Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dissociative identity disorder wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Conversion disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Child psychopathology wikipedia , lookup
Obsessive–compulsive personality disorder wikipedia , lookup
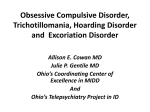
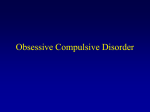
Psychological Assessment 2003, Vol. 15, No. 4, 578 –581 Copyright 2003 by the American Psychological Association, Inc. 1040-3590/03/$12.00 DOI: 10.1037/1040-3590.15.4.578 BRIEF REPORT The Children’s Yale–Brown Obsessive–Compulsive Scale: Item Structure in an Outpatient Setting Dean McKay John Piacentini Fordham University University of California, Los Angeles Scott Greisberg Flemming Graae, Margaret Jaffer, and Jillian Miller Fordham University New York Presbyterian Hospital–Weill Cornell Medical Center Fugen Neziroglu and Jose A. Yaryura-Tobias Bio-Behavioral Institute The Children’s Yale–Brown Obsessive–Compulsive Scale (CY-BOCS) is one of the most popular measures of symptom severity for childhood obsessive– compulsive disorder (OCD). This study describes the factor structure of the CY-BOCS. A total of 233 children diagnosed with OCD were evaluated with the CY-BOCS. The results indicated that 2 alternate 2-factor solutions (obsessions and compulsions; severity and disturbance) fit the data set best. The results also suggested that items assessing resistance to obsessions and compulsions provide unreliable evaluations of these symptoms in children with OCD. Recommendations for modifications to the CY-BOCS as well as clinical applications and for future research with the measure are made. Although the intuitive structure of the Y-BOCS has allowed for a highly structured assessment of symptoms, there have been questions about the construct validity of the subscales and associated total score. In one confirmatory factor analysis of the Y-BOCS (samples; McKay, Danyko, Neziroglu, & YaryuraTobias, 1995), it was found that the total score was not construct valid, but support was found for separate obsessions and compulsions subscales. In a second, larger study (two sets of 202 samples each), separate obsessions and compulsions subscale scores were again supported by a confirmatory factor analysis (Amir, Foa, & Coles, 1997). There was support for the total score, but only when it was considered in isolation, with no additional subscale scores. Further, it was found that the Y-BOCS items form a second two-factor model, with the factors disturbance and symptom severity. On the basis of these findings, McKay, Neziroglu, Stevens, and Yaryura-Tobias (1998) conducted a replication confirmatory factor analysis (with 148 participants). They found that the two different two-factor models (obsessions and compulsions; disturbance and severity) were construct valid but that the total score was not. In all three of these studies, nonsignificant factor loadings were found for the resistance-to-obsessions item. There appears to be ample evidence that the adult Y-BOCS is essentially a two-factor scale without a total score. The Y-BOCS has attracted a great deal of attention and has become a widely used measure of severity because of its intuitive structure and good psychometric qualities (Taylor, 1998). For example, the Y-BOCS has demonstrated good reliability and convergent validity. The CY-BOCS has gained widespread popularity and also has been used in many treatment trials (see, for example, March, Franklin, The Yale–Brown Obsessive–Compulsive Scale (Y-BOCS) (Goodman et al., 1989) has become the most widely used assessment instrument for evaluating the severity of symptoms in obsessive– compulsive disorder (OCD). The severity portion of the scale is composed of 10 items, 5 each for the obsessions and compulsions subscales. The items for each scale are identical, assessing frequency, interference, distress, resistance, and control. Given this intuitive structure and the identical format for the subscales, the authors assumed that the items formed a total score, which has been used to determine cutoff scores for various study protocols for OCD. Further, the intuitive nature of the Y-BOCS has led to a downward age extension for children (Children’s Y-BOCS [CY-BOCS]; Scahill et al., 1997). Dean McKay and Scott Greisberg, Department of Psychology, Fordham