationship: Code N (No
Commercial Relationship) | Purva Valvekar: Commercial Relationship: Code N (No Commercial Relationship) |
Deepen Sheth: Commercial Relationship: Code N (No Commercial Relationship) | Sunita Mohan: Commercial
Relationship: Code N (No Commercial Relationship) | Radhika Krishnan: Commercial Relationship: Code N (No
Commercial Relationship) | Pandurang Kulkarni: Commercial Relationship: Code N (No Commercial Relationship)
120
Poster Board Number: P37
Hand-held non-mydriatic digital fundus imaging for the detection of diabetic retinopathy
Author(s): Steven R. Cohen, Grace E. Boynton, Cagri G. Besirli, Maria A. Woodward, Paula Anne Newman-Casey
University of Michigan
Purpose: To describe early experiences using a hand-held non-mydriatic digital fundus camera for diabetic
retinopathy (DR) screening.
Methods: In this prospective pilot study, diabetic patients underwent non-mydriatic, hand-held fundus imaging
(Pictor, Volk®) followed by mydriatric ultrawide-field (UWF) imaging (Optos®) and dilated fundus examination by
a retina specialist. Forty-five degree-field fundus images were obtained in 3 fields (posterior pole, nasal,
superotemporal) prior to dilation using the hand-held digital imager. The hand-held fundus images were taken by
both a certified ophthalmic photographer and a medical student not trained in ophthalmic photography. A single,
masked retina specialist graded all images to assess image quality and presence of DR.
Results: Twenty-three eyes (12 patients) underwent ophthalmic imaging. Patient ages ranged from 31-73 years and
mean Hemoglobin A1c was 8.0 (6.0-14.0). No eyes had significant media opacities. Twenty-one of 23 (91%) UWF
images were gradable. Of the 68 fields taken with the hand-held camera, 34 (50%) were gradable. Of the hand-held
images taken by the ophthalmic photographer, 20/35 (57%) were gradable, while 14/33 (42%) of the images taken
by the medical student were gradable. The nasal images had the poorest quality (9/23 gradable), while the
superotemporal images had the highest quality (18/23 gradable). In 5 eyes, all 3 fields were gradable with the handheld camera. Of these 5 eyes, DR was accurately detected in 4 (80%). One patient had mild nonproliferative DR
(NPDR) on exam that was not detected on fundus imaging. Of the eyes that had at least 1 gradable 45°-field, DR
was accurately assessed in 14/18 (78%). Of the 4 eyes that were not accurately assessed, NPDR was present in 3
eyes on clinical exam. Of the 21 gradable UWF images, DR was accurately assessed in 19 (90%).
Conclusions: Non-mydriatic, hand-held digital fundus imaging may have a useful role in DR screening in the
future. Non-ophthalmic personnel can effectively perform the imaging, although the greater proportion of higher
quality images taken by the ophthalmic photographer reveals the importance of strong training in this new screening
modality. Used with appropriate training in a primary care setting or in underserved areas, hand-held imaging may
provide a cost-effective screening method to serve the growing diabetic population.
Commercial Relationships Disclosure (Abstract): Steven Cohen: Commercial Relationship: Code N (No
Commercial Relationship) | Grace Boynton: Commercial Relationship: Code N (No Commercial Relationship) |
Cagri Besirli: Commercial Relationship: Code N (No Commercial Relationship) | Maria Woodward: Commercial
Relationship: Code N (No Commercial Relationship) | Paula Anne Newman-Casey: Commercial Relationship: Code
N (No Commercial Relationship)
121
Poster Board Number: P38
Can Heidelberg MultiColor images be used interchangeably with color fundus photography for grading agerelated macular degeneration features?
Author(s): Katie Graham3, Patrick Larkin2, 3, Katherine Alyson Muldrew2, 3, Vittorio Silvestri1, 3, Graham Young1, 2,
Philip McIntyre1, Helen McAtamney1, Ruth E. Hogg3
1
Belfast Health and Social Care Trust, 2Queen's University Belfast, 3Queen's University
Purpose: To characterize the appearance of age-related macular degeneration features (AMD) on Heidelberg
MultiColor images(MCI) and then systematically compare their appearance with color fundus photography (CFP).
