Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Plant disease resistance wikipedia , lookup
Common cold wikipedia , lookup
Antimicrobial peptides wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Infection control wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
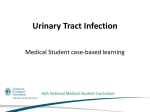
european urology 49 (2006) 235–244 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review - Infections Treatment of Bacterial Urinary Tract Infections: Presence and Future Florian M.E. Wagenlehner *, Kurt G. Naber Urologic Clinic, Hospital St. Elisabeth, Straubing, Germany Article info Abstract Article history: Accepted December 12, 2005 Published online ahead of print on January 4, 2006 Bacterial urinary tract infections (UTIs) are frequent infections in the outpatient as well as in the nosocomial setting. The stratification into uncomplicated and complicated UTIs has proven to be clinically useful. Bacterial virulence factors on the one side and the integrity of the host defense mechanisms on the other side determine the course of the infection. In uncomplicated UTIs Escherichia coli is the leading organism, whereas in complicated UTIs the bacterial spectrum is much broader including Gram-negative and Gram-positive and often multiresistant organisms. The therapy of uncomplicated UTIs is almost exclusively antibacterial, whereas in complicated UTIs the complicating factors have to be treated as well. There are two predominant aims in the antimicrobial treatment of both uncomplicated and complicated UTIs: (i) rapid and effective response to therapy and prevention of recurrence of the individual patient treated; (ii) prevention of emergence of resistance to antimicrobial chemotherapy in the microbial environment. The main drawback of current antibiotic therapies is the emergence and rapid increase of antibiotic resistance. To combat this development several strategies can be followed. Decrease the amount of antibiotics administered, optimal dosing, prevention of infection and development of new antibiotic substances. The aim of this review is to highlight the current and to describe future treatment options for UTIs. # 2005 Elsevier B.V. All rights reserved. Keywords: Urinary tract infections (UTI) Uncomplicated and complicated UTI Antibiotic resistance of uropathogens Antibiotic treatment New antiinfectives for treatment of UTI * Corresponding author. Urologic Clinic, Hospital St. Elisabeth, St. Elisabeth Str. 23, D-94315 Straubing, Germany. Tel. +49 9421 710 6702; Fax: +49 9421 710 1717. E-mail address: [email protected] (Florian M.E. Wagenlehner). 1. Background Urinary tract infections (UTIs) are among the most prevalent microbial diseases, and their financial burden on society is substantial. In the United States of America, UTIs are responsible for over 7 million physician visits annually, including more than 2 million visits for cystitis [1,2]. Approximately 15% of all community-prescribed antibiotics in the United States are dispensed for 0302-2838/$ – see front matter # 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2005.12.017 236 european urology 49 (2006) 235–244 UTI, at an estimated annual cost of over $1 billion [3]. Furthermore, the direct and indirect costs associated with community-acquired UTIs in the United States alone exceed an estimated $1.6 billion [2]. UTIs account for more than 100,000 hospital admissions annually, most often for pyelonephritis [1,2], and they also account for at least 40% of all hospital-acquired infections and are in the majority of cases catheter-associated [4–6]. Nosocomial bacteriuria develops in up to 25% of patients requiring a urinary catheter for 7 days, with a daily risk of 5% [6]. It has been estimated that an episode of nosocomial bacteriuria adds $500 to $1,000 [7,8] to the direct cost of acute-care hospitalization. In addition the pathogens are fully exposed to the nosocomial environment, including selective