University; John Piacentini, Division of Child and Adolescent Psychiatry, University of California, Los Angeles; Flemming Graae, Margaret Jaffer, and Jillian Miller, Childhood OCD/Anxiety Disorders Treatment Program, New York Presbyterian Hospital–Weill Cornell Medical Center, White Plains, New York; Fugen Neziroglu and Jose A. Yaryura-Tobias, BioBehavioral Institute, Great Neck, New York. Portions of these data were presented at the annual meeting of the Anxiety Disorders Association of American, Atlanta, Georgia, March 2001, and at the World Congress of Behavioral and Cognitive Therapies, Vancouver, British Columbia, Canada, July 2001. Correspondence concerning this article should be addressed to Dean McKay, Department of Psychology, Fordham University, 441 East Fordham Road, Bronx, New York 10459-5198. E-mail: mckay@fordham .edu 578 BRIEF REPORT Nelson, & Foa, 2001). The widespread use of the CY-BOCS may be attributed to the extensive use of the adult version as well as the relative absence of other measures of obsessive– compulsive symptoms tailored specifically for children. The CY-BOCS is structured in the same manner as the adult scale but with modified language for direct administration to children 8 to 16 years old. In the one study documenting the psychometric characteristics of the CY-BOCS (Scahill et al., 1997), the total score was found to be significantly correlated with the Leyton Obsessional Inventory (Cooper, 1970; r ⫽ 0.62), with the Children’s Depression Inventory (Kovacs, 1985; r ⫽ 0.34), and with the Revised Children’s Manifest Anxiety Scale (Reynolds & Richmond, 1987; r ⫽ 0.37). The scale is considered appropriate for use with a wide age range (5 to 17 years). This large developmental span may cast some doubt on the utility of the measure, leading to discrepancies in applications. Whereas the adult Y-BOCS relies on interview data from the client, the CY-BOCS culls ratings from both the child and the parent or guardian. Further, the instructions specify that “sometimes, however, it may also be useful to interview the child or parent alone” (from reprinted CY-BOCS in March & Mulle, 1998, p. 219). It is likely that administration will vary by age, with results for younger children being more reliant on informant data than results for older children. Given the popularity of the CY-BOCS and the findings from confirmatory factor analyses with the Y-BOCS, it appears that an investigation of the factor structure of the child measure is warranted. Studies of the factor structure of the adult Y-BOCS have shown that reliance on a total score may be a misrepresentation of symptoms and that two separate scores provide a better description of psychopathology. It is unknown whether the same is true for a sample of children with OCD when evaluated with the CY-BOCS. At present, studies examining childhood OCD and relying on the CY-BOCS as an indicator of severity use the total score as well as the subscales. As noted elsewhere (McKay et al., 1998), in the event that the total score is not representative of symptoms, it is likely to be an underestimate of psychopathology. Therefore, a confirmatory factor analysis was undertaken with the CY-BOCS. We hypothesized that the CY-BOCS would form two different two-factor models, in keeping with the findings of Amir et al. (1997) and McKay et al. (1998). Specifically, we hypothesized model support for obsessions and compulsions and for disturbance and severity. We also hypothesized that there would be no support from the factor analysis for a total score. Method Participants A total of 233 children and adolescents diagnosed with OCD participated. Participants were selected from consecutive eligible referrals to the Childhood OCD/Anxiety Disorders Treatment Program at New York Presbyterian Hospital–Weill Cornell Medical Center (n ⫽ 138), from the UCLA Childhood OCD, Anxiety, and Tourette’s Disorder Program (n ⫽ 65), and from the Bio-Behavioral Institute (n ⫽ 30), a specialty center for the treatment of anxiety disorders. The participants ranged in age from 5 to 17 years (M ⫽ 10.8, SD ⫽ 3.19). The sex distribution was evenly split, with 116 females (49.8%) and 117 males (50.2%). The three sites did not differ in terms of demographic characteristics. All patients met diagnostic criteria set forth in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994) for OCD as their primary diagnosis on the basis of interdisciplinary staff case conferences. 