Methods: Study design: Observational case series. Participants: 30 patients attending Macular clinics in Belfast
and 30 participants from the Northern Ireland Cohort for the Longitudinal study of aging (NICOLA). Images were
obtained after dilation using both CFP and cSLO MCI (Heidelberg Engineering, Germany) using standardized
protocols. Color fundus photographs were assessed and clinical features of AMD noted (hard drusen, soft drusen,
reticular pseudodrusen, geographic atrophy, haemorrhage and fibrosis), the constituent images from the cSLO
imaging were assessed in turn (infrared(IR), green reflectance(GR), blue reflectance(BR) and composite
MultiColor) and the presence or absence of the features noted on CFP was determined. Features present on
MultiColor and absent on CFP were also noted. Test characteristics were determined and a matrix describing the
appearance of AMD features on the different images was constructed. Examples of artefact’s were also collected.
Results: A total of 99 eyes with gradable images were available for comparison (56 eyes from patients and 43 eyes
from NICOLA study participants). Using CFP as the gold standard, sensitivity values for MCI ranged from 100%
for fibrosis to 68% for soft drusen. Specificity values were high (95%+) for all features except hard drusen
(75%). For all AMD features except haemorrhage there were instances where features were noted on MCI but not
on CFP. When features were present on MCI their edges usually appeared more distinct than on CFP.
Conclusions: Although sensitivity and specificity values were high for most AMD features it is unlikely that these
technologies could be used interchangeably. Careful interpretation is also required given the different appearance of
features on CFP and MCI. Given the improved definition of features on MCI it may prove most useful in situations
where measurement of lesion size is important.
Commercial Relationships Disclosure (Abstract): Katie Graham: Commercial Relationship: Code N (No
Commercial Relationship) | Patrick Larkin: Commercial Relationship: Code N (No Commercial Relationship) |
Katherine Alyson Muldrew: Commercial Relationship: Code N (No Commercial Relationship) | Vittorio Silvestri:
Commercial Relationship: Code N (No Commercial Relationship) | Graham Young: Commercial Relationship:
Code N (No Commercial Relationship) | Philip McIntyre: Commercial Relationship: Code N (No Commercial
Relationship) | Helen McAtamney: Commercial Relationship: Code N (No Commercial Relationship) | Ruth Hogg:
Commercial Relationship: Code N (No Commercial Relationship)
122
Poster Board Number: P39
Ultra high resolution imaging of subepithelial ocular pathologies
Author(s): James R. Wong1, Madhura G. Joag1, Afshan A. Nanji1, Juan Murillo1, Nabeel M. Shalabi1, 2, Marwan A.
Atallah1, Ibrahim Sayed-Ahmed1, Anat Galor1, 2, Carol L. Karp1
1
University of Miami Miller School of Medicine, 2Miami Veterens Affairs Medical Center
Purpose: To describe subepithelial ocular pathologies using ultra high resolution optical coherence tomography
(UHR OCT)
Methods: Twenty five patients with subepithelial pathologies, consisting of 9 lymphomas, 4 lymphangiectases, 4
with Salzmann’s nodular degeneration (SND), 2 conjunctival amyloidoses, 2 corneal keloids, 2 anterior basement
membrane dystrophies (ABMD), 1 vernal keratoconjunctivitis (VKC) with Horner-Trantas dots, and 1 benign
lymphoid hyperplasia (BLH). Clinical features, slit-lamp photos and UHR OCT scans (RTVue premier, Optovue,
Fremont, CA, USA) are described.
Results: UHR OCT assisted in the diagnosis of the subepithelial lesions. In SND, small, hyperreflective, discrete,
well-circumscribed, nodules occurred between the epithelium and Bowman’s layer, with thinning of the overlying
epithelium. Changes in ABMD were very subtle in comparison, but similarly showed hyperreflective, moderately
thickened, subtle subepithelial material extending anteriorly into the epithelium (Fig. 1). Corneal keloid appeared as
a hyperreflective, inhomogeneous, elevated, well-circumscribed, space-occupying lesion with variable depth of
involvement. In VKC, Horner-Trantas dots appeared as intermediately reflective lesions with variable depth and
some intraepithelial involvement. Conjunctival amyloidosis appeared as a well-demarcated lesion with
hyporeflective areas interspersed with areas of inhomogeneous hyperreflectivity. Lymphangiectasis appeared as
hyporeflective spaces with hyperreflective borders suggestive of dilated channels (Fig. 2). Lymphoma appeared as a
homogenous, hyporeflective lesion with small stippled, hyperreflective dots suggestive of a homogenous cellular
infiltrate. BLH appeared similarly as a well-circumscribed, homogenous, hyporeflective lesion with some
shadowing. However, these last two lesions could not be differentiated by UHR OCT.
