Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
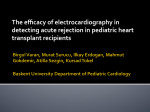
Coronary Interventions Optical Coherence Tomographic Evaluation of Transplant Coronary Artery Vasculopathy With Correlation to Cellular Rejection Liang Dong, MD; Akiko Maehara, MD; Tamim M. Nazif, MD; Ari T. Pollack, MD; Shigeo Saito, MD; LeRoy E. Rabbani, MD; Mark A. Apfelbaum, MD; Kate Dalton, MS, RD; Jeffrey W. Moses, MD; Ulrich P. Jorde, MD; Ke Xu, PhD; Gary S. Mintz, MD; Donna M. Mancini, MD; Giora Weisz, MD Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 Background—Cardiac allograft vasculopathy is an accelerated fibroproliferative process that affects the coronary arteries of transplanted hearts. Intracoronary imaging with optical coherence tomography enables detection of subangiographic cardiac allograft vasculopathy. Methods and Results—At the time of routine surveillance coronary angiography, 48 consecutive heart transplant recipients underwent optical coherence tomographic imaging of 1 coronary artery. Imaging findings were compared per rejection history that was graded according to the International Society of Heart and Lung Transplantation classification as none/ mild (International Society of Heart and Lung Transplantation 0, 1A/1B, or 2) or high-grade rejection (≥3A). Compared with the none/mild rejection group (37 patients) using Mann–Whitney U test, patients in the high-grade rejection group (11 patients) had a thicker intima in all coronary segments (distal: 0.22 mm [0.09–0.41] versus 0.09 mm [0.06–0.17], P=0.02; middle: 0.35 mm [0.00–0.45] versus 0.14 mm [0.08–0.24], P=0.002; and proximal: 0.34 mm [0.21–0.44] versus 0.15 mm [0.11–0.21], P=0.005) and a higher prevalence of foamy macrophages (distal: 55% versus 9%, P=0.003; middle: 55% versus 22%, P=0.004; and proximal: 44% versus 13%, P=0.05) using χ2 statistics. Side branches in the high-grade rejection group had smaller lumen diameters and a higher prevalence of intimal thickening (54% versus 36%; P=0.01). Intimal microvessels were also more prevalent in the high-grade rejection group versus the none/mild rejection group (46% versus 11%; P=0.02). Conclusions—Coronary optical coherence tomographic evaluation revealed that patients with a history of high-grade cellular rejection, compared with those with none/mild rejection, had more coronary artery intimal thickening with macrophage infiltration, involving all coronary segments and side branches. Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT01403142. (Circ Cardiovasc Interv. 2014;7:00-00.) Key Words: heart transplantation ◼ tomography, optical coherence C symptoms, early diagnosis and surveillance of CAV remain important clinical challenges.2 Optical coherence tomography (OCT) provides high-resolution (10–20 μm) intravascular imaging in vivo and has been used to visualize and characterize coronary atherosclerotic plaque composition.3 The current study used OCT to identify CAV disease patterns and to investigate the relationship to prior acute cellular rejection. ardiac allograft vasculopathy (CAV) is a unique form of accelerated coronary artery disease that is a major cause of morbidity and mortality in heart transplant recipients, especially those who survive beyond the first year after transplantation.1,2 The pathophysiology of CAV involves immunologic and nonimmunologic factors that cause localized inflammation with persistent vascular injury and endothelial dysfunction. Despite improvements in immunotherapy, the incidence of angiographically detected CAV has not changed appreciably during the past 2 decades, and limited progress has been made in characterizing this disease process. Emerging evidence now suggests that alterations in medical therapy may interrupt the progression of CAV. Because of the absence of typical ischemic Methods Study Population The analysis included 48 consecutive heart transplant recipients who underwent routine surveillance coronary angiography between February 2011 to December 2012. These patients underwent Received July 11, 2013; accepted March 6, 2014. From the NewYork Presbyterian Hospital, Columbia University Medical Center, New York, NY (L.D., A.M., T.M.N., A.T.P., S.S., L.E.R., M.A.A., K.D., J.W.M., U.P.J., D.M.M., G.W.); the Cardiovascular Research Foundation, New York, NY (L.D., A.M., S.S., J.W.M., K.X., G.S.M., G.W.); The Second Affiliated Hospital, Zhejiang University School of Medicine, Zhejiang, China (L.D.); and Shaare Zedek Medical Center, Jerusalem, Israel (G.W.). Correspondence to Giora Weisz, MD, Department of Cardiology, Shaare Zedek Medical Center, 12 Shmuel (Hans) Beyth St, Jerusalem 91031, Israel. E-mail [email protected] © 2014 American Heart Association, Inc. Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org 1 DOI: 10.1161/CIRCINTERVENTIONS.113.000949 2 Circ Cardiovasc Interv April 2014 Table 1. Rejection Grade and Groups What Is Known • Pathological reports showed that cardiac allograft vasculopathy is a diffuse, accelerated fibroproliferative process that affects the coronary arteries of transplanted hearts. • Previous intravascular ultrasound studies of cardiac allograft vasculopathy showed intimal thickening with advanced morphological changes. What the Study Adds • Intracoronary Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 imaging with optical coherence tomography enables detection of cardiac allograft vasculopathy more clearly both quantitatively and qualitatively. • Coronary optical coherence tomography revealed that patients with a history of high-grade cellular rejection, compared with those with no/mild rejection, had more coronary artery intimal thickening with macrophage infiltration involving all coronary segments, as well as side branches. orthotopic cardiac