Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
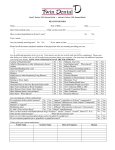
Completed by: Self llan deilo Guardian Parent dental practice Patient’s Signature: Date: / / Dentist’s Signature: Date: / / Electronic Privacy The practice regularly communicates with its patients by email and texts to confirm appointments and costs of treatment. For you to benefit from receiving these communications, we require your permission. If you choose not to agree, you will not receive emails or texts from us. Confidential Medical History Form We ask you for information about your general health to help us treat you safely. Please write your contact details below, answer the health questions inside then sign the form on the back page. We will use this form at later visits to discuss any change in your general health. All information will be kept strictly confidential by the people caring for you. Surname: First Name/s: We will not pass on your contact details to third parties, We will also not send any information regarded as personal - for example, information about treatments and plans. Title: I agree that Llandeilo Dental Practice may use my email address and mobile phone number to contact me regarding appointments and related information. Such communications may include information relating to products and services of the practice. I understand that I can opt out from receiving these communications at any time. Address: Patient’s Signature: Date: llan deilo dental practice / / Sex: Male Date of Birth: / / Postcode: Home Telephone: Mobile: Emergency Contact: Name: Number: E-mail: Occupation: Doctors Name & Address: Doctor’s Telephone: Female Are you currently: Receiving treatment from a doctor, hospital or clinic? Yes No Give Details Taking any prescribed medicines (eg, tablets, ointments, injections or inhalers, including contraceptives and hormone replacement therapy)? Carrying a medical warning card? Pregnant or possibly pregnant? Alcohol: How many units of alcohol do you drink per week? Have you ever suffered from: Allergies to medicines (eg. Penicillin), substances (eg. Latex) or foods? Bronchitis, asthma or other chest conditions? Fainting attacks, giddiness, blackouts or epilepsy? Heart problems, angina, blood pressure problems or stroke? Heart Surgery? Bone or joint disease? Bruising or persistent bleeding following injury, tooth extraction or surgery? Any other serious illness or infectious disease? Liver disease (eg. Jaundice, hepatitis) or kidney disease? Blood refused by the Blood Transfusion Service? A bad reaction to general or local anaesthetic? Treatment that required you to be in hospital? Diabetes (or does anyone in your family)? Yes No Give Details (A unit is half a pint of lager, a single measure of spirits or a small glass of wine/aperitif) units per week Tobacco use: Do you smoke any tobacco products now or in the past? Yes No In the Past times per day Do you chew tobacco, pan, use gutkha or supari now or in the past? times per day Please give any other details which your dentist might need to know, such as self-prescribed medicines (eg. Aspirin) or any disabilities.