Conclusions: UHR OCT is a useful adjuvant tool in the diagnosis of subepithelial ocular pathologies
Fig. 1. A: SND (arrows), B: corresponding UHR OCT shows hyperreflective material deposited above
Bowman’s layer (arrow). C: ABMD (arrow), D: corresponding UHR OCT shows subtle hyperreflective
material (arrows)
123
Fig. 2. A: Biopsy-proven conjunctival amyloidosis, B: corresponding UHR OCT shows interspersed heterogeneous
hyporeflective (up arrow) and hyperreflective material (down arrow). C: Conjunctival lymphangiectasis, D:
corresponding UHR OCT shows dilated lymphatic channel (arrow)
Commercial Relationships Disclosure (Abstract): James Wong: Commercial Relationship: Code N (No
Commercial Relationship) | Madhura Joag: Commercial Relationship: Code N (No Commercial Relationship) |
Afshan Nanji: Commercial Relationship: Code N (No Commercial Relationship) | Juan Murillo: Commercial
Relationship: Code N (No Commercial Relationship) | Nabeel Shalabi: Commercial Relationship: Code N (No
Commercial Relationship) | Marwan Atallah: Commercial Relationship: Code N (No Commercial Relationship) |
Ibrahim Sayed-Ahmed: Commercial Relationship: Code N (No Commercial Relationship) | Anat Galor:
Commercial Relationship(s);Bausch + Lomb:Code C (Consultant) | Carol Karp: Commercial Relationship: Code N
(No Commercial Relationship)
124
Poster Board Number: P40
Topographic analysis of outer retinal atrophy in type 2 idiopathic macular telangiectasia
Author(s): Ferenc B. Sallo1, 2, Irene Leung1, Valérie Krivosic5, Vincent Rocco1, Kiyoko Gocho8, Michel Paques6, 7,
Tunde Peto4, 1, Alan C. Bird3, Alain Gaudric5
1
Moorfields Eye Hospital, 2UCL Institute of Ophthalmology, 3Moorfields Eye Hospital, 4NIHR Biomedical
Research Center for Ophthalmology, at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of
Ophthalmology, 5Université Paris Diderot, Hopital Lariboisière, 6CHNO des Quinze-Vingts, 7Institut de la Vision ,
8
Chiba Hokusoh Hospital, Nippon Medical University
Purpose: Type 2 macular telangiectasia (MacTel) is associated with outer retinal abnormalities at and near the
foveal centre. Optical Coherence Tomographic (OCT) topographic mapping of the IS/OS junction layer (or ellipsoid
zone) is a validated method for assessing disease severity in MacTel. On OCT, the photoreceptor outer segment tips
as well as the tight junctions between the photoreceptors and Muller cells are associated with clear signals (POST
line or interdigitation zone and external limiting membrane, ELM respectively). Adaptive optics (AO) imaging
offers a clarity and resolution superior to commercially available SD-OCT systems. Our aim was to examine outer
retinal morphology using these two imaging modalities.
Methods: Patients were selected from the MacTel Study cohort. OCT volume scans with 11-30µ B-scan intervals
were acquired using Heidelberg Spectralis OCT units. Automated segmentation and topographic mapping of the
POST (IZ), IS/OS (EZ) and ELM layers was reviewed and corrected manually. AO images of the fundus focusing
on the photoreceptors were captured using an Imagine Eyes rtx1 unit. OCT topographic maps and AO images were
superimposed and aligned. Lesions characteristic of the disease were analyzed in each imaging modality and results
were compared.
Results: Nineteen eyes of 10 MacTel patients (ranging in age 34-69 years, mean age 54.4, SD=14.1 years) were
examined. In 3 eyes no break was seen in any layer on OCT and the photoreceptor mosaic was imaged clearly and
appeared normal in AO images. 16 eyes demonstrated a defect in the IS/OS layer (EZ). Consistently, the POST (IZ)
break appeared larger, the ELM break (if present) smaller than the break in the IS/OS (EZ). In AO images, areas
corresponding to a break appeared featureless, their boundaries corresponded closest to those of the POST (IZ)
break.
Conclusions: AO imaging demonstrates abnormalities in the photoreceptor matrix corresponding to the defects in
the outer retinal layers seen on OCT. A topographic analysis of the outer retina may adjunct current Methods and
provide a tool for early detection as well as clues to the sequence of cellular degeneration in MacTel.
