Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
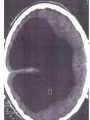
Hva er psykose, hva er psykisk lidelse? • Slagelse, DK, nov 2015 • Jan Olav Johannessen • • • Mental illness and substance use disorders account for 60% of the nonfatal burden of disease amongst young people aged 15-34 (Public Health Group 2005) 75% of mental health problems occur before the age of 25 (Kessler et al 2005) 14% of young people aged 12-17, and 27% of young people aged 18-24 experience a mental health problem in any 12 month period (Sawyer et al 2000, Andrews et al 1999, ABS 2008) Økning i antall uføre ? 12 Hvordan man dypest sett forstår hva psykisk lidelse er, bestemmer både organisering av og innhold i behandlingen” “ Jan Olav Johannessen 13 To viktigste spørsmål som mor stiller: • «Hva er det som feiler gutten min?» • Hvordan kommer det til at gå med gutten min Hva er psykose, hva er psykisk lidelse? • Slagelse, DK, nov 2015 • Jan Olav Johannessen Hva er psykose? Hva er psykisk lidelse? (Når følelser blir lidelse…) 22 23 24 33 38 Psykosen som psykologisk sammenbrudd • Hugdals forskning omkring stemmehøring 42 45 Husk: Psykiske lidelser som dimensjoner Jan Olav Johannessen 46 “An air of desolation more calculated to fix than to remove” Hvordan man dypest sett forstår hva psykisk lidelse er, bestemmer både organisering av og innhold i behandlingen” “ Jan Olav Johannessen 56 The ability to conceptualise what you feel, what you experience Wittgenstein’s duck “An air of desolation more calculated to fix than to remove” Harry Stack Sullivan Forekomst varierer • • • • VOKSE OPP STORBY vs LAND (ikke drift) 8:1 2.generasjons innvandrere 4:1 Etnisitet i byer Menn>Kvinner 6:4 : Resultater • • F20-F29 Mænd Kvinder 3,5 3,5 3 3 2,5 2,5 1,92 1,57 1,21 0,86 2 1,5 1 0,5 2,28 1,84 2 1,5 1,21 1 0,5 2000 2003 2005 2007 2009 2011 2000 2003 2005 2007 2009 2011 0,69 Johanne Olivia Grønne Kühl stud. med PCK 28.05-2015 Det Sundhedsvidenskabelige Fakultet Dias 64 Det sentrale: uheldige livshendelser!! • • • • • Sykdom eller syndrom Gen eller miljø Traumer Uhell Tilfeldigheter Uheldige livshendelser (adverse life events) • Traume Tilfeldighet The impact of trauma in childhood and adulthood on clinical and social functioning in first episode psychosis Stain HJabcd, Joa Id, Larsen TKde, Johannessen JOd, ten Velden Hegelstad Wd, and Langeveld Jd Conclusions While it would appear that trauma in adulthood had a greater impact on functioning in FEP than childhood trauma, it is important to note that childhood trauma increased the risk of experiencing trauma as an adult. The association of trauma with increased negative symptoms and poorer premorbid functioning highlights the need to address trauma in assessment and intervention for FEP. The Myth of Schizophrenia as a Progressive Brain Disease by Zipursky, Reilly & Murray Schizophrenia Bulletin: The Myth of Schizophrenia as a Progressive Brain Disease by Zipursky, Reilly & Murray http://schizophreniabulletin.oxfordjournals.org/content/early/2012/11/20/schbul.sbs135.abstra ct Abstract: Schizophrenia has historically been considered to be a deteriorating disease, a view reinforced by recent MRI findings of progressive brain tissue loss over the early years of illness. On the other hand, the notion that recovery from schizophrenia is possible is increasingly embraced by consumer and family groups. This review critically examines the evidence from longitudinal studies of (1) clinical outcomes, (2) MRI brain volumes, and (3) cognitive functioning. First, the evidence shows that although approximately 25% of people with schizophrenia have a poor long-term outcome, few of these show the incremental loss of function that is characteristic of neurodegenerative illnesses. Second, MRI studies demonstrate subtle developmental abnormalities at first onset of psychosis and then further decreases in brain tissue volumes; however, these latter decreases are explicable by the effects of antipsychotic medication, substance abuse, and other secondary factors. Third, while patients do show cognitive deficits compared with controls, cognitive functioning does not appear to deteriorate over time. The majority of people with schizophrenia have the potential to achieve long-term remission and functional recovery. The fact that some experience deterioration in functioning over time may reflect poor access, or adherence, to treatment, the effects of concurrent conditions, and social