579 Assessment All children were administered the CY-BOCS severity test at the start of behavioral and/or pharmacological treatment. Raters were supervised by M. Jaffer (New York Presbyterian Hospital–Weill Cornell Medical Center), J. Piacentini (UCLA), and F. Neziroglu (Bio-Behavioral Institute). Each of these clinicians has between 10 and 20 years of experience with OCD in general and with children in particular. The ratings used in the present analyses were from baseline assessments, and all ratings were from both child and parent or guardian informants. A subsample (n ⫽ 137) of children were also administered the checklist portion of the CY-BOCS in order to determine primary OCD symptoms for use in the severity ratings. The checklist has been subjected to additional analyses to determine the dimensions of obsessive– compulsive symptoms (McKay et al., 2003). There was no significant difference in severity ratings among the sites (all Fs ⬍ 1.04, p ⫽ ns). Instrument The CY-BOCS is a 10-item clinician-administered scale that represents a total scale as well as two subscales (obsessions and compulsions). Both subscales are identically structured, with five items assessing frequency, distress, interference, resistance, and control over either obsessions or compulsions. Each item is rated from 0 to 4, with higher numbers indicating greater severity of symptoms. Data Analysis The data were analyzed with AMOS 4.0 (Arbuckle, 1999) to examine the hypothesized factor structures. AMOS allows factor structures to be defined, tests for goodness of fit, and determines item–factor loadings and associated level of significance. Results A reliability analysis showed that the CY-BOCS had adequate internal consistency for the obsessions (␣ ⫽ .92) and compulsions (␣ ⫽ .94) subscale scores and for the total score (␣ ⫽ .95) for our sample. Likewise, internal consistency for the severity (␣ ⫽ .88) and disturbance (␣ ⫽ .95) subscale scores was considered adequate. In order to examine the proposed factor structures, the covariance matrix for the 10 primary items was used. The fit indices chosen to provide evidence of model fit were chi-square, adjusted goodness-of-fit index (AGFI; Jöreskog & Sörbom, 1984), root-mean-square residual (RMR; Steiger, 1989), normed fit index (NFI; Bentler & Bonett, 1980), and comparative fit index (CFI; Bentler, 1990). Although the chi-square frequently is used to determine model fit, it is also sensitive to sample size and tends to underestimate adequate model fit (Hayduk, 1987). The AGFI, NFI, and CFI all range from 0 to 1, with scores closer to 1 indicating better model fit. In general, scores for these indices of greater than 0.9 are considered evidence of good model fit. The RMR describes variability not accounted for by the model; scores of less than 0.08 are considered indicative of adequate model fit, and scores of less than 0.05 are considered signs of good model fit (Browne & Cudeck, 1993). Model Testing A null model was tested first to ensure that each item did not form a separate latent variable. This model was found to have inadequate fit, 2(45, N ⫽ 233) ⫽ 381.92, p ⬍ .001. The single- BRIEF REPORT 580 factor model also was found to have poor model fit, 2(21, N ⫽ 233) ⫽ 167.58, p ⬍ .001, as was the two-factor model with a higher-order third factor, 2(38, N ⫽ 233) ⫽ 214.71, p ⬍ .001. These results suggest that the use of the total score, either as a single metric or in the context of the originally proposed subscales of obsessions and compulsions, is not factor analytically sound. When the two-factor model of obsessions and compulsions was tested, it was found to have adequate fit, 2(25, N ⫽ 233) ⫽ 8.61, p ⫽ ns. Likewise, the two-factor model of severity and disturbance also was found to have adequate fit, 2(38, N ⫽ 233) ⫽ 9.12, p ⫽ ns. Table 1 shows the results of these analyses. Individual Item Loadings for Models With Adequate Fit Given that AMOS provides significance values for individual item–factor loadings, in the two-factor model of obsessions and compulsions, only the resistance-to-compulsions and resistanceto-obsessions items had nonsignificant factor loadings for their respective factors (Figure 1). Likewise, in the two-factor model of severity and disturbance, both resistance items had nonsignificant factor loadings for the