Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
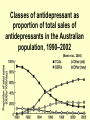
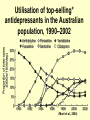
Antidepressants Sue Henderson Clinical Indications • Mood disorders • Anxiety disorders • Eating disorders • Chronic pain • Incontinence Personal perspective • “I don’t take Prozac for fun. And it has not changed my personality. I am not ridiculously happy but I do not spend most days miserable about being here, there or anywhere and no longer have a need to vomit before I have to talk to a work related colleague or deal with anything slightly stressful.” (Dietz, 2000, p. 37) Use of antidepressants in the Australian population, 1975– 2002 (Mant et al., 2004) Classes of antidepressant as proportion of total sales of antidepressants in the Australian population, 1990–2002 (Mant et al., 2004) Utilisation of top-selling* antidepressants in the Australian population, 1990–2002 (Mant et al., 2004) Major and sub-classes • • • • Based on 3 physiological actions: 1. Reuptake inhibition 2. Enzyme inhibition 3. Receptor blockade (Nash & Nutt, 2007). Reuptake inhibitors • Selective Serotonin Reuptake Inhibitors( SSRI) • Tricyclic Antidepressants (TCAs) • Selective Serotonin and NorAdrenaline Reuptake Inhibitors (SNRI) • Nor-adrenaline Reuptake Inhibitor (NARI) Enzyme inhibitors • The following antidepressant subclasses work by inhibiting the action of enzymes: • Reversible Inhibitors of Mono-Amine Oxidase type A (RIMA) • Mono-Amine Oxidase Inhibitors (MAOI) Receptor blockers • Nor-adrenergic and Specific Serotonin Antidepressants (NaSSA) work by blocking receptors. Therapeutic effect • Time lag of 2-4 weeks before antidepressant effect occurs. • Side effects & improved sleep occur earlier (Suicide risk). • 1st episode: Up to 1 year following recovery. • Repeat episodes: Up to 3 years (Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Depression, 2004). Stopping anti-d too early can lead to relapse Normal Mood Depression requiring treatment 2-4 weeks relief depression 1-3 weeks sex drive, self care, activity, memory 1st week sleep Begin antidepressant anxiety SSRIs available in Australia • • • • • • Citalopram Escitalopram Fluoxetine Fluvoxamine Paroxetine Sertraline Indications SSRIs • Mood disorders • Anxiety disorders Off label: • Premature ejaculation • Migraine headache, • Diabetic neuropathy • Fibromyalgia SSRI’s Action 1.Normally serotonin, a brain chemical is released from a nerve cell. 2.Serotonin is then received by the next nerve cell. 3.Some serotonin is then reabsorbed into the 1st nerve cell. 4.Not having enough serotonin may be associated with depression & anxiety disorders. SSRI’s block the reabsorbtion of serotonin into the 1st nerve cell. 5.This blocking action results in an increased amount of serotonin being available at the next nerve cell. SSRI’s block reuptake of serotonin into presynaptic neurone Neurotransmitter Re-uptake pump Receptor MAO Dendrite Axon Synapse Presynaptic storage vesicles 1st person account • “Some people look upon medication and/or therapy as some sort of life sentence, but to me, the alternative is a life sentence.” (Dietz, 2000, p. 37) The hype of Prozac Side-Effects: SSRI’s • Common: Nervousness & anxiety, insomnia (give dose in morning), drowsiness or fatigue, G.I nausea & diarrhoea, loss of appetite, weight loss, sexual dysfunction. Common Side Effects: SSRI Drug SSRI's Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline Daily range mg 20 - 40 20 - 40 100 - 200 20 - 40 50 - 100 Inso mnia ++ ++ ++ ++ ++ Sex Agit G.I.T Wt Dysf. ation gain +++ +++ +++ +++ +++ + ++ ++ = ++ ++ ++ ++ ++ ++ 0 0 0 + 0 Less common side effects • • • • • • Apathy Extrapyramidal side effects (EPSEs) Increased prolactin levels Serotonin syndrome Hyponatraemia Bruising and bleeding Increased risk of gastrointestinal bleeding (Loke, Trivedi, & Singh, 2008). Clinical response • SSRI’s produce a clinical response much more rapidly than tricyclic antidepressants. True or False? Serotonin syndrome • Prevention: do not co-administer SSRI’s and other drugs that increase serotonin. • Drug free interval before changing from SSRI to other serotonin drugs. Antidepressant discontinuation symptoms • • • • • • F = flu like symptoms I = insomnia N = nausea I = imbalance S = sensory disturbances H = hyperarousal (anxiety) in Carson, 2000, p. 432) (Gelenberg, 1998 cited Advantages SSRI’s • • • • • Minimal cardiac toxicity Safe in overdose Mild side effects Non sedating SSRI’s reduce overall suicide rates in depressed patients significantly more than tricyclic antidepressants. True or False? Tricyclic antidepressants:TCA’s Axon Dendrite Dendrite • Tricyclics block reuptake of noradrenaline & serotonin into presynaptic neurone. Tricyclics available in Australia • • • • • • • Amitriptyline Clomipramine Dothiepin Doxepin Imipramine Nortriptyline Trimipramine Indications • • • • Mood disorders OCD Panic disorder Neuralgia (nerve pain) - best available evidence is for amitriptyline (Saarto & Wiffen, 2007) • Nocturnal enuresis TCA Action: 4 actions 1. Block presynaptic noradrenaline reuptake pump (black lines). 2. Block the presynaptic serotonin reuptake pump (red lines). 3. Block histamine receptors (yellow square) = Sedative side effects. 