and financial impoverishment. Mental health professionals need to join with patients and their families in understanding that schizophrenia is not a malignant disease that inevitably deteriorates over time but rather one from which most people can achieve a substantial degree of recovery. • Is there really such a thing as SCHIZOPHRENIA? Antistigma “With (my patients at Chestnut Lodge) I came upon the scene too late; most of the damage was already done. I remain convinced that with schizophrenia in its moderate to severe form, our current treatment efforts amount to palliation and damage control. There is no doubt that our efforts make a difference, but they effect little if any restitution of what has been lost. For many vulnerable to schizophrenia, the ultimate answer lies in early detection and preventive intervention.” Thomas McGlashan. Editor’s Introduction: Early detection and intervention in schizophrenia, Schizophrenia Bulletin, 1996, 22(2):197-9 The Trauma of Late Intervention Early intervention group Late intervention group THE GRAND DSM V RAILROAD Psychosis Risk Syndrome Bipolar Risk Syndrome Tenacious Depression Syndrome Progression through the prodromal period mania depression mania psychosis Stage 1a mania depression depression psychosis Stage 1b Psychosis schizophrenia Stage 2+ Stages of onset of schizophrenia Stages of decompensation: 0 Equilibrium I Overextension II Restricted consciousness III Disinhibition IV Psychotic disorganisation 1. destructuring of the external world 2. destructuring of the self 3. total fragmentation V Psychotic resolution Docherty 1978 Am J Psychiatry 80 82 bizarre delusions delusions hearing voices suspiciousness isolation problems with concentration anxiety sleeping problems the ”Domino-effect” SIPS Interview Probes Attenuated Psychotic Phenomena PANSS Delusions 7 6 5 4 3 SIPS Unusual Thought Content/Delusional Ideas 6 5 4 Psychosis Threshold 2 3 2 1 1 0 Why study prodromal syndromes and symptoms? • DSM-5 and the “Psychosis risk syndrome”: The need for a broader perspective. Invited editorial , Psychosis, vol 2, no2, june 2010, 93-110 Johannessen/McGorry Psykiske lidelser utvikles i stadier • There has been a growing recognition during the past two decades that mental disorders in general, and psychotic disorders in special, are not static , sharply defined illnesses with separate aethiologies and courses (categories), but rather disorders that develop in stages and overlap (dimensions) (Sullivan 1927,Crow 1990, Docherty 1978, Alanen 1997, Johannessen 2006, McGorry 2006). The idea of phase-specific treatments with its derivative early intervention has grown in almost an explosive manner throughout the last two decades, with the aims of a) reducing or preventing secondary morbidity , and b) achieving primary prevention, i.e prevent the transition from early (prodromal) stages into a fullthreshold psychosis. McGlashan Building of relations (establishing alliances and contacts) No Engagement Alanen Social situation, family situation, individual state of the patient Gunderson Support Relationship Building Renewed therapy meetings Working Alliance Supportive Psycotherapeu tic community Strcuture Communicating Problem Solving Renewed therapy meetings Working Aliance Analytic Internalisation Termination Intermediate phase Therapy of the primary family Relationship Using Fortification Integration Cognitive Enhancement Therapy Family and environmentcentered crisis intervention Attachment Phases of development Basic phase Protection Engagement (Relationship Parameters) Personal Therapy Initial investigation in the first therapy meeting Bonding May be weeks 1-2 years Hogarty Engagement Therapy of the secondary family Advanced Phase Relationship Modifying Individual therapy Validation Recovery phase 91 • Current DSM and ICD systems do not have criteria to define the initial threshold for so-called “caseness”. • The current diagnostic systems define an “end state” syndrome, derived from studying subsets of chronic patients, and thus provides a spurious impression of stability and validity, without considering the complex evolution of symptoms during the onset of a major mental disorder. • A need for a new diagnostic infrastructure for the early stages of mental illness • And: time is running out for the more established concepts such as schizophrenia. • Unfortunately, the DSM V committees have chosen not to evaluate this diagnosis at this point of time. • There is now comprehensive research performed in what has been called “Prodromal stage”, “At risk mental health (ARMS)”, “Ultra high risk (UHR)” “Pre- psychosis” ” Psychosis risk syndrome” • “Prodromes” are by definition retrospective concepts, and all these concepts are connected with serious ethical and stigma aspects that need continuous and careful reflection . • It is deemed unethical and stigmatising to label somebody as “may become psychotic” or “pre-schizophrenia”. • The symptoms in these stages are unspecific, • With low predictive value as to what condition or diagnosis that may be the next stage. • Early stages of bipolar disorders has a similar, or even longer, DUP, and the symptoms being similar to those of non-affective psychosis. (Yung/McGorry 2007). The risk syndrome • For some of these disorders there seems to be an almost indistinguible early stage, or one could hypothesize, a kind of shared early pathway before manifest psychosis occurs. • “The risk syndrome” should not be reserved for the schizophrenia spectre only, but that the scope should be broadened and include bipolar psychoses as well. Pluripotential risk syndrome • A pluripotential risk syndrome that is phenotypically broad and difficult to subtype is perhaps the most useful model. • This model indicates a need for care without attempting to define an end-stage syndrome. • Within the clinical staging framework each stage is in fact a risk syndrome for the next. Advantages: • It will strengthen the dynamic understanding of psychotic disorders, • Support the strategies for early detection and intervention, • It will give new opportunities for developing evidence-based treatments as we will be able to filter out better defined sub-populations of patients, • It will give us a better position in our efforts to understand the evolution of onset of serious mental illnesses. Disadvantages • stigmatising by labelling young people with an “at risk for psychosis” diagnosis is indeed realistic, and has to be answered. • if this new concept will be used as an argument for utterly medicalisation of young people with beginning symptoms of what could develop into a psychosis, • contribute to overmedicalisation of normal humans experiences, • we underline that today’s knowledge-base do not justify that. POP screening prosedures OT el. Outpat. clinics Actual Yes / No 1st episode anxiety or depressive disorder PQ, selreport > cut,off or Therapist Prodr. cheecklist > 2 PANSS=3 item;P1,P2,P 3;P5,P6.A9 Prodrome; ? POP assesment,SIPS 24 hours < 1 week POP inclusion Yes / no Continous treatement 2 years Diagnoser: Gode knagger eller farlige stempler? DIA = GNOSIS = GJENNOM KUNNSKAP 4 A’er • • • • Ambivalens Autisme Affektavflating ??? Diagnoser: Gode knagger eller farlige stempler? Vi stiller alltid en diagnose (også de som ikke stiller diagnoser….) Mennesket har behov for å ordne/kategorisere/sortere Kvinne/mann Ung/gammel levende/død norsk/svensk vestlending/østlending syk/frisk nerver/ikke nerver eller psyke/soma osv, osv F.20.13 Diagnoser: Gode knagger eller farlige stempler? Diagnoser samlebetegnelse • Samlebetegnelse i medisin = hva er galt med mennesket • Samlebetegnelse i bil/maskin = hva er galt med bilen • Samlebetegnelse i samfunnet = hva er galt i samfunnet • Knyttet til stigma/antistigma = samlebetegnelse på ”grupper” Lars Thorgaard (LTH 3-R) Schizofreni er: • • • • • • • A separation/attachment disorder Distrust/loss of trust disorder A relation disorder An identity disorder A paroxysmal and relapse disorder A control and loss of control disorder A selfcare-failing disorder Diagnoser: Gode knagger eller farlige stempler? Diagnoser: ICD10/DSM IV • nyttige • uunngåelige • Vite hva vi gjør Behandlingsresultat, hvorfor er det ingen som spør? • ER der noen der blir goe’ • Lokalpolitiker, 1986 115 116 117 I S - FORELØPIG Utredning, behandling og oppfølging av personer med psykoselidelser Utkast til endelig versjon 2.11.2012 Hovedgrep Nasjonale retningslinjer • • • • • • Fasespesifikk tilnærming Dimensjonell psykoseforståelse Behovstilpasset behandling Standardisert ”Utrednings- og behandlingslinje” Helhetlig perspektiv Behandlingsresultat-perspektiv 119 Remisjon og recovery % Kontroll Tidlig oppdagelse Odds ratio Remisjon 46.6 52.5 1.3 Recovery* 12 31 2.5 *p<.017 GLOBAL MENTAL HEALTH CAMPAIGN STRATEGY #101 Early Intervention! No way! WPA Maybe Later? THE CAMPAIGN FOR GLOBAL MENTAL HEALTH THE LANCET’S Dr Richard Horton