disturbance factor (Figure 2). Comparisons Between Ages and Sexes The CY-BOCS assesses obsessive– compulsive symptoms across a wide age range. Our sample was split into younger children (less than 11 years old; n ⫽ 101) and older children (11 years old and older; n ⫽ 132), and the covariance matrices for the groups were compared. The results of this analysis showed a nonsignificant difference, Barlett-Box F(1, 232) ⫽ 1.22, p ⫽ ns. Likewise, the covariance matrices for males and females were compared, with similar results, Bartlett-Box F(1, 232) ⫽ 0.77, p ⫽ ns. Discussion The CY-BOCS has become one of the most popular instruments for assessing the severity of obsessive– compulsive symptoms in children. The scale was developed by downward age extension of the original adult scale (Scahill et al., 1997). Although the scale has been popular in clinical trials and direct service delivery settings, the properties of the scale have been underexamined. In this study, we sought to determine the nature of the factor structure of the CY-BOCS for a sample of children diagnosed with OCD. We hypothesized that the CY-BOCS would conform to the factor structures obtained with the adult scale (Amir et al., 1997; McKay Figure 1. Factor structure and item loadings for two-factor solution with obsessions and compulsions. *p ⬍ .05. et al., 1995, 1998). We found support for our hypothesis, namely, that the CY-BOCS is essentially a two-factor scale. The two factors can be defined according to the subscale division of the original scale (obsessions and compulsions) or according to a division based on severity and disturbance. These data suggest that reliance on the total score as an indication of overall severity may underestimate the degree of psychopathology. For example, in the event that a child suffers primarily obsessions, scores on the compulsion subscale would bring the total severity level down and the total score obtained would not be representative of the symptom level. Likewise, a child could have a higher level of disturbance but a lower level of objective severity, so that the total score would not represent the level of distress experienced by the child. In the event that treatment planning were based on the total score, there could be an unintended effect of reduced emphasis on severity level. That is, if treatment were anchored to total scores, then children with primarily obsessions or compulsions might be assumed to have symptoms of lower severity and therefore receive less intensive treatment. As in the earlier factor analyses with the adult scale, the resistance-to-obsessions item had nonsignificant factor loadings for each two-factor model. It was suggested previously (McKay et al., 1995, 1998) that this item is problematic for persons with Table 1 Model Fit Statistics Model 2 df p AGFI RMR NFI CFI Null One-factor Two-factor (obsessions and compulsions) Two-factor (severity and disturbance) Two-factor with higher-order third factor (obsessions, compulsions, and total score) 381.92 167.58 8.61 9.12 45 21 25 12 ⬍.001 ⬍.001 ns ns .27 .54 .97 .93 .39 .43 .05 .06 .66 .77 .98 .97 .62 .73 .96 .94 214.71 38 ⬍.001 .36 .26 .68 .61 Note. AGFI ⫽ adjusted goodness-of-fit index; RMR ⫽ root-mean-square residual; NFI ⫽ normed fit index; CFI ⫽ comparative fit index. BRIEF REPORT Figure 2. Factor structure and item loadings for two-factor solution with disturbance and severity. *p ⬍ .05. OCD, as the way in which patients experience resistance to their symptoms is highly variable. In this study, the ability of children to consistently rate their resistance was low for the items associated with obsessions and with compulsions. Scahill et al. (1997) found low reliability for the resistance items. In that study, it was observed that resistance could be low (leading to a higher score) when symptoms were in fact mild and vice versa. This situation led to low interrater reliability in the CY-BOCS validity study. Therefore, although resistance has been considered an important factor in considering the severity of obsessive– compulsive symptoms (i.e., Rachman & Shafran, 1998), the degree to which the CYBOCS effectively assesses this construct is problematic. It appears from these data that the resistance items require revision in order to reduce the amount of error variability associated with them or that they should be removed and the CY-BOCS severity ratings should be supplemented with a measure of obsessive– compulsive symptoms that assesses cognitive features of the condition. This study is limited by the number of children in the younger group (less than 11 years old) and the number of children of each sex. Although we found that the covariance matrices were not significantly different for symptom severity, it is possible that younger and older children experience different dimensions of symptoms. That is, younger and older children may differ in the extent to which they experience washing or checking symptoms or other dimensions of obsessions or compulsions associated with OCD. Additional study is necessary to determine whether the factor structure for a sample of younger patients is consistent with the adult scale. It is possible that the scale differs fundamentally by age on the basis of the degree to which raters must rely on informants. The same possibility could be plausibly indicated with regard to sex differences. Although the covariance matrices for the severity ratings were not significantly different, the manifestations of symptoms could differ. References American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. 581 Amir, N., Foa, E. B., & Coles, M. E. (1997). Factor structure of the Yale–Brown Obsessive–Compulsive Scale. Psychological Assessment, 9, 312–316. Arbuckle, J. (1999). Analysis of moment structures (Version 4.0). Philadelphia: Temple University. Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238 –246. Bentler, P. M., & Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88, 588 – 606. Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136 –162). Thousand Oaks, CA: Sage. Cooper, J. (1970). The Leyton Obsessional Inventory. Psychological Medicine, 1, 48 – 64. Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., Heninger, G. R., & Charney, D. S. (1989). The Yale–Brown Obsessive–Compulsive Scale: I. Development, use, and reliability. Archives of General Psychiatry, 46, 1006 –1011. Hayduk, L. A. (1987). Structural equation modeling with LISREL: Essentials and advances. Baltimore: Johns Hopkins University Press. Jöreskog, K. G., & Sörbom, D. (1984). LISREL VI user’s guide (3rd ed.). Mooresville, IN: Scientific Software. Kovacs, M. (1985). The Children’s Depression Inventory. Psychopharmacology Bulletin, 21, 995–998. March, J. S., Franklin, M., Nelson, A., & Foa, E. (2001). Cognitivebehavioral psychotherapy for pediatric obsessive– compulsive disorder. Journal of Clinical Child Psychology, 30, 8 –18. March, J. S., & Mulle, K. (1998). OCD in children and adolescents: A cognitive-behavioral treatment manual. New York: Guilford Press. McKay, D., Danyko, S., Neziroglu, F., & Yaryura-Tobias, J. A. (1995). Factor structure of the Yale–Brown Obsessive–Compulsive Scale: A two dimensional measure. Behaviour Research and Therapy, 33, 865– 869. McKay, D., Neziroglu, F., Stevens, K., & Yaryura-Tobias, J. A. (1998). The Yale–Brown Obsessive–Compulsive Scale: Confirmatory factor analytic findings. Journal of Psychopathology and Behavioral Assessment, 20, 265–274. McKay, D., Piacentini, J., Greisberg, S., Graae, F., Jaffer, M., & Miller, J. (2003). The structure of childhood obsessions and compulsions: Subtypes and syndromes. Manuscript submitted for publication. Rachman, S., & Shafran, R. (1998). Cognitive and behavioral features of obsessive– compulsive disorder. In R. P. Swinson, M. M. Antony, S. Rachman, & M. A. Richter (Eds.), Obsessive– compulsive disorder: Theory, research, and treatment (pp. 51–78). New York: Guilford Press. Reynolds, C. R., & Richmond, B. (1987). Revised Children’s Manifest Anxiety Scale (RCMAS) manual. Los Angeles: Western Psychological Services. Scahill, L., Riddle, M. A., McSwiggin-Hardin, M., Ort, S. I., King, R. A., Goodman, W. K., Cicchetti, D., & Leckman, J. F. (1997). Children’s Yale–Brown Obsessive–Compulsive Scale: Reliability and validity. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 844 – 852. Steiger, J. H. (1989). EzPATH: A supplementary module for SYSTAT and SYGRAPH. Evanston, IL: SYSTAT. Taylor, S. (1998). Assessment of obsessive– compulsive disorder. In R. P. Swinson, M. M. Antony, S. Rachman, & M. A. Richter (Eds.), Obsessive– compulsive disorder: Theory, research, and treatment (pp. 229 –257). New York: Guilford Press. Received July 24, 2002 Revision received August 6, 2003 Accepted August 10, 2003 䡲