Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
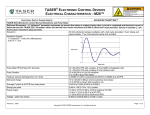
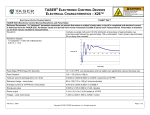
Comparative Analysis of Three Projectile Stun Guns By: Wayne McDaniel, Ph.D. Purpose: To compare the output of three commercial projectile stun guns, the Taser M26, Taser X26, and Stinger S200. These devices were compared by applying the stun guns to a resistive load, and also by applying the stun guns to a live, human-sized animal. Background: Electronic stun guns were originally developed as hand-held weapons with two electrodes on the end, which would be held against the subject to directly apply the electric shock. Projectile stun guns (PSGs) have extended the range of application of these stun guns, by shooting two barbed electrodes to the subject, which trail wires back to the device to conduct the electricity from the device to the subject. The maximum range of PSGs is now about 20 to 22 feet. Presently available PSGs include the Taser M26 and the Taser X26 (Taser International, Scottsdale, AZ), and the Stinger S200 (Stinger Systems, Tampa, FL). Field use of PSGs typically involves shooting the barbed electrodes towards the torso of the subject to be subdued. These barbed electrodes either stick into the skin of the subject, or more likely stick into the clothing of the subject and the electricity arcs through the clothing to the skin. Frequently one or both of the electrodes strike the thorax of the subject. Any application of electricity to the thorax raises the concern that the electrical stimulation will induce ventricular fibrillation (VF) in the subject, which is a potentially lethal cardiac arrhythmia. These devices have been shown to be capable of incapacitating humans, but they do so with very different electrical waveforms and shock amplitude (See figs 1-3). The goal of this study was to characterize the output of these three PSGs in both a resistive model and an animal model. Figs. 1, 2, 3. Output waveforms of the Taser M26, Taser X26, and Stinger S200. In each projectile stun gun, the waveform shown is repeated 15-19 times per second. [Note different time and amplitude scales in these figures] Literature Review: The first modern PSG was the Taser M26, and this device was therefore the first to be studied in an animal model. This device was tested in a canine model and was found to not induce VF in 192 applications, when the darts were applied to various locations on the chest and abdomen [McDaniel et al, 2000]. The Taser X26 was tested in a porcine model with animals having a range of body weights. In this study, the electrical output could be increased up to 50 times the output charge of the normal X26, and the electrical output was increased in each animal until VF was observed. A safety factor was then estimated for each animal, which was found to be weight dependent, ranging from 15X to 42X the normal X26 output, as the animal weight ranged from 30 to 117 kg. [McDaniel et al, 2004]. Our conclusion from these two studies was that the initiation of VF by the commercial devices would be a rare event. The Taser devices have now been applied to humans over 600,000 times, without an observed episode of inducing VF [Upson, 2007]. However, there have also now been more than 250 deaths of subjects, after having received one or more shocks from either the Taser M26 or the Taser X26 [Walter et al, 2008]. The number of these deaths has caused some to question the safety of these devices, and has motivated many investigators to study these devices more thoroughly. There have been several published studies of the application of Taser devices in healthy, human volunteers. These studies have looked at various cardiovascular and physiologic parameters [Ho et al, 2006] and have not documented any changes that would provide a causal link between exposure to the Taser device and death [Ho et al, 2007]. However, there have been other studies that have found that the Taser devices consistently pace the heart of experimental animals, and that they can induce VF in experimental animals under certain conditions. One study in pigs found that when the Taser X26 was applied to the chest for either 5 or 15 seconds, it capture paced the heart in 98% of the shocks. When the Taser M26 was applied to the chest, it captured the heart in 54% of the shocks. The mean heart rate during stimulation and capture was 324 beats/min [Nanthakumar, 2006]. Another study of the Taser X26 in pigs gave two 40 second exposures. Two deaths were observed in this group of animals from acute onset VF. No cardiac capture data was available, as they were not able to observe the cardiac rhythm during the X26 applications, due to device limitations [Dennis, 2007]. Another study of the Taser X26 also gave a protocol of two 40 second exposures, and followed the animals for 48 hours after the exposure. They found cardiac capture pacing in all experimental animals, with a rate of 301 beats/min. The cardiac rhythm of one of these experimental animals degenerated into VF [Walter et al, 2008]. Another study of the Taser X26 looked at the dart to heart distance that could induce VF. They found an average distance of 17 mm for the first induction of VF, and an average distance of 13.7 mm for successive VF events. They observed a higher frequency of VF when the dart to heart distance was smaller. The authors interpreted their data as indicating that the current density at the heart needed to be a certain level to induce VF. By increasing the dart to heart distance, the current density at the heart decreased, and VF was less likely. They further report skin to heart distances in humans of 10 to 57 mm, as measured by echocardiography [Wu et al, 2006]. These studies just described, which demonstrated cardiac pacing and the induction of VF with thoracic application of Tasers, were performed in animal models. Recently, a case study detailed a human subject with a pacemaker who was subjected to a Taser discharge. The internal memory of the pacemaker recorded two high ventricular rate episodes, which corresponded to the Taser application. The authors interpreted this as demonstrating myocardial capture pacing in humans [Cao et al, 2007]. Finally, there has been one published case report of VF being documented shortly after Taser application in a human subject. The authors interpreted the VF as having been induced by the Taser [Kim et al, 2005]. Another consideration of the use of these devices relates to physiological changes brought about by extended duration near-maximal muscle contractions. One study applied the Taser X26 repeatedly for 5 seconds on and 5 seconds off, which was repeated for 3 minutes. They found the blood pH was significantly decreased for 1 hour following exposure, and that the lactate level was highly elevated [Jauchem, 2007]. This study demonstrated another consideration to repeated use of the Taser devices. It is possible that the cause of the deaths after Taser application will be multi-factorial, and could include a combination of drug use, compromised physiological status, and cardiac stimulation. The Stinger S200 is the latest PSG to enter the market, and it generates the radically different waveform shown in Fig. 3. A safety study has now been completed of the S200, and this study has been accepted for presentation and publication [McDaniel, 2008]. This study confirmed the experience in human subjects, wherein the S200 has been applied to several thousand subjects with no observation of ventricular fibrillation or ventricular tachycardia. This literature review found studies that indicate cardiac stimulation and capture pacing is possible with the application of the Taser devices in both experimental animals and humans. These studies further indicate that the shock intensity, in particular the current density at the heart, and the manner in which the current varies with time, are important determinants of the ability to stimulate and pace the heart. Finally, they indicate that physiological changes may also accompany prolonged exposure to these Taser devices. Further research will be required to fully understand the mechanism of death after the application of a projectile stun gun. However, it appears that achieving neuromuscular incapacitation with the smallest electrical shock is very desirable. Here we performed two studies to characterize the output of these projectile stun guns, one with a resistive load, and one with a human-sized pig. Study 1 The objective of this study was to evaluate the output of the 3 projectile stun guns with a resistive load. METHODS In this study, the three PSGs were applied to a 430 ohm non-inductive resistor. The voltage across the resistor and the current through the resistor were captured on a digital oscilloscope with the use of high voltage probes and an inductive current probe (Model 2877, Pearson Electronics, Palo Alto, CA). From these tracings, the other electrical parameters were measured and/or calculated. RESULTS The electrical parameters observed when the PSGs were applied to the resistive load are shown in the following table. We used published values for the pulse repetition frequency in our calculations, due to possible variation with battery status. Energy per pulse (J) Power (W) Current – pk (A) Current – rms (mA) Voltage – pk (V) Votage – rms (V) Taser M26 0.565 10 15.6 153 6,320 63 Taser X26 0.084 1.59 4.0 61 1,520 26.2 Stinger S200 0.053 0.92 2.14 47 864 19.7 DISCUSSION Our study found that the Stinger S200 delivered substantially less of each of the relevant electrical parameters than either the Taser X26 or the Taser M26. For example, the S200 delivered 63% of the energy/pulse of the X26, and less than 10% of the energy/pulse of the M26. The X26 delivered a peak