Commercial Relationships Disclosure (Abstract): Ferenc Sallo: Commercial Relationship: Code N (No
Commercial Relationship) | Irene Leung: Commercial Relationship: Code N (No Commercial Relationship) |
Valérie Krivosic: Commercial Relationship: Code N (No Commercial Relationship) | Vincent Rocco: Commercial
Relationship: Code N (No Commercial Relationship) | Kiyoko Gocho: Commercial Relationship: Code N (No
Commercial Relationship) | Michel Paques: Commercial Relationship: Code N (No Commercial Relationship) |
Tunde Peto: Commercial Relationship: Code N (No Commercial Relationship) | Alan Bird: Commercial
Relationship: Code N (No Commercial Relationship) | Alain Gaudric: Commercial Relationship: Code N (No
Commercial Relationship)
125
Poster Board Number: P41
Predicting Progression of Geographic Atrophy in Age-Related Macular Degeneration with Retinal Thickness
Measurements using Spectral Domain Optical Coherence Tomography
Author(s): Praveena Gupta2, Kevin Wells1, Vincent Nguyen3, Bernard F. Godley1, Gibran Khurshid1
1
University of Texas Medical Branch, 2UNiversity of Texas medical Branch, 3Teaxs A&M Health Science Center
School of medicine
Purpose: To test whether retinal thickness measurements, as measured by spectral domain optical coherence
tomography (SD-OCT), can be utilized to predict the enlargement rate (ER) of geographic atrophy (GA) secondary
to age related macular degeneration.
Methods: Patients with the diagnosis of GA and 2 sets of imaging studies (fundus autofluorescence [FAF] and SDOCT) at least 6 months apart were identified. Fifteen eyes from 20 patients were included in this study. The ER of
GA for each patient was determined utilizing FAF images. Retinal thickness measurements were determined by
analyzing the patient’s initial SD-OCT B-scan that corresponded with the area of greatest GA in the linear X-axis.
The retinal layer boundaries were identified and manually separated. Three separate zones for each retinal layer
were analyzed: (1) the zone of GA, (2) the transition zone (200um lateral to the zone of GA), and (3) the peripheral
zone (200um lateral to the transition zone). The average thickness of each of these zones was determined and was
correlated with the ER of GA. All measurements were performed using the software ImageJ (NIH, Bethesda, MD).
Results: The mean follow-up time was 2.64 years. The average ER of GA was 1.77mm2/year. When applying the
square root transformation of the GA area measurements, the average ER was 0.30mm/yr. The combined thickness
of the RPE and photoreceptor layer at the nasal transition zone inversely correlated with the square root
transformation ER (Spearman r=-0.638, p=0.010, n=15). However, a photoreceptor layer was only identified in 9 of
the 15 eyes at the nasal transition zone. The thickness of the photoreceptor layer in those 9 eyes inversely correlated
to the square root transformation ER (Spearman r=-0.669, p=0.049, n=9). All other thickness measurements did not
correlate with the ER.
Conclusions: SD-OCT microstructure analysis of the transitional zone can provide unprecedented insight into the
progression of the geographic atrophy. Such additional information can serve as a promising marker for disease
monitoring and therapeutic interventions.
Commercial Relationships Disclosure (Abstract): Praveena Gupta: Commercial Relationship: Code N (No
Commercial Relationship) | Kevin Wells: Commercial Relationship: Code N (No Commercial Relationship) |
Vincent Nguyen: Commercial Relationship: Code N (No Commercial Relationship) | Bernard Godley: Commercial
Relationship: Code N (No Commercial Relationship) | Gibran Khurshid: Commercial Relationship: Code N (No
Commercial Relationship)
126
Poster Board Number: P42
En-Face Analysis of Spectral Domain Ocular Coherence Tomography (SD-OCT) in Acute Multifocal Placoid
Pigment Epitheliopathy (AMPPE)
Author(s): Kanchan Bhan1, Adam Dubis1, 2, Carlos Pavesio1
1
Moorfields Eye Hospital, 2University College London
Purpose: To establish what role En-face analysis in SD-OCT may have in diagnosis, monitoring and understanding
the pathophysiology of AMPPE
Methods: We present a case (within a series) of AMPPE on which pre and post treatment macular SD-OCT
(Spectralis, Heidelberg) and En-face analysis (generating C Scans using Image J) was performed. SD-OCT images
were correlated with En-face analysis and further correlation was undertaken with indocyanine green angiography
(ICGA), fluorescein angiography (FA) and clinical examination.