transplantation at Columbia University Medical Center (New York, NY) between January 1996 and August 2011 and were followed for acute cellular rejection by serial right ventricular endomyocardial biopsies. The study was approved by the institutional review board, and all patients gave written informed consent. Classification of Transplant Cellar Rejection All patients underwent serial right ventricular endomyocardial biopsies according to institutional protocol and clinical needs. The presence of acute cellular rejection was graded according to the International Society of Heart and Lung Transplantation (ISHLT) classification proposed in 1990: grade 1A, focal, mild acute rejection; grade 1B, diffuse, mild acute rejection; grade 2, focal, moderate acute rejection; grade 3A, multifocal, moderate rejection; grade 3B, diffuse, borderline severe acute rejection; and grade 4, severe acute rejection. In consideration of the updated classification proposed in 2005, we categorized tissue as showing none/mild rejection (ISHLT 0, 1A/1B, or 2) or high-grade rejection (≥3A; Table 1).4 Rejection grade was chosen as the worst grade per patient recorded since transplantation. Quantitative Coronary Angiographic Analysis Angiographic analysis was done using QAngio XA version 7.2.34.0 (Medis Medical Imaging Systems, Leiden, The Netherlands) blinded to the OCT findings. After guiding catheter calibration, proximal, mid, and distal coronary artery segments were identified that corresponded to the areas of OCT analysis, and the minimal lumen diameter in each segment was measured. Qualitative analysis included side branch narrowing, lumen irregularity, and calcium.5 OCT Imaging, Definitions, and Analysis After diagnostic coronary angiography, patients received intravenous coronary heparin and nitroglycerin (100 μg). A 2.7F OCT imaging catheter (C7 Dragonfly, St Jude Medical, St Paul, MN) was advanced over an angioplasty guidewire into a target vessel. The target vessel was either (1) the vessel showing the most severe disease or irregularities on angiography or (2) the left anterior descending (LAD) when all 3 vessels looked the same or appeared to be normal. OCT images were obtained using the LightLab C7-XR Frequency Domain OCT system during continuous contrast injection (4 mL/s, 14–18 mL total) Group None/mild rejection (n=37) ISHLT 1990 ISHLT 2004 0 0 1A 4 21 1R 1B 2 High-grade rejection (n=11) No. of Cases 7 5 3A 2R 3B 3R 4 11 0 0 ISHLT indicates International Society of Heart and Lung Transplantation; and N/A, not applicable. with a motorized pullback speed of 20 mm/s, a frame rate of 100/s, and a maximum scan length of 54 mm. OCT images were analyzed off-line by 2 independent investigators (L.D. and A.M.) using LightLab ORW software (version C.0.4). Each OCT pullback was separated into 3 segments (proximal, middle, and distal) corresponding with the coronary angiogram. After coregistration of OCT and angiographic studies and assessment of the angiograms based on the American Heart Association classification of proximal, middle, and distal segments, the OCT image was divided into (1) 3 equal segments if all 3 (proximal, middle, and distal) angiographic segments had been visualized by OCT or (2) 2 equal segments if only 2 angiographic segments (proximal and middle or middle and distal) had been visualized by OCT.6 Calibration was done for each segment, and every frame was evaluated. For interpretation of the OCT images, the internal elastic lamina (IEL) and external elastic lamina (EEL) were identified as high backscattering bands (≈20 μm). The intima is a thickening inside of the IEL, the media is a low backscattering layer between the IEL and EEL, and the adventitia is a high backscattering and heterogeneous layer outside the EEL. Plaque with attenuation has fast signal drop-off indicates lipidic plaque or macrophages; attenuation behind surface high backscattering with a narrow trailing shadow that changes frame by frame is considered to represent foamy macrophages rather than lipidic plaque.7,8 Thrombi are graded as (1) red blood cell–rich thrombus that has strong backscattering with a high degree of attenuation, (2) platelet-rich thrombus that has less backscattering with a lower degree of attenuation, or (3) mixed thrombus.9,10 Organized thrombus shows low backscattering with little attenuation.7 Microvessels within the intima appear as signal-poor voids that are sharply delineated and can usually be followed in multiple contiguous frames. Calcium is a signal-poor region with sharply delineated borders. Ruptured plaques show features of intimal tearing, disruption, or dissection of the cap. A visible abnormal branch structure (VABS) was defined as the presence of intimal thickening inside of a side branch in which both the lumen and the media of the side branch connected to the main vessel (Figure 1). For every visible side branch, the lumen diameter was measured as the largest of the minimum diameters among consecutive frames to avoid overestimation because of angulation. For quantitative analysis, we chose the frame with minimum lumen area and the maximum plaque thickness in each segment to measure EEL, IEL, and lumen area. Percent media/EEL area, intima/EEL area, and intima/IEL area11 were calculated as: % % Media EEL Intima EEL Intima area= area= EEL area − IEL area EEL area × 100; IEL area − lumen area EEL area IEL area − lumen area × 100; × 100. EEL IEL area When the EEL was not visible over a circumference of >60°, we reviewed cross-sections proximal or distal to the minimal lumen area % area= Dong et al OCT Evaluation of Transplant Vasculopathy 3 B A Figure 1. Visible abnormal branch structure. A, Consecutive frames showing intima thickening (white arrows) in a side branch from a patient with in a high-grade rejection case. B, Consecutive frames showing no intima thickening (white arrows) in a side branch from a patient with none/mild rejection. Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 slice. We only contoured the EEL if this helped to fill in the missing arc of EEL. In this cohort, 89% of attenuation had the appearance of trailing attenuation with narrow shadow. Therefore, even with attenuation, in most (90%) of the slices the EEL was analyzable. Statistical Methods Statistical analysis was performed with SAS software, version 9.1 (SAS Institute Inc, Cary, NC). For patient level data, categorical variables are presented as frequencies and compared between groups with χ2 statistics or Fisher exact test (if there was an expected cell value <5), and continuous variables are presented as median and first to third quartiles and compared between groups using Mann–Whitney U test. The correlation between mean intimal thickness versus IEL area was analyzed using Pearson correlation. Intraobserver and interobserver variability for the qualitative analysis was measured by κ test of concordance. For side branch data, a model with the generalized estimating equations approach was used to compensate for any potential cluster effect of multiple side branches in the same patient and is presented as least square means with 95% confidence intervals. To identify independent predictors of lumen dimensions, clinical variables with P<0.2 were entered into the multiple linear regression model. A P<0.05 was considered statistically significant. Results The age of donor at heart transplantation was 31±11 years (high rejection group versus none/mild rejection group: 29±8 years versus 32±12 years; P=0.42). Among them, 58% were men (high rejection group versus none/mild rejection group: 40% versus 63%; P>0.99); and 46% of donors were cytomegalovirus positive (high rejection group versus none/mild rejection group: 11% versus 57%; P=0.02). Patient characteristics are summarized in Table 2. There were no significant clinical differences between the none/mild versus high-grade rejection groups except for the time from heart transplant that was longer in the high-grade rejection group. Sirolimus and clopidogrel were more often prescribed in patients with high-grade rejection, but there were no other significant differences in medical treatment between groups (Table 3). Angiographic Findings Angiographic findings are shown in Table 4. Comparing patients with high-grade rejection to those with none/mild rejection, there were no significant differences in minimal lumen diameter in the proximal or mid segments, but the Clinical Characteristics The coronary arteries that were imaged included 44 LAD arteries, 3 left circumflex arteries, and 1 right coronary artery. OCT imaging of all 3 segments (proximal, mid, and distal) was successful in 38 cases, whereas imaging of either the distal or proximal segment was incomplete in 10 cases. Patient age at heart transplantation was 56±14 years (median, 61 years), and 77% were men. The median duration from transplantation to OCT imaging was 5.6 years: 8.2 years in the h igh-grade rejection group and 4.9 years in the low-grade rejection group (P=0.03). Among the 37 low-grade rejection patients, there were 19 patients (51%) who were >4 years after transplantation, whereas among the 11 high-grade rejection patients, there were 10 patients (91%) who were >4 years after transplantation. In 11 high-grade rejection patients, the median time of rejection from the transplantation was 4.2 years. About half of the transplant recipients were whites (26 of 48). The none/mild rejection group included 37 patients (ISHLT 0 in 4 cases, ISHLT 1A in 21 cases, ISHLT 1B in 7 cases, and ISHLT 2 in 5 cases), whereas the high-grade rejection group included 11 patients (ISHLT 3A in all cases; Table 1). There were no patients with ISHLT grade 3B or grade 4 rejection. Table 2. Patient Characteristics None/Mild Rejection (n=37) Age, y 60 (53–65) High-Grade Rejection (n=11) 64 (32–66) P Value 0.81 Male sex 76% (28) 82% (9) 1.0 Height, cm 175 (170–180) 175 (167–183) 1.0 Weight, kg 88 (69–104) 86 (75–103) 1.0 Body mass index, kg/m2 26.8 (23.8–32.3) 27.5 (26.4–30.6) 0.6 HTx indication for ICM 35% (13) 46% (5) 0.72 Duration post HTx, y 4.9 (1.0–9.0) 8.2 (7.0–11.8) 0.03 Humoral rejection 8% (3) 9% (1) 1.0 Hypertension 38% (14) 27% (3) 0.72 Dyslipidemia 38% (14) 36% (4) 1.0 Diabetes mellitus 30% (11) 36% (4) 0.72 Smoking 30% (11) 36% (4) 0.72 Prior coronary artery disease 41% (15) 46% (5) 1.0 5% (2) 9% (1) 0.55 Prior peripheral vessel disease HTx indicates heart transplantation; and ICM, ischemic cardiomyopathy. 4 Circ Cardiovasc Interv April 2014 Table 3. Medical Treatment Table 5. Optical Coherence Tomographic Finding None/Mild Rejection High-Grade Rejection (n=37) (n=11) P Value Aspirin None/Mild Rejection (n=37) High-Grade Rejection (n=11) P Value 87% (32) 82% (9) 0.65 Distal segment 0% (0) 18% (2) 0.05 EEL area, mm2 8.07 (6.24–11.30) 6.50 (5.07–7.46) 0.15 Statin 76% (28) 64% (7) 0.46 IEL area, mm 7.30 (5.16–9.73) 5.67 (4.64–6.60) 0.13 β-Blocker 19% (7) 18% (2) 1 Lumen area, mm2 6.14 (3.57–8.40) 4.31 (2.79–5.36) 0.01 ACE-I/ARB 30% (11) 27% (3) 1 0.09 (0.06–0.17) 0.22 (0.09–0.41) 0.02 CCB 46% (17) 46% (5) 0.98 Mean intima thickness, mm Steroid 76% (28) 73% (8) 1 %media/EEL area 10.3 (7.9–13.1) 11.5 (8.8–15.4) 0.27 11.7 (7.2–17.7) 35.7 (10.9–45.2) 0.009 13.1 (7.7–20.0) 39.0 (12.9–50.3) 0.007 55% (6) 0.003 Clopidogrel Tacrolimus 2 57% (21) 55% (6) 1 %intima/EEL area 8% (3) 36% (4) 0.04 %intima/IEL area Mycophenolate mofetil 68% (25) 46% (5) 0.29 Mycophenolic acid 16% (6) 9% (1) 1 Prevalence of attenuation Cyclosporine 38% (14) 36% (4) 1 