current almost twice that of the S200, and the M26 delivered a peak current more than 7 times that of the S200. Perhaps the best descriptor of current delivered by PSGs is rms current, and the X26 delivered an rms current 30% higher than the S200, while the M26 delivered an rms current more than 3 times that of the S200. CONCLUSIONS The Stinger S200 was found to deliver less energy, power, current, and voltage than both the Taser M26 and X26 when applied to a resistive load. The Taser X26 was also found to deliver less energy, power, current, and voltage than the Taser M26 when applied to the same resistive load. By delivering less of each of the relevant electrical parameters, the S200 could have a larger safety margin for the induction of VF than the Taser devices. This will need to be tested in future studies. Study #2 This study was performed to characterize the electrical current that flows when three commercial projectile stun guns were applied to the thorax and abdomen of a pig, in three different orientations of the darts. METHODS A 72 kg pig was anesthetized and placed in dorsal recumbency on an insulated table. The darts from the stun gun being studied were applied in each of the following orientations: Side to Side across the heart (S-S), Sternal Notch to Xiphoid (SN-X), and Sternal Notch to Umbilicus (SN-Umb). One of the probes from the stun gun was fed through an inductive current probe (Model 2877, Pearson Electronics, Palo Alto, CA), which was then connected to a digital oscilloscope (Model 3014B, Tektronix, Beaverton, OR). Each stun gun was applied to the pig in each of the three orientations, while recording the current waveform that actually flowed into the pig. The peak current and rms current were then measured and/or calculated. RESULTS - Measured and calculated current values are shown in the table below. Device Stinger S-200 Stinger S-200 Stinger S-200 Taser X-26 Taser X-26 Taser X-26 Taser M-26 Taser M-26 Taser M-26 Orientation S-S SN-X SN-Umb S-S SN-X SN-Umb S-S SN-X SN-Umb Peak Current (A) 1.96 1.88 2.12 3.48 3.40 3.64 14.6 15.3 15.3 RMS Current (mA) 43.1 40.1 40.5 51.2 56.7 53.3 147 137 145 Probe orientation abbreviations: S-S Side to side across heart SN-X Sternal notch to Xiphoid SN-Umb Sternal notch to Umbilicus We used the following published values for the repetition frequency of each stun gun in our calculations, due to possible variation with battery status: S-200 17.5 pulse groups per second X-26 19 pulses per second M-26 17 pulses per second The peak current of the X-26 was approximately 75% higher than the peak current of the S-200. The peak current of the M-26 was approximately 7 times the peak current of the S-200, and 5 times the peak current of the X26. The rms current delivered by the X-26 was approximately 28% higher than the rms current delivered by the S-200. The rms current delivered by the M-26 was more than 3 times the rms current delivered by the S-200 and about 2.5 times the rms current delivered by the X26. DISCUSSION Projectile stun guns apply high voltage, pulsatile shocks to the thorax of subjects, which raises concerns about the induction of ventricular fibrillation. The critical electrical parameter that could actually induce ventricular fibrillation is the electrical current that flows from the stun gun into the subject. The present study characterized the current that flows into the subject during actual application of the projectile stun guns to a human-sized pig. Here we characterized this current in two different ways. We found that the Stinger S200 delivers appreciably less peak current and rms current than both the Taser X-26 and the Taser M-26, and the X-26 delivers appreciably less peak current and rms current than the M-26. CONCLUSIONS The current delivered by three commercial projectile stun guns into a pig model was characterized. We found that the Stinger S-200 delivered less peak and rms current than the Taser X-26 and the Taser M-26. We further found that the Taser X-26 delivers less peak and rms current than the Taser M-26. Further studies will be necessary to test whether delivering lower peak and rms current translates into a reduced ability to pace the heart and whether the device that generates the lowest peak and rms current proves to be the safest device. ANALYSIS The Taser M26 and Taser X26 have now been applied to over 600,000 human subjects without an observed episode of initiating ventricular fibrillation. However, there have now been over 250 deaths associated with the application of one of these Taser devices. There have been several studies of Taser device application in human volunteers that have failed to demonstrate a causal link between the Taser application and death. However, there have been several studies of the Taser M26 and the Taser X26 in experimental animals, which have demonstrated the ability of these devices to capture pace the heart and to induce ventricular fibrillation. There has also now been one published case report of a Taser capture pacing in a human, and another case report documenting VF shortly after a Taser application. There is a general consensus among those that work in this area, that the electrical current density at the heart is the most important electrical parameter to quantify the ability to pace the heart and to induce VF. Measuring the current density at the heart represents a very difficult technical challenge, but we were able to measure the current that was delivered to the chest. The present report has characterized the output of the 3 commercial projectile stun guns in two different studies. The first study demonstrated that the Stinger S200 delivers less energy, power, current, and voltage than both of the Taser devices. The second study found that the S200 delivers less peak and rms current than either of the Taser devices, when the devices were applied to the torso of a human-sized pig. This data suggests that the S200 will be less likely to pace capture the heart and less likely to induce VF. Further studies will be necessary to test whether it is in fact a safer stun gun than the Taser devices. References: 1. McDaniel WC, Stratbucker RA, Smith RW: Surface application of Taser stun guns does not cause ventricular fibrillation in canines. Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2000. 2. McDaniel WC, Stratbucker RA, Nerheim M, et al: Cardiac safety of neuromuscular incapacitating defensive devices. PACE 2005; 28:S284-287. 3. Upson S: How a Taser works. IEEE Spectrum, December, 2007, p.23-27. 4. Walter RJ, Dennis AJ, Valentino DJ, et al: Taser X26 discharges in swine produce potentially fatal ventricular arrhythmias. Acad Emerg Med 2008; 15:66-73. 5. Ho JD, Miner JR, Lakireddy DR, et al: Cardiovascular and physiologic effects of conducted electrical weapon discharge in resting adults. Acad Emerg Med 2006; 13:589-95. 6. Ho JD, Dawes DM, Bultman LL, et al: Respiratory effect of prolonged electrical weapon application on human volunteers. Acad Emerg Med 2007; 14:197-201. 7. Nanthakumar K, Billingsley IM, Masse S, et al: Cardiac electrophysiological consequences of neuromuscular incapacitating device discharges. J Am Coll Cardiol 2006; 48:798-804. 8. Dennis AJ, Valentino DJ, Walter RJ, et al: Acute effects of Taser X26 discharges in a swine model. J Trauma 2007; 63:581-590. 9. Wu J-Y, Sun H, O’Rourke AP, et al: Dart-to-heart distance when Taser causes ventricular fibrillation in pigs. IFMBE Proc., 2006; 15: 578-583. 10. Cao M, Shinbane JS, Gillberg JM, et al: Taser-induced rapid ventricular myocardial capture demonstrated by pacemaker instracardiac electrograms. J Cardiovasc. Eectrophysiol. 2007; 18:876-9. 11. Kim PJ, Franklin WH: Ventricular fibrillation after stun-gun discharge. N Engl J Med. 2005; 353:958-9. 12. Jauchem JR, Sherry CJ, Fines DA, et al: Acidosis, lactate, electrolytes, muscle enzymes, and other factors in the blood of Sus scrofa following repeated TASER exposures. Forensic Sci International 2006; 161:20-30. 13. McDaniel WC: Cardiac Safety of the Surface Application of the Stinger S-200, (accepted for presentation and publication), 2008. Wayne McDaniel, Ph.D. Ph.D. – Electrical Engineering (Bioengineering emphasis) Presently – Adjunct Associate Professor of Electrical & Computer Engineering at the University of Missouri - Columbia Over 20 years experience performing research related to electricity and the heart, primarily related to electrical defibrillation of the heart. Performed the first animal study of the Taser M26 in 1999 PI of the animal portion of the testing of the Taser X26 in 2003 Frequent presenter on the subject of the cardiac safety of stun guns Author and co-author of multiple articles related to the cardiac safety of stun guns Representative Publications: 1. McDaniel WC, Stratbucker RA, Smith RW: Surface application of Taser stun guns does not cause ventricular fibrillation in canines. Proceedings: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2000. 2. McDaniel WC, Nerheim M, Stratbucker R: Assessing the Cardiac Rhythm Safety of Thoracic Application of Tasers. Europace, 6(Suppl. 1):96, 2004. 3. McDaniel WC, Stratbucker R, Nerheim M, Brewer J: Cardiac Safety of Neuromuscular Incapacitating Defensive Devices. PACE 28:S284-S287, 2005. 4. Stratbucker RA, Kroll MW, McDaniel WC, Panescu D, Cardiac Current Density Distribution by Electrical Pulses from TASER devices, Proc. 28th IEEE EMBS Intl. Conf., New York, August-September 2006. 5. McDaniel WC, Stratbucker RA: Testing the Cardiac Rhythm Safety of the Thoracic Application of TASER Devices. Europace, 8(Suppl 1):58P/23, 2006. 6. Panescu D, Kroll MW, McDaniel W, Stratbucker RA: Cardiac Current Density Distribution by Electrical Pulses from TASER Devices, Conf Proc IEEE Eng Med Biol Soc. 1(1):6305-6307, 2006.