Results: Pre-treatment SD-OCT revealed acute phase hyper-reflectivity of the photoreceptor inner segment/outer
segment (IS/OS) junction with multiple serous sub neurosensory retinal detachments bilaterally. Serous detachments
contained hyper-reflective material. Acute phase En-face analysis revealed discrete hyporeflective areas at the level
of the IS/OS junction which correlated positively with hypocyanescent areas on ICGA. These areas, in turn,
correlated well with placoid fundus lesions visible clinically and on FA. Serous detachments also appeared as
hyporeflective areas on En-face analysis with hyper-reflective material within at the former level of the IS/OS
junction. Hyper-reflective spots within the choriocapillaris on ehanced depth imaging (EDI) SD-OCT were revealed.
Post steroid treatment SD-OCT revealed decreased reflectivity of the IS/OS junction and resolution of sub retinal
fluid. Post-treatment En-face analysis revealed thinning of the IS/OS junction and mottled increased reflectivity at
this level which correlated with RPE changes visible clinically.
Conclusions: En-face analysis of SD OCT correlates well with hypocyanescent lesions on ICGA diminishing the
need for ICGA in diagnosis and disease monitoring. En-face analysis also enables accurate depth localisation of the
pathophysiological process, in this case, suggesting that the IS/OS junction is involved in the acute process EDI
findings suggest that the pathophysiology includes that of inflammation of the choriocapillaris.
127
Pre-treatment SD-OCT showing left serous sub retinal fluid with hyper-reflective material within correlating well
with hypo-reflective area on en-face analysis<br /> <br /> Post treatment SD-OCT showing right IS/OS junction
thinning correlating with mottled reflectivity on en-face analysis
Commercial Relationships Disclosure (Abstract): Kanchan Bhan: Commercial Relationship: Code N (No
Commercial Relationship) | Adam Dubis: Commercial Relationship: Code N (No Commercial Relationship) | Carlos
Pavesio: Commercial Relationship: Code N (No Commercial Relationship)
128
Poster Board Number: P43
Optical Coherence Tomography (OCT) detects epiretinal membrane formation after intravitreal injection
of anti VEGF in cases of Diabetic macular edema
Author(s): Soheir Mahmoud Ali
Cairo University
Purpose: To assess the frequency of formation of epiretinal membrane after intravitreal injection (IV) of ranibizumab (Lucentis) and bevacizumab (Avastin) in cases of Diabetic macular edema using spectral domain OCT
Methods: The study included 60 eyes of NPDR having Diabetic macular edema that required intravitreal injection
of anti VEGF. Each eye had full ophthalomological examination ( best corrected visual acuity,anterior segment
examination, intraocular pressure measurement, fundus examination) then OCT was performed for each eye to
record central foveal thickness, juxtafoveal thickness in the four quadrants, presence of cystoid spaces. Exkusion
criteria were: #Previous intraocular surgery, or intravitrel injections or laser treatment. #Presence of epiretinal
membranes or vitreoretinal traction.#Elevated IOP. Eyes were divided into two groups each of 30 eyes. Group I had
IV injection of Lucentis and Group II had Iv injection of Avastin. Recording epiretinal membrane formation or
vitreoretianl surface changes was performed by OCT at 1,2 and 3 months after injections. Results were recorded ,
correlated to IS/OS integrity and retinal thickness then statistically analyzed.
Results: After 1 month ERM was detected in 72% of cases of group 1 and 70% of group 2. After 2 month ERM
was detected in 76% of cases of group 1 and 74% of group 2. After 3 months no significant chages were detected
compared to features after 1 and 2 months. Fragmented ERM was 20% in gp1 and 26% in Gp 2. Thightly aherent
ERM was 30% in Gp1 and 35% in Gp2. Cleavage lines were detected in 30% in GP1 and 28% in Gp2. Free edges
were detected in 40% in Gp1 and 35% in Gp2. Vitreoretinal traction was detected in 10% in GP1 and 12% in Gp 2.
No significant correlation was detected with IS/Os segment regularity in both GPs.
Conclusions: OCt can successfully detect ERM fomation as a complication after IV injection of antiVEGf which
was highly significantly detected. ERM formation percentage was more after Avastin than after lucentis injection
but the results did not show high significant difference.
Commercial Relationships Disclosure (Abstract): Soheir Mahmoud Ali: Commercial Relationship: Code N (No
Commercial Relationship)
129
Poster Board Number: P44
Enhanced Depth Imaging Optical Coherence Tomography of the Choroid in Chinese Normal Highly Myopic
Eyes
Author(s): Fenghua Wang2, 1, Yanping Zhou1, Xiaodong Sun1
1
Shanghai Firist People's Hosptial, 2Shanghai First People
Purpose: To investigate the choroidal thickness and characteristics by enhanced depth imaging optical coherence
tomography (EDI OCT) in the subjects of high myopia with good corrected visual acuity.
Methods: 55 subjects were recruited, from whom 91 eyes were diagnosed as high myopia with best corrected
visual acuity (BCVA) equivalent to 20/20. Subjects were scheduled for a spectral-domain optical coherence
tomography (SD-OCT) scanning with a HD line Raster in two directions (Horizontal & Vertical) with the enhanced
depth imaging technique. The choroidal thickness (CT) was manually measured in 12 locations (0.5mm, 1.5mm and
3mm away from the fovea in four directions). Furthermore, the central foveal retinal thickness (CFRT) and the
central subfoveal choroidal thickness (CSFCT) were also analyzed for their correlations with age and axial length
(AxL).
Results: Mean age of the 55 subjects (91 eyes) is 35.7±10.7 years old, mean spherical equivalent refraction is 8.56±1.61D, and mean AxL is 26.97±0.87mm. The mean central foveal retinal thickness was 106.8±5.4μm and was
the thinnest both in vertical and in horizontal direction. The mean central subfoveal choroidal thickness is
173.6±57.4μm, negatively correlated with age and axial length. Horizontally, choroidal thickness became thinner
from the temporal side to the nasal side. The choroid was thinnest at 3.0 mm nasally away from the fovea, while the
CSFCT was thinnest in vertical direction.
Conclusions: In the eyes without myopic maculopathy, the foveal retinal thickness of normal highly myopic eyes
remains in the normal range. Nevertheless, the central subfoveal choroidal thickness of highly myopic eyes decrease
compared with normal eyes. Choroidal thinning is related with high myopia which may be a useful diagnostic
parameter for high myopia and even a predictor to monitoring the continuing progress of pathological myopia.
Commercial Relationships Disclosure (Abstract): Fenghua Wang: Commercial Relationship(s);Carl Zeiss
Meditec:Code C (Consultant);Heidelberg Engineering:Code R (Recipient) | Yanping Zhou: Commercial
Relationship: Code N (No Commercial Relationship) | Xiaodong Sun: Commercial Relationship: Code N (No
Commercial Relationship)
130
Poster Board Number: P45
Optical Coherence Tomography (OCT) to Detect Disease Progression in Birdshot Chorioretinopathy (BCR) –
A Novel Multi-View Approach
Author(s): William R. Tucker1, Gregory Short2, Robert Nussenblatt1, Nida Sen1
1
NEI, 2National Institutes of Health
Purpose: To highlight a valuable ability of Spectral Domain OCT scanners to non-invasively show retinal vascular
leakage during the treatment and monitoring phases of BCR. OCT guided detection and monitoring of uveitic
macula edema secondary to BCR is well established, however fluorescein angiography (FA) is the accepted gold
standard for identifying the posterior pole vascular leakage common during disease recrudesence. We aim to
demonstrate that simple, safe, quick OCT techniques can provide similar information.
Methods: Five BCR patients were selected for inclusion and follow-up in this pilot study. As part of their standard
of care at each visit they received a fovea centered OCT macula cube 512 x 128. In addition a macula cube was
obtained centered on the optic disc, superotemporal arcade and inferotemporal arcade. The standard software was
able to compare retinal thickness differences between visits and highlighted areas of thickening or thinning next to
the vessels as demonstrated in Figure 1. Perivascular thickening suggestive of increased vascular leakage was
confirmed with subsequent FA.
Results: Mean length of follow-up during which the OCTs were obtained was 7 months (range 4 to 24 months).
During this time 4/5 patients experienced a disease flare with increased symptoms, worsening FA findings and
functional testing (e.g. Visual field testing). 5/5 patients also had periods of disease remission after initiation of
higher dose treatments. OCT was able to detect perivascular thickening during disease flares and thinning during
disease remission.
Conclusions: Modern OCT scanners have the ability to precisely measure retinal thickness, with software that can
detect subtle changes between visits. We hope to highlight a simple yet novel adaptation of scanning technique
which can provide clinically important information. In disease entities like BCR, characterized by posterior pole
vascular leakage, it can be used to detect recurrence, guide the need for FA and monitor the response to treatment.
131
Figure 1: A) Multi-view OCT thickness map of right eye in an asymptomatic BCR patient on oral prednisone 20mg
once daily B) OCT map 2 months later following taper of prednisone to 7.5mg and return of symptomatic floaters
C) Thickness comparison map demonstrating perivascular retinal thickening, confirmed on FA (not shown) as
secondary to vascular leakage
Commercial Relationships Disclosure (Abstract): William Tucker: Commercial Relationship: Code N (No
Commercial Relationship) | Gregory Short: Commercial Relationship: Code N (No Commercial Relationship) |
Robert Nussenblatt: Commercial Relationship: Code N (No Commercial Relationship) | Nida Sen: Commercial
Relationship: Code N (No Commercial Relationship)
132
Poster Board Number: P46
Inferior chiasmal syndrome diagnosed by Optical Coherence Tomography (OCT) before any visual field
defects
Author(s): Shawkat S. Michel1, Monica Michel2
1
ophthalmology, Alberta, Canada, 2Akron General Hospital
Purpose: Optical Coherence Tomography (OCT) is widely used to study the macula and the retinal nerve fiber
layer (RNFL). Axons of the retinal ganglion cells form the RNFL that converge onto the optic nerve. These nerve
fibers run a long course in the orbit and intra-cranial to end at synapsis with the nerve cells of the lateral geniculate
body (visual fibers) or the nerve cells of the pretectal nucleus (pupillary fibers). Along their long course the nasal
RNFs decussate at the optic chiasma and go to the opposite optic tract. OCT provides invaluable information about
the structure and function (anatomy and physiology) of these long RNFs through its scanning of the RNFL
and accurately computing the thickness of the RNFL all around the optic disc.
Methods: This is a case study of a 36 year old male who complained of frequent headaches and whose OCT
showed abnormal thinning of the RNFL in exactly corresponding points inferiorly in each eye; the patient did not
have glaucoma. The striking point that led to the thought of an inferior chiasmal syndrome was that RNFL thinning
was in exactly corresponding points in each eye and there was also a great degree of symmetry as to the shape and
size of the area of the thin RNF (please see OCT image). Octopus eighty degrees static visual field test was
repeatedly normal in both eyes. Due to the RNFL defects in both eyes in this OCT I requested a pituitary MRI that
showed pituitary adenoma of significant size and the patient had partially hypophysectomy through the nasal route.
Results: Interpreting results of OCT must take in account the anatomy, physiology and pathology of different
layers of the retina and the RNFL. Because the RNFs extend a long course from the retina ganglion cells through
the optic nerve, the optic chiasma and the optic tract; invaluable information may be obtained by carefully
interpreting scans of the RNFL.
Conclusions: There have been some papers looking into OCT importance in the prognosis of cases that had
resection of pituitary adenomas. To the best of my knowledge there has been no papers talking about the possibility
of diagnosing pituitary enlargement by OCT.
133
This OCT made me think of possible inferior chiasmal syndrome; pituitary MRI showed significant enlargement of
the pituitary gland.
Commercial Relationships Disclosure (Abstract): Shawkat Michel: Commercial Relationship: Code N (No
Commercial Relationship) | Monica Michel: Commercial Relationship: Code N (No Commercial Relationship)
134
Poster Board Number: P47
Assessment of choroidal metastases with the Enhanced Depth Imaging Optical Coherence Tomography
Author(s): Efthymia Pavlidou1, Amit Arora1, Victoria Cohen1, Mandeep S. Sagoo1, 2
1
Moorfields Eye Hospital & Bart's and the London Hospital, 2UCL Institute of Ophthalmology
Purpose: To assess and describe the imaging features of choroidal metastases with the enhanced depth imaging
optical coherence tomography
Methods: Case series of patients with choroidal metastases
Results: 20 eyes of 14 patients with choroidal metastases underwent full ophthalmological examination and
imaging with enhanced depth imaging- optical coherence tomography. 5 patients had primary breast cancer, 6
patients had primary lung cancer, 2 had prostate cancer and 1 patient had carcinoid metastatic lesions. All the cases
(100%) presented clumps of hyperreflective deposits in the subretinal space and/or in the vascular choroidal layers
in variable degree. Subretinal fluid was present in 18 eyes (90%). The RPE / choriocapillaries complex showed
multiple, consecutive elevations causing a lumpy appearance in all the cases. The layer of the choriocapillaries was
almost diminished, while the major vascular choroidal layers appeared mainly as dilated hyporeflective lobules in
cases with prostate cancer followed by cases of breast and lung cancer. Secondary deposits from prostate and breast
cancer appeared more lobulated whilst those from lung cancer were more diffuse.
Conclusions: The enhanced depth imaging optical coherence tomography shows characteristic imaging patterns in
cases with choroidal metastases. These images can contribute to the diagnostic approach but further studies need to
establish its role better
Commercial Relationships Disclosure (Abstract): Efthymia Pavlidou: Commercial Relationship: Code N (No
Commercial Relationship) | Amit Arora: Commercial Relationship: Code N (No Commercial Relationship) |
135
Victoria Cohen: Commercial Relationship: Code N (No Commercial Relationship) | Mandeep Sagoo: Commercial
Relationship: Code N (No Commercial Relationship)
136
Poster Board Number: P48
Development of Imaging Biomarker Algorithms to Assess Drug Efficacy and Predict Responders
Author(s): Kristie Lin1, Tom Chang1, Allen Ho2, Rami Mangoubi3, David O'Dowd3, Nathan Lowry3, Lei
Hamilton3, John Irvine3, Sicco Popma4
1
Retina Institute of California, 2Wills Eye Hospital, 3C.S. Draper Laboratory, 4Janssen Research and Development
Purpose: Investigate the potential of retinal image based algorithms to assess drug efficacy and response
prediction.
Methods: Quantitative statistical features were extracted from OCT and SLO images and were correlated to
changes in Best Corrected Visual Acuity (BCVA) observed in a clinical study. Images and BCVA were drawn from
2 patient visits: the pre-procedure visit, and one post-procedure visit. Six biomarkers were mined from these images
and statistically analyzed individually. Algorithms were then applied to statistically fuse/pair features from
promising biomarkers to more accurately predict procedure success, and explain efficacy. The resulting algorithms
were tested for their ability to correctly classify 25 subjects into three categories: significant improvement (>15
letters of BCVA), moderate improvement (0 to 15 letters of BCVA), and no improvement (<0 letters of BCVA).
Results: Six biomarker features were selected, which generated 384 statistical features. Linear regression analysis
showed a relationship between changes in features value and BCVA. Three of the regression values positively
correlated with BCVA (between 0.22 and 0.38) and three others were inversely correlated (between -0.11 and 0.44). Individually, none of the 384 fused features separated the subjects into the 3 classification groups reliably.
However, 1300 paired features were identified as potential biomarkers of value (p=<0.02). Applying these pairing
exploratory algorithms to the subject data (n=25) showed approximately 200 pairs correctly classified 20 out of the
25 subjects (80%) and 32 pairs correctly classified 22 out of 25 subjects (88%). Independent, masked, statistical
analysis showed that these paired features were twice as significant compared to random data, thus increasing
confidence in the algorithms.
Conclusions: Results demonstrated that mined individual statistical imaging features are combinable into
fused/paired features, enabling classification results among the 3 categories; significant, moderate and no
improvement of BCVA. Future studies will focus on a larger sample size and automation of image feature extraction
to verify the algorithms in assessing efficacy and response prediction. However, initial imaging algorithms are
promising for prediction and efficacy.
Commercial Relationships Disclosure (Abstract): Kristie Lin: Commercial Relationship(s);Janssen
Pharmaceuticals, Inc:Code C (Consultant);Thrombogenics :Code C (Consultant) | Tom Chang: Commercial
Relationship(s);Janssen:Code C (Consultant) | Allen Ho: Commercial Relationship(s);Janssen:Code C
(Consultant);Alcon:Code F (Financial Support);Allergan:Code F (Financial Support);NIH/NEI:Code F (Financial
Support);Ophthotech:Code F (Financial Support);Regeneron:Code F (Financial Support);Thrombogenics:Code F
(Financial Support);Digisight:Code C (Consultant);Endooptiks:Code C (Consultant);Genetech:Code C
(Consultant);Regeneron:Code C (Consultant);Thrombogenics:Code C (Consultant);Alcon:Code C
(Consultant);Allergan:Code C (Consultant);PRN:Code C (Consultant);Second Sight:Code F (Financial Support) |
Rami Mangoubi: Commercial Relationship(s);Janssen:Code F (Financial Support) | David O'Dowd: Commercial
Relationship(s);Janssen:Code F (Financial Support) | Nathan Lowry: Commercial Relationship(s);Janssen :Code F
(Financial Support) | Lei Hamilton: Commercial Relationship(s);Janssen:Code F (Financial Support) | John Irvine:
Commercial Relationship: Code N (No Commercial Relationship) | Sicco Popma: Commercial
Relationship(s);Janssen Research and Development:Code E (Emplyment)
137