pressure by antibiotic or antiseptic substances. Therefore nosocomial UTIs comprise perhaps the largest institutional reservoir of nosocomial antibioticresistant pathogens [6]. Whereas community acquired UTIs are often uncomplicated, almost all nosocomial UTIs are complicated infections. Complicated UTI is a very heterogenous entity, with a common pattern of the following complicating factors: - anatomical, structural or functional alterations of the urinary tract (e.g. stents, urine transport disturbances, instrumentation of the urinary tract, stones, tumors, neurological disorders) - impaired renal function, by parenchymal diseases, or pre,-intra,-or post renal nephropathies (e.g. acute, chronic renal insufficiencies, heart insufficiency) - accompanying diseases, that impair the patients immune status (e.g. diabetes mellitus, liver insufficiency, immunosuppression, cancer, AIDS, hypothermia). (ii) prevention of emergence of resistance to chemotherapy in the microbial environment or at least prevention of further increase of resistance. 2.1. Current treatment and prophylaxis of UTI Two major strategies currently exist in the pharmacological treatment and prophylaxis of UTIs: (i) Antimicrobial chemotherapy and (ii) Vaccines. 2.1.1. Chemotherapy The currently recommended chemotherapeutic classes and dosages of antiinfectives for the treatment of bacterial UTI are listed in Table 1. The target and mechanism of actions of chemotherapeutic drugs is shown in Fig. 1. Antimicrobial susceptibility levels are often gauged relative to what antibiotic concentration is achievable in the blood. However tissue levels in renal parenchyma, the deeper layer of the urinary bladder wall or in the prostate may be more relevant in the treatment of UTI. Because these concentrations are difficult to assess in humans, urinary concentrations or antimicrobial activity levels in the urine are frequently consulted to evaluate the activity of an antibiotic substance in the treatment of UTI [9]. The urinary excretion and the determination of the activity of a substance in urine is therefore important to assess if a substance is suitable for treatment of UTI. The urinary excretion of fluoroquinolones for example differs widely between substances. A high urinary excretion For antimicrobial chemotherapy the bacterial spectrum, it’s antimicrobial resistance patterns and the development of both over the time is critical for an effective chemotherapy. The prevalence of uropathogens is different comparing uncomplicated and complicated UTI. 2. Aims in the treatment of UTI There are two predominant aims in the treatment of both uncomplicated and complicated UTIs: (i) rapid and effective response to therapy and prevention of recurrence in the individual patient treated. Fig. 1 – Target and mechanism of actions of current and future antibacterial substances [modified after [50]. DHFA – dihydrofolic acid; THFA – tetrahydrofolic acid; PABA – para-amino-benzoic acid. 237 european urology 49 (2006) 235–244 Table 1 – Groups and dosages of current chemotherapeutics for the treatment of UTI in adults Antibiotic groups Antimicrobial substance b-lactams Mecillinam Aminopenicillin + BLI Acylureidopenicillin + BLI Cephalosporin Gr. 1 Cephalosporin Gr. 2 Cephalosporin Gr. 3 Cephalosporin Gr. 3a Cephalosporin Gr. 3b Cephalosporin Gr. 4 Carbapenem Gr. 1 Carbapenem Gr. 2 Fluoroquinolones Fluoroquinolone Fluoroquinolone Fluoroquinolone Fluoroquinolone Gr. Gr. Gr. Gr. 1 2 3 4 Daily dosage oral i.v./i.m. Pivmecillinam Ampicillin/Sulbactam Amoxicillin/Clavulanic acid Piperacillin/Tazobactam Cephalexin Cefuroxime axetil Cefuroxime Cefotiam Cefpodoxim proxetile Cefixime Ceftibuten Cefotaxime Cetriaxone Ceftazidime Cefepime Ertapenem Imipenem Meropenem 2 200*–400* mg 2 750 mg 3 625–1000 mg – for prophylaxis only 2 250*–500 mg – – 2 200 mg 1 400 mg 1 200*–400 mg – – – – – – – – 3 0.75–3 g 3 1.2–2.2 g 3 2.5–4.5 g – – 3 0.75–1.5 g 2–3 1–2 g – – – 2–3 1–2 g 1 