Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Echocardiography wikipedia , lookup
Artificial heart valve wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Atrial septal defect wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
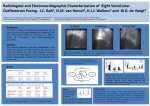
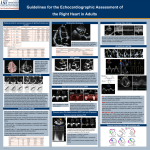
Echo Rounds Infundibular Pulmonary Stenosis Viji Kurup, MD* Albert Perrino, Jr., MD* Paul Barash, MD* Sabet W. Hashim, MD† A 63-yr-old patient presented with a preoperative diagnosis of aortic stenosis and pulmonary stenosis for aortic valve (AV) replacement and possible pulmonary valve (PV) repair. His symptoms included chest heaviness and shortness of breath. A preoperative transthoracic echocardiogram demonstrated calcified tri-leaflet AV with severe stenosis and a peak pulmonic flow velocity of 3.7 m/s. Cardiac catheterization confirmed these findings with a right ventricular (RV) pressure of 71/⫺3 mm Hg, pulmonary artery (PA) pressure of 26/11 mm Hg and a peak pulmonic gradient of 45 mm Hg. Intraoperative transesophageal echocardiography (TEE) was performed and the PV was interrogated in several planes. The midesophageal (ME) RV inflow–outflow view was suboptimal due to shadowing from the calcified AV. Similarly, the ME AV short axis (SAX) view was obtained and the probe was gradually withdrawn to image the PA. This view was inadequate because of bronchial interference. Subsequently, the upper esophageal aortic arch SAX view was obtained and the PV visualized. The leaflets were mobile with normal morphology. Continuous wave Doppler interrogation revealed a maximum velocity of 3.2 m/s (peak gradient of 40 mm Hg) (Fig. 1). The RV function was assessed to be normal. To better define the etiology of the gradient, the probe was advanced to the transgastric (TG) midpapillary level, turned rightward and the multiplane angle rotated to 125° to obtain the TG RV inflow–outflow view (1). Gain settings and focus were adjusted to optimize image acquisition. This view revealed a normal appearing PV and a thickened infundibular septum bulging into the RV outflow tract (RVOT) (Echo Clip 1). These findings, consistent with subpulmonic stenosis, altered the surgical This article has supplementary material on the Web site: www.anesthesia-analgesia.org. From the *Department of Anesthesiology; and †Section of Cardiothoracic Surgery, Yale University School of Medicine, New Haven, Connecticut. Accepted for publication November 21, 2006. Address correspondence and reprint requests to Viji Kurup, MD, Department of Anesthesiology, Tompkins-3, Yale University School of Medicine, 333 Cedar St., New Haven, CT 06510. Address e-mail to [email protected]. Copyright © 2007 International Anesthesia Research Society DOI: 10.1213/01.ane.0000255204.39328.0b Vol. 104, No. 3, March 2007 plan from valve repair to pulmonary arteriotomy and examination of the RVOT and infundibular myomectomy. After institution of cardiopulmonary bypass and AV replacement, the main PA was incised, revealing a normal PV and bulging of the interventricular septum into the RVOT. Other conditions that could mimic RVOT obstruction such as aneurysm of the membranous interventricular septum and mass lesions in the RVOT were excluded by inspection. A septal myomectomy of the RVOT was performed. (Fig. 2) Postcardiopulmonary bypass, Doppler interrogation in the TG RV inflow–outflow view documented velocities of 2.39 m/s (peak pressure gradient 22 mm Hg). The pathology report on the excised septum noted cardiac myocyte hypertrophy and interstitial fibrosis. The patient’s postoperative course was uneventful. On postoperative day 13, a transthoracic echocardiogram showed peak RVOT/pulmonic velocities of 1.55 m/s (peak gradient 9.6 mm Hg). Isolated infundibular pulmonic stenosis is an uncommon cardiac abnormality, with a reported incidence of 0.4% (2) of patients with congenital heart disease. Novel methods of decreasing pulmonary gradient with DDD pacing have been described in the literature (3). The views used in a standard TEE examination may not provide detailed morphologic and hemodynamic assessment of the RVOT and PA. The ME RV inflow– outflow view is useful to examine the morphology of the RVOT. However, the RVOT flow is perpendicular to the interrogating Doppler beam used to estimate velocities. Further, shadowing from a calcific AV can obscure the RVOT. In this case, the upper esophageal aortic arch SAX view demonstrated a morphologically normal PV, but we were not able to visualize the RVOT. An alternative approach to visualizing right heart structures is the TG RV inflow– outflow view. From the TG left ventricular midpapillary SAX view, the probe is turned rightward and the imaging array rotated to 110°–140° to obtain a view of the right atrium, tricuspid valve as well as the RVOT and PV (Clip 2). (1) Using this approach, the TEE examination demonstrated a normal appearing PV with protrusion of the septum into the RVOT, and facilitated the diagnosis of infundibular pulmonary stenosis. Other conditions causing RVOT obstruction are 507 Figure 1. Prebypass upper esophageal aortic arch short axis view with schematic representation of the view. Continuous wave doppler interrogation of right ventricular outflow tract (RVOT)/PA reveals maximum velocity of 3.19 m/s with peak gradient of 40 mm Hg. Figure 2. Post resection transgastric right ventricular inflow-outflow view showing area of resection. Schematic representation of the view showing right atrium (RA), right ventricle (RV), pulmonary artery (PA), pulmonary valve (PV), and aorta (Ao). protrusion of right sinus of Valsalva into the RVOT, aneurysm of membranous ventricular septum, and intra and extracardiac mass lesions in the RVOT such as sarcoma. Congenital conditions such as Tetralogy of Fallot may also be associated with this condition, and search for other components should be conducted. This report demonstrates the value of a comprehensive examination of the right heart to identify an uncommon abnormality and guide surgical management. 508 Infundibular Pulmonary Stenosis REFERENCES 1. Sreeram GM, Mark MJ. Right ventricle, right atrium, tricuspid valve, and pulmonic valve. In: Perrino R, ed. A practical approach to transesophageal echo cardiography. Philadelphia: Lippincott Williams & Wilkins, 2003:227. 2. Shyu KG, Tseng CD, Chiu IS, et al. Infundibular pulmonic stenosis with intact ventricular septum: a report of 15 surgically corrected patients. Int Cardiol 1993;41:115–21. 3. Angelkov L Trajic S, Popovic Z, et al. Acute effects of DDD pacing in patients with pulmonary infundibular stenosis. Am J Cardiol 1999;84:117–18. ANESTHESIA & ANALGESIA