Sirolimus Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 ACE-I indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blockers; and CCB, calcium channel blockers. minimal lumen diameter in the distal segment was significantly smaller in high-grade rejection patients. Qualitative parameters were not different between the 2 groups. Quantitative OCT Findings OCT findings are shown in Table 5 and Figures 2 through 4. There were no significant differences in EEL areas, IEL areas, or %media/EEL between the 2 groups. However, the mean intimal thickness, %intima/EEL area, and %intima/IEL area were all significantly greater in the high-grade rejection group, resulting in smaller lumen areas. Comparing proximal versus middle versus distal segments in the 2 groups separately, mean intimal thickness was not significantly different between any adjacent segment, including (1) distal versus middle, P=0.14, and middle versus proximal, P=0.90, in the high-grade rejection group and (2) distal versus middle, P=0.43, and middle versus proximal, P=0.10, in the none/mild rejection group. By regression analysis, mean intimal thickness did not correlate with IEL area in the high-grade rejection group (P=0.76), although there was a moderate correlation between mean intimal thickness and IEL area (R=0.38; P=0.0004) in the none/ mild rejection group. Table 4. Angiographic Findings None/Mild Rejection (n=37) High-Grade Rejection (n=11) P Value 2.04 (1.64–2.37) 1.70 (1.19–1.96) 0.009 Mid segment MLD, 2.37 (2.12–2.67) mm 2.29 (1.83–2.53) 0.25 Proximal segment MLD, mm 2.35 (2.09–3.29) 0.5 Distal segment MLD, mm 2.57 (2.24–2.94) Lumen irregularity 0% (0) 0% (0) N/A Branch orifice narrowing 3% (1) 0% (0) 1 Calcification 0% (0) 0% (0) N/A MLD indicates minimum lumen diameter; and N/A, not applicable. 9% (3) Middle segment EEL area, mm2 12.54 (8.54–15.37) 9.8 (7.63–13.79) 0.25 IEL area, mm2 11.40 (7.48–13.31) 9.10 (7.05–12.41) 0.26 Lumen area, mm2 9.43 (6.68–11.05) 6.46 (3.74–7.64) 0.03 Mean intima thickness, mm 0.14 (0.08–0.24) 0.35 (0.22–0.45) 0.002 %media/EEL area 9.7 (8.3–11.2) 9.9 (7.6–11.8) 0.67 %intima/EEL area 13.0 (8.7–18.2) 30.4 (22.8–43.0) 0.0007 %intima/IEL area 14.5 (9.5–20.7) 34.5 (24.5–46.5) 0.0006 Prevalence of attenuation 22% (8) 55% (6) 0.004 Proximal segment EEL area, mm2 17.77 (12.46–22.45) 12.36 (10.79–17.89) 0.19 IEL area, mm2 15.69 (11.28–20.45) 11.23 (9.65–15.24) 0.16 13.06 (9.11–16.08) 8.13 (6.55–12.47) 0.06 0.15 (0.11–0.21) 0.34 (0.21–0.44) 0.005 Lumen area, mm 2 Mean intima thickness, mm %media/EEL area 9.6 (8.5–11.4) 11.3 (9.1–11.7) 0.4 %intima/EEL area 11.2 (9.1–14.3) 20.9 (15.5–35.9) 0.002 %intima/IEL area 12.5 (10.4–16.5) 23.8 (18.2–39.6) 0.003 Prevalence of attenuation 13% (4) 44% (4) 0.05 EEL indicates external elastic lamina; and IEL, internal elastic lamina. In the high-grade rejection group, there were 5 patients who had 2 episodes of high-grade rejection and 6 patients who had a single episode of high-grade rejection (none had >2 episodes). Patients with 2 episodes of high-grade rejection trended toward a smaller IEL area compared with patients with a single episode of high-grade rejection (4.6 [3.2–6.4] versus 6.2 [5.7–6.6] mm2; P=0.13). Only 4 patients (3 in the none/mild rejection group and one in the high-grade rejection group) had a history of humoral rejection. Percent intimal/IEL area trended toward larger in the patients with a history of humoral rejection compared with those without a history of humoral rejection (26.1% [18.3%– 43.9%] versus 13.6% [8.8%–24.7%]; P=0.09). Qualitative OCT Findings Intraobserver and interobserver variability yielded good concordance for the diagnosis of trailing attenuation with narrow Dong et al OCT Evaluation of Transplant Vasculopathy 5 None/Mild Rejection (mm) 0.9 0.6 Mean Intima Thickness P=0.005 P=0.002 (mm2) 21 (%) 60 40 % Intima/IEL P=0.003 P=0.007 20 Proxmial Middle Distal Minimum Lumen Area 0 (%) 90 Proxmial 14 Middle Distal Plaque with Attenuation Figure 2. Optical coherence tomographic findings. Mean intima thickness, %intima/internal elastic lamina (IEL) area, and prevalence of plaque with attenuation were greater in the high-grade rejection group, which resulted in smaller minimum lumen areas in high-grade rejection group. P=0.004 P=0.06 60 P=0.03 P=0.01 Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 7 0 P=0.0006 P=0.02 0.3 0 High Grade Rejection P=0.003 P=0.054 30 Proximal Middle Distal 0 Proximal Middle shadow (κ=0.90 and κ=0.90), microvessels (κ=0.95 and κ=0.84), thrombus (κ=0.89 and κ=0.89), and VABS (к=0.84 and к=0.80). Qualitative analysis showed that patients in the high-grade rejection group had significantly greater prevalence of plaque with attenuation than the none/mild rejection group in all 3 segments: proximal, middle, and distal. The majority of attenuation had the appearance of trailing with narrow shadow, suggesting macrophages; this finding was present in 89% of plaque with attenuation in the none/mild rejection group and in all plaque with attenuation in the highgrade rejection group. Mural thrombus was found in 3 of 48 patients (6%), including 1 in the none/mild rejection group (involving <1 quadrant and 1.6 mm in length) and 2 in the high-grade rejection group. In the patient in the none/mild rejection group, a mixed thrombus was observed in the middle segment of the LAD artery. One of the patients from the high-grade rejection group had multiple mixed thrombi in both the middle and proximal segment (Figure 5A), involving 4 quadrants and a total length of 11 mm, whereas the other had an organized thrombus in the proximal segment of the LAD (Figure 5A′), involving 2 quadrants and a total length of 9 mm. One plaque rupture with no associated thrombus was found in a single patient in the high-grade rejection group. Intimal microvessels were visualized in 9 patients (19%): 5 patients with high-grade rejection and 4 patients with none/ mild rejection (46% versus 11%; P=0.02). Multiple segment involvement was observed in 4 patients and single segment involvement in 5 patients. Overall, microvessels were observed in 8 distal segments, 6 middle segments, and 8 proximal segments. In 55% (12 of 22) of the microvessels, the distribution pattern was mainly localized parallel to the lumen of the main vessel and with >3 microvessels circumferentially in one image frame (Figure 5B). Eight patients (3 with high-grade rejection and 5 with none/ mild rejection cases) had intimal calcification in ≥1 coronary artery segment (17%), and 3 patients had it in >1 segment. Overall, calcification was found in 16 segments, including 2 distal, 7 middle, and 7 proximal. In 3 patients, the calcium Distal was found in >1 coronary artery segment, and in 5 patients, the calcium was found in only 1 segment. Calcification was crescent-shaped, thin (maximum thickness <0.3 mm), and superficial in 10 instances (63%; Figure 5C). Other than the greater prevalence of plaque with attenuation and intimal microvessels in the high-grade rejection group, none of the other qualitative findings were different between the 2 groups. Side Branch OCT Analysis The analysis included 332 side branches from 44 LAD arteries. Side branch diameter was smaller in the high-grade rejection group compared with the none/mild rejection group (1.01 [0.80–1.21] versus 1.23 [1.10–1.36] mm; P=0.06). The prevalence of small side branches (<0.5 mm in lumen diameter) in the high-grade rejection group was greater compared with the none/mild rejection group (34.2% versus 23.0%; P=0.05). The prevalence of VABS was also significantly greater in the A B Figure 3. Representative none/mild rejection grade case. In the angiogram (A), the vessel looks normal from the distal to the proximal segments. In the corresponding optical coherence tomographic images (B), 3 layers of normal arterial structures are seen without any abnormal intimal thickness or attenuation. 6 Circ Cardiovasc Interv April 2014 −2.93 [−5.41, −0.45], P=0.03; lumen area at distal segment, −2.66 [−5.03, −0.29], P=0.03; average diameter of side branch per patient, −0.33 [−0.68, 0.02], P=0.07). Conversely, duration after transplant or other clinical factors including age, transplant indication for ischemic heart disease, and diabetes mellitus were not predictors. When %intima/IEL area at distal or middle segment was used as the dependent variable, both high-grade rejection group (versus none/mild rejection) and duration post transplant were independent predictors. When %intima/IEL area at proximal segment was used as the dependent variable, only high-grade rejection group was an independent variable. B A Discussion Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 Figure 4. Representative high-grade rejection case. In the angiogram (A), the middle and distal left anterior descending segments look smaller than expected from vessel tapering alone. The optical coherence tomographic image (B) shows the 3 layers of the arterial structure with proximal, middle, and distal segments having significant intimal thickening with trailing attenuation (white arrow) in the middle and distal segments. high-grade rejection group than in the none/mild rejection group (54% [47/87] versus 36% [98/272]; P=0.01). Within the none/mild group, the 12 patients with either ISHLT grade 1B or 2 rejection had a higher prevalence of VABS compared with the 25 patients with either ISHLT grade 0 or 1A rejection (57.3% versus 23.8%; P=0.0003). However, the 12 patients with either ISHLT grade 1B or 2 rejection had similar mean intimal thickness and a similar prevalence of plaque with attenuation compared with the 25 patients with either ISHLT 0 or 1A rejection grade. Predictors of OCT Findings Using multivariate linear regression, only high-grade rejection (versus none/mild rejection) was an independent predictor of lumen area at distal segment, lumen area at middle segment, lumen area at proximal segment, and the average diameter of side branch per patient (regression coefficient [95% confidence interval] and P value: lumen area at proximal segment, −3.61 [−7.28, 0.06], P=0.06; lumen area at middle segment, A A’ B B’ The principal findings of the present study are that (1) OCT demonstrated greater intimal thickening and findings suggestive of a higher prevalence of foamy macrophages in all coronary segments in patients with prior high-grade cellular rejection than those with none/mild rejection, and (2) OCT demonstrated more intimal thickening within side branches and VABS as a part of the more diffuse involvement in patients with prior high-grade rejection. The pathophysiology of CAV involves immunologic and nonimmunologic factors that cause localized inflammation with persistent vascular injury and endothelial dysfunction.12.13 As such, CAV may be conceived of as a form of chronic rejection,14 and the prevalence of CAV increases with time: 20% at 3 years, 30% at 5 years, and 45% at 8 years after transplantation.15 Histologically, there is subendothelial accumulation of lymphocytes (primarily T cells), myointimal proliferation of smooth muscles cells, development of lipid-laden foam cells, and perivascular fibrosis. Concentric intimal hyperplasia leads to progressive luminal compromise and typically results in a diffuse obliterative process of the intramural and epicardial coronary arteries.16 The early diagnosis of CAV is essential to facilitate treatment of CAV before progression to the point of requiring revascularization. However, ischemic symptoms are frequently absent or atypical because of allograft denervation. Multiple noninvasive modalities, including dobutamine stress echocardiography, pharmacological radionuclide myocardial C C’ Figure 5. Representative qualitative optical coherence tomographic findings. A and A′, Mural thrombus (white arrows) from 2 patients with International Society of Heart and Lung Transplantation (ISHLT) 3A grade rejection. A, mixed thrombus; A′, low scattering area without attenuation, indicating organized thrombus. B and B′, Intimal microvessels (white arrows). B, From an ISHLT 2 grade rejection patient; and B′, from an ISHLT 1A grade rejection patient. In both patients, the multiple microvessels were located parallel to the lumen border. C and C′, Superficial calcium (white arrows) from 2 patients with ISHLT 3A grade rejection. In both patients, there was a similar pattern of superficial broadly thin calcification parallel to the intimal surface. Dong et al OCT Evaluation of Transplant Vasculopathy 7 Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 perfusion imaging, computerized tomographic angiography, and MRI, are available, but none has replaced angiography that remains the gold standard for diagnosing CAV.17 Routine coronary angiography is, therefore, performed on a periodic basis at many cardiac transplant centers.2 On angiography, CAV usually seems diffuse and concentric,18 similar to the pathology findings,19 and differs from the lesions of typical atherosclerotic disease that tend to be more proximal, focal, and eccentric. The angiographic diagnosis of CAV provides important prognostic information. In one study, absence of angiographic disease was a significant predictor of cardiac event-free survival in heart transplant recipients.20 However, coronary angiography frequently underestimates the extent and severity of the disease. The positive predictive power of coronary angiography (compared with intravascular ultrasound [IVUS]) is only 44%,21 and IVUS detects a 5× greater number of CAV lesions than can be found angiographically in the same patients.22 The process of lumen loss can also be studied using serial IVUS. In one report of 38 cases studied annually for 5 years,23 the investigators found that early lumen loss was primarily caused by intimal thickening and that late lumen loss was caused primarily by vessel constriction (negative remodeling). Furthermore, intimal thickening determined using IVUS showed a poor prognosis in heart transplant recipients, even in the presence of normal angiography.24–27 Radiofrequency (virtual histology)-IVUS of plaque composition in CAV has extended these findings to show increasing amounts necrotic core and calcium over time that are associated with greater rejection.28–30 Because of its higher resolution compared with IVUS, OCT may be more suitable for the assessment of vessel intima and small structures3 and provides greater information about plaque components.7–10 For example, in 15 patients who were studied a mean of 2.8 years after cardiac transplant, half of the patients had lipid-rich or calcified atherosclerotic plaques.31 Another OCT evaluation of 53 heart transplant patients showed that the prevalence of thin-cap fibroatheroma, macrophages, and microchannels increased in relation to the duration from the transplant.32 In the current analysis, trailing attenuation with narrow shadow likely caused by macrophage accumulation was seen in the majority of patients, even those with none/mild rejection. In the current study, intimal microvessel formation, thrombus, calcification, and plaque rupture were found in ≈15% of patients and were located within middle or proximal segments except microvessels, which were located equally from the distal to the proximal segments. Previous OCT studies in atherosclerotic coronary artery disease in nontransplant patients suggested that intimal microvessels were related to plaque vulnerability such as thin-cap fibroatheroma or plaque rupture along with serum high sensitivity C-reactive protein and were a potential predictor of subsequent progression of nonsignificant coronary plaques, as well as of intraluminal thrombi.33,34 CAV is a diffuse process that involves not only distal arterial segments but also side branches. Because of limited resolution, previous IVUS or virtual histology-IVUS studies were unable to evaluate changes in side branches that can be detected by OCT. The effect of intimal proliferation on the luminal area of side branches may explain the significantly higher prevalence of small side branches (diameter <0.5 mm) in the high-grade rejection group in the current study. In addition, VABS was present even in some patients with none/mild rejection and before intimal thickening in the main vessel; this suggests that side branch involvement may appear earlier than the main vessel disease and may be used as a predictor of early rejection. Limitations This study included only 48 patients with only 11 patients having a history of high-grade rejection, and OCT imaging was limited to 1 coronary artery. This may have affected the statistical analysis because of the 3:1 ratio of low-to-high–grade rejection patients. The distribution of years after transplantation is skewed, especially in the high-grade rejection group who were assessed significantly later than the none/mild rejection group; this may confound the relationship between the rejection grade and the OCT findings. Many patients died from the first to the 12th year in both groups such that sampling was incomplete in both groups. None of the patients in this analysis had grade 3B or 4 (3R) rejection, so conclusions cannot be drawn about the effect of severe rejection of CAV. Correlation of OCT findings with histopathologic finding is not available. Because there was no OCT evaluation at the time of the transplant, we cannot eliminate the possibility that intimal hyperplasia already existed in the donor hearts. Despite the good reproducibility for the assessment of VABS in the current study, this diagnosis may be difficult because the side branch is located in the farfield. Finally, type I statistical error may have occurred, given the number of patients and the number of statistical tests; therefore, this analysis should be considered hypothesis generating. Conclusions In patients after cardiac allograft transplantation, OCT imaging demonstrated greater intimal thickening in patients with a history of high-grade rejection than those with mild or without rejection. Involvement was diffuse and included distal, middle, and proximal segments, as well as side branches. OCT may have the potential for early detection of CAV in heart transplantation patients. Acknowledgments We thank Khady N. Fall, MD, for her assistance in acquiring optical coherence tomographic data. Disclosures Dr Dong received grant support from Boston Scientific. Dr Mintz is a consultant for Volcano Corporation (research grant) and Boston Scientific (grant support). Dr Maehara received grant support (institutional) from Boston Scientific and honoraria from Boston Scientific. Dr Weisz is a consultant for InfraReDx. The other authors report no conflicts. The study has no external funding. References 1. Christie JD, Edwards LB, Kucheryavaya AY, Aurora P, Dobbels F, Kirk R, Rahmel AO, Stehlik J, Hertz MI. The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult lung and heart-lung transplant report–2010. J Heart Lung Transplant. 2010;29:1104–1118. 2. Pollack A, Nazif T, Mancini D, Weisz G. Detection and imaging of cardiac allograft vasculopathy. JACC Cardiovasc Imaging. 2013;6:613–623. 8 Circ Cardiovasc Interv April 2014 Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 3.Suter MJ, Nadkarni SK, Weisz G, Tanaka A, Jaffer FA, Bouma BE, Tearney GJ. Intravascular optical imaging technology for investigating the coronary artery. JACC Cardiovasc Imaging. 2011;4:1022–1039. 4.Stewart S, Winters GL, Fishbein MC, Tazelaar HD, Kobashigawa J, Abrams J, Andersen CB, Angelini A, Berry GJ, Burke MM, Demetris AJ, Hammond E, Itescu S, Marboe CC, McManus B, Reed EF, Reinsmoen NL, Rodriguez ER, Rose AG, Rose M, Suciu-Focia N, Zeevi A, Billingham ME. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J Heart Lung Transplant. 2005;24:1710–1720. 5. Pompa J, Almonacid A, Burke D. Qualitative and quantitative coronary angiography. In: Topol EJ, Teirstein PS, eds. Textbook of Interventional Cardiology. 6th ed. Philadelphia, PA: Saunders; 2011:757–775. 6. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, McGoon DC, Murphy ML, Roe BB. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975;51(4 suppl):5–40. 7. Nakano M, Otsuka F, Virmani R. Letter by Nakano et al regarding article, “optical coherence tomographic analysis of in-stent neoatherosclerosis after drug-eluting stent implantation.” Circulation. 2011;124:e954, author reply e955. 8. van Soest G, Regar E, Goderie TP, Gonzalo N, Koljenović S, van Leenders GJ, Serruys PW, van der Steen AF. Pitfalls in plaque characterization by OCT: image artifacts in native coronary arteries. JACC Cardiovasc Imaging. 2011;4:810–813. 9. Tearney GJ, Chowdhary S, Costa MA, de Silva R, Dijkstra J, Di Mario C, Dudek D, Dudeck D, Falk E, Falk E, Feldman MD, Regar E, Fitzgerald P, Garcia-Garcia HM, Garcia H, Gonzalo N, Granada JF, Guagliumi G, Holm NR, Honda Y, Ikeno F, Kawasaki M, Akasaka T, Kochman J, Koltowski L, Kubo T, Kume T, Kyono H, Lam CCS, Lamouche G, Lee DP, Leon MB, Maehara A, Adriaenssens T, Manfrini O, Mintz GS, Mizuno K, Morel M, Nadkarni S, Okura H, Otake H, Pietrasik A, Prati F, Räber L, Barlis P, Radu MD, Rieber J, Riga M, Rollins A, Rosenberg M, Sirbu V, Serruys PWJC, Shimada K, Shinke T, Shite J, Bezerra HG, Siegel E, Sonoda S, Sonada S, Suter M, Takarada S, Tanaka A, Terashima M, Thim T, Troels T, Uemura S, Bouma B, Ughi GJ, van Beusekom HMM, van der Steen AFW, van Es GA, van Es GA, van Soest G, Virmani R, Waxman S, Weissman NJ, Weisz G, Bruining N, Cho Jm. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol. 2012;59:1058–1072. 10.Yabushita H, Bouma BE, Houser SL, Aretz HT, Jang IK, Schlendorf KH, Kauffman CR, Shishkov M, Kang DH, Halpern EF, Tearney GJ. Characterization of human atherosclerosis by optical coherence tomography. Circulation. 2002;106:1640–1645. 11.Burke AP, Kolodgie FD, Farb A, Weber DK, Malcom GT, Smialek J, Virmani R. Healed plaque ruptures and sudden coronary death: evidence that subclinical rupture has a role in plaque progression. Circulation. 2001;103:934–940. 12.Vassalli G, Gallino A, Weis M, von Scheidt W, Kappenberger L, von Segesser LK, Goy JJ; Working Group Microcirculation of the Eurpean Society of Cardiology. Alloimmunity and nonimmunologic risk factors in cardiac allograft vasculopathy. Eur Heart J. 2003;24:1180–1188. 13. Weis M, von Scheidt W. Coronary artery disease in the transplanted heart. Annu Rev Med. 2000;51:81–100. 14.Schmauss D, Weis M. Cardiac allograft vasculopathy: recent developments. Circulation. 2008;117:2131–2141. 15. Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dobbels F, Kirk R, Rahmel AO, Hertz MI. The Registry of the International Society for Heart and Lung Transplantation: twenty-eighth Adult Heart Transplant Report–2011. J Heart Lung Transplant. 2011;30:1078–1094. 16. Billingham ME. Histopathology of graft coronary disease. J Heart Lung Transplant. 1992;11(3 pt 2):S38–S44. 17. Colvin-Adams M, Agnihotri A. Cardiac allograft vasculopathy: current knowledge and future direction. Clin Transplant. 2011;25:175–184. 18. Gao SZ, Alderman EL, Schroeder JS, Silverman JF, Hunt SA. Accelerated coronary vascular disease in the heart transplant patient: coronary arteriographic findings. J Am Coll Cardiol. 1988;12:334–340. 19.Lin H, Wilson JE, Kendall TJ, Radio SJ, Cornhill FJ, Herderick E, Winters GL, Costanzo MR, Porter T, Thieszen SL. Comparable proximal and distal severity of intimal thickening and size of epicardial coronary arteries in transplant arteriopathy of human cardiac allografts. J Heart Lung Transplant. 1994;13:824–833. 20. Barbir M, Lazem F, Banner N, Mitchell A, Yacoub M. The prognostic significance of non-invasive cardiac tests in heart transplant recipients. Eur Heart J. 1997;18:692–696. 21. Störk S, Behr TM, Birk M, Uberfuhr P, Klauss V, Spes CH, Angermann CE. Assessment of cardiac allograft vasculopathy late after heart transplantation: when is coronary angiography necessary? J Heart Lung Transplant. 2006;25:1103–1108. 22. Tuzcu EM, Kapadia SR, Tutar E, Ziada KM, Hobbs RE, McCarthy PM, Young JB, Nissen SE. High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation. 2001;103:2705–2710. 23.Tsutsui H, Ziada KM, Schoenhagen P, Iyisoy A, Magyar WA, Crowe TD, Klingensmith JD, Vince DG, Rincon G, Hobbs RE, Yamagishi M, Nissen SE, Tuzcu EM. Lumen loss in transplant coronary artery disease is a biphasic process involving early intimal thickening and late constrictive remodeling: results from a 5-year serial intravascular ultrasound study. Circulation. 2001;104:653–657. 24. Mehra MR, Ventura HO, Stapleton DD, Smart FW, Collins TC, Ramee SR. Presence of severe intimal thickening by intravascular ultrasonography predicts cardiac events in cardiac allograft vasculopathy. J Heart Lung Transplant. 1995;14:632–639. 25. Rickenbacher PR, Pinto FJ, Lewis NP, Hunt SA, Alderman EL, Schroeder JS, Stinson EB, Brown BW, Valantine HA. Prognostic importance of intimal thickness as measured by intracoronary ultrasound after cardiac transplantation. Circulation. 1995;92:3445–3452. 26.Tuzcu EM, Kapadia SR, Sachar R, Ziada KM, Crowe TD, Feng J, Magyar WA, Hobbs RE, Starling RC, Young JB, McCarthy P, Nissen SE. Intravascular ultrasound evidence of angiographically silent progression in coronary atherosclerosis predicts long-term morbidity and mortality after cardiac transplantation. J Am Coll Cardiol. 2005;45:1538–1542. 27. Kobashigawa JA, Tobis JM, Starling RC, Tuzcu EM, Smith AL, Valantine HA, Yeung AC, Mehra MR, Anzai H, Oeser BT, Abeywickrama KH, Murphy J, Cretin N. Multicenter intravascular ultrasound validation study among heart transplant recipients: outcomes after five years. J Am Coll Cardiol. 2005;45:1532–1537. 28. König A, Kilian E, Sohn HY, Rieber J, Schiele TM, Siebert U, Gothe RM, Reichart B, Klauss V. Assessment and characterization of time-related differences in plaque composition by intravascular ultrasound-derived radiofrequency analysis in heart transplant recipients. J Heart Lung Transplant. 2008;27:302–309. 29. Hernandez JM, de Prada JA, Burgos V, Sainz Laso F, Valls MF, Vilchez FG, Llano M, Ruano J, Zueco J, Colman T, Duran RM. Virtual histology intravascular ultrasound assessment of cardiac allograft vasculopathy from 1 to 20 years after heart transplantation. J Heart Lung Transplant. 2009;28:156–162. 30.Raichlin E, Bae JH, Kushwaha SS, Lennon RJ, Prasad A, Rihal CS, Lerman A. Inflammatory burden of cardiac allograft coronary atherosclerotic plaque is associated with early recurrent cellular rejection and predicts a higher risk of vasculopathy progression. J Am Coll Cardiol. 2009;53:1279–1286. 31. Khandhar SJ, Yamamoto H, Teuteberg JJ, Shullo MA, Bezerra HG, Costa MA, Selzer F, Lee JS, Marroquin OC, McNamara DM, Mulukutla SR, Toma C. Optical coherence tomography for characterization of cardiac allograft vasculopathy after heart transplantation (OCTCAV study). J Heart Lung Transplant. 2013;32:596–602. 32. Cassar A, Matsuo Y, Herrmann J, Li J, Lennon RJ, Gulati R, Lerman LO, Kushwaha SS, Lerman A. Coronary atherosclerosis with vulnerable plaque and complicated lesions in transplant recipients: new insight into cardiac allograft vasculopathy by optical coherence tomography. Eur Heart J. 2013;34:2610–2617. 33. Uemura S, Ishigami K, Soeda T, Okayama S, Sung JH, Nakagawa H, Somekawa S, Takeda Y, Kawata H, Horii M, Saito Y. Thin-cap fibroatheroma and microchannel findings in optical coherence tomography correlate with subsequent progression of coronary atheromatous plaques. Eur Heart J. 2012;33:78–85. 34. Kitabata H, Tanaka A, Kubo T, Takarada S, Kashiwagi M, Tsujioka H, Ikejima H, Kuroi A, Kataiwa H, Ishibashi K, Komukai K, Tanimoto T, Ino Y, Hirata K, Nakamura N, Mizukoshi M, Imanishi T, Akasaka T. Relation of microchannel structure identified by optical coherence tomography to plaque vulnerability in patients with coronary artery disease. Am J Cardiol. 2010;105:1673–1678. Downloaded from http://circinterventions.ahajournals.org/ by guest on November 17, 2016 Optical Coherence Tomographic Evaluation of Transplant Coronary Artery Vasculopathy With Correlation to Cellular Rejection Liang Dong, Akiko Maehara, Tamim M. Nazif, Ari T. Pollack, Shigeo Saito, LeRoy E. Rabbani, Mark A. Apfelbaum, Kate Dalton, Jeffrey W. Moses, Ulrich P. Jorde, Ke Xu, Gary S. Mintz, Donna M. Mancini and Giora Weisz Circ Cardiovasc Interv. published online April 8, 2014; Circulation: Cardiovascular Interventions is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2014 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-7640. Online ISSN: 1941-7632 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circinterventions.ahajournals.org/content/early/2014/04/08/CIRCINTERVENTIONS.113.000949 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Interventions can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Interventions is online at: http://circinterventions.ahajournals.org//subscriptions/