4. Block post synaptic acetylcholine receptors (grey square) = Dry mouth, confusion, memory impairments, blurred vision. • This blocking action results in an increased amount of nor-epinephrine & serotonin being available to the post synaptic neuron. Side Effects: TCA’s Common • Sedation (give dose at night) • Dry mouth • Blurred vision • Weight gain • Constipation • Sweating. TCA S/E. Less common but important • postural hypotension • urinary retention • sexual dysfunction • raised intra-ocular pressure. Side Effects: TCA’s • Cardio-vascular effects in people with cardiac disease. • Impaired Cognitive function in dementia. • Precipitate a manic swing in bipolar. • May be fatal in O/D. Admit ICU, cardiac monitor Tetracyclics: Mianserin SE • Common: as for TCA’s, plus vivid dreams. • Less common: anti-cholinergic effects, plus jaundice, neutropenia, agranulocytosis, effect glucose tolerance & insulin levels Tetracyclics: Mianserin SE • Report sore throat & flu like symptoms. • Regular blood glucose tests. • May be fatal in O/D Selective Serotonin and NorAdrenaline Reuptake Inhibitors (SNRI) Venlafaxine • Low doses inhibits serotonin • Medium dose inhibits nor-adrenaline • High dose inhibits dopamine • Nor-adrenergic drugs tend to have alerting and energising effects • Wide therapeutic index – tolerability similar to SSRIs • Monitor for elevated blood pressure on high doses Nor-adrenaline Reuptake Inhibitor (NARI) • NARI available in Australia • Reboxetine • Reasonable tolerability – similar to TCAs Enzyme inhibitors • Mono-Amine Oxidase Inhibitors (MAOI) – The first antidepressants discovered • Alternative mechanism for increasing synaptic availability of monoamines. • MAOI & RIMA prevent intracellular destruction of monamines by MAO • MAOI’s available in Australia • Phenelzine • Tranylcypromine MAOI & RIMA prevent intracellular destruction of monamines by MAO Neurotransmitter Re-uptake pump Receptor MAO Dendrite Axon Synapse Presynaptic storage vesicles Side Effects: MAOI’s • Common: as for TCA’s, plus agitation/excess stimulation (do not give dose after 3 p.m.) • Rare but serious: Hypertensive crisis caused by ingesting tryramine containing foods or a drug interaction (cough & cold remedies, nasal drops & sprays, diet pills, pethidine). Side Effects: MAOI’s • Prevention: Follow MAOI diet. Check with Dr before using OTC medication, notify Dr or dentist prior to anaesthetic. • Potential for abuse (amphetamine like properties) • Not well tolerated in > 65y MAOI: Diet • Avoid tyramine containing foods (often in foods requiring aging): banana peel (banana flavouring), broad bean pods, sauerkraut, matured cheeses, aged meats, smoked or pickled fish, vegemite, brewers yeast. MAOI: Diet • Limited quantity: raspberries, avocado, soy sauce, commercial soups, coffee substitutes, wine, port, beer, chocolate. Reversible Inhibitors of MonoAmine Oxidase type A (RIMA) • RIMAs more selective than older MAOIs • Do not cause serious dietary and drug interactions (except at high doses). • Have greater safety & tolerability compared to MAOIs but are not as effective in treatment resistant depression. RIMA available in Australia • Moclobemide - Not effective for OCD Receptor blockers: Antagonists • Noradrenergic and Specific Serotonergic Antidepressant (NaSSA) • Work by completely blocking (antagonist) the serotonin and nor-adrenaline receptors, preventing them from latching on to serotonin and nor-adrenaline (thereby allowing the neurotransmitters to build up). NaSSA available in Australia • Mirtazapine Debate • What effect have SSRIs had on suicidal ideation, attempts and completed suicide? Summary • Lag time 1 – 4/52 before initial response • Newer antidepressants better tolerated, safer in OD (less cardiotoxic) • Caution in switching from 1 to another (drug free intervals) to prevent serotonin syndrome, P450 problems • Continue for adequate time • All anti-depressants can precipitate mania • Increase psychomotor activity before mood elevation (risk suicide) References Carson, V. B., (2000). Mental Health Nursing: The nurse patient journal. (2nd ed.), Philadelphia: W. B. Saunders. Dietz, M. (2000). Managing depression: A consumers view. Australian Health Consumer, 3, 36-37. Fortinash, K. M., & Holoday-Worret, P. A. (2000). Psychiatric mental health nursing ( 2nd ed.). St. Louis: Mosby. Galbraith, A., Bullock, S. & Manias, E. (2001). Fundamentals of pharmacology (3rd ed.). Melbourne: Prentice Hall. Hickie, I. (2000). An approach to managing depression in general practice. Medical Journal of Australia, 173:106-110. Loke, Y. K., Trivedi, A. N., & Singh, S. (2008). Meta-analysis: Gastrointestinal bleeding due to interaction between selective serotonin uptake inhibitors and non-steroidal anti-inflammatory drugs. Alimentary Pharmacology & Therapeutics, 27(1), 31-40. References Mant, A., Rendle, V. A., Hall, W. D., Mitchell, P. B., Montgomery, W. S., McManus, P. R., et al. (2004). Making new choices about antidepressants in Australia: the long view 1975-2002. Medical Journal of Australia, 181(7 Suppl), S21-24. Nash, J., & Nutt, D. (2007). Antidepressants. Psychiatry, 6(7), 289-294. Weitzel, C., & Jiwanlal, S. (2001). The darker side of SSRIs. RN, 64(8), 43-48.