1–2 g 2–3 1–2 g 22g 11g 3–4 0.5–1 g 3 0.5–1 g Norfloxacin Ciprofloxacin Levofloxacin Gatifloxacin 2 400* mg 2 500–750 mg 1–2 500 mg 1 400 mg – 2–3 400 mg 1–2 500 mg 1 400 mg Pyrimethamines Trimethoprim Trimethoprim + Sulfamethoxazole 2 200 mg 2 160 mg + 2 800 mg Fosfomycines Fosfomycine Fosfomycin-trometamol 1 3* g Nitrofuranes Nitrofurane Nitrofurantoin 3 100* mg Gentamicin Tobramycin Amikacin – – – 1 5–7 mg/BW 1 5–7 mg/BW 1 15 mg/BW Linezolid 2 600 mg 2 600 mg Vancomycin Teicoplanin – – 2 1000 mg 1 400 mg Aminoglycosides Aminoglycoside Oxazolidinones Oxazolidinone Glycopeptides Glycopeptide BLI – beta-lactamase inhibitor; Gr. – group according to PEG [31]; BW – body weight (kg); *recommended for uncomplicated UTI. (75%) can be observed with gatifloxacin (80%), levofloxacin (84%), lomefloxacin (75%) and ofloxacin (81%). An intermediate excretion rate (40–74%) is seen with ciprofloxacin (43%), enoxacin (53%), fleroxacin (67%), and a low excretion rate (<40%) is seen with gemifloxacin (28%), moxifloxacin (20%), norfloxacin (20%), pefloxacin (14%) and sparfloxacin (10%) [9]. Whereas most of the drugs with high or intermediate excretion achieved the clinical indication for the treatment of UTI, of the drugs with low excretion only the older substance norfloxacin achieved this indication, possibly because of the lack of comparator substances at these days. The newer fluoroquinolone substances gemifloxacin and moxifloxacin both have passed phase III UTI studies with the comparator agents ciprofloxacin, ofloxacin or levofloxacin with generally unsatisfying results (data on file Bayer Healthcare, SmithKline Beecham). As a result of these studies the indication for the treatment of UTI in both substances was not achieved up to date. Therefore both pharmacokinetic parameters, serum concentration and urinary excretion are currently used to evaluate if an antibiotic substance might be suitable for the treatment of UTI. 238 european urology 49 (2006) 235–244 The main drawback of current antibiotic therapies is the emergence and rapid increase of antibiotic resistance [10]. Since antibiotics have been introduced into clinical medicine, antibiotic resistant bacteria have evolved [11]. Antibiotic resistance mechanisms have recently been alluded to in the European Urology Update Series 2, 2004, page 125–135 [10]. The overall cause of increasing antibiotic resistance is selective pressure by antimicrobial substances in various environmental settings causing antibiotic resistant bacterial clones, followed by the distribution of such clones facilitated by modern medico-social circumstances [10]. The development of new antimicrobial substances in the past has counterbalanced this trend. However we are currently approaching a resistance level that might pose a risk to loose effectiveness of antibiotic treatment in the future. The epidemiology of antibiotic resistant bacteria varies with type of infection, with medical speciality, with region, and with time. 2.1.2. Vaccines There are two different agents for immunisation currently availabale. Uro-vaxom1 and Strovac1. Both preparations are recommended for patients with recurrent uncomplicated UTIs. Uro-vaxom1 is an orally administered bacterial extract consisting of immunostimulating components derived fom 18 uropathogenic E. coli strains [12]. A metaanalysis on five placebo controlled, double-blind studies comprising 601 women resulted in a pooled odds ratio of 2.28. UTIs per year were reduced from 1 to a rate of 0.15–0.82 [13]. In a multicenter, double-blind study 453 female patients were enrolled and Uro-vaxom1 resulted in a 34% reduction of UTIs in patients compared to placebo [14]. Therefore the oral immunotherapy with Uro-vaxom is effective in the prevention of recurrent UTI. Nevertheless a metaanalysis showed that if antibiotic prophylaxis was compared with placebo the reduction of recurrent UTIs was 81% with antibiotics compared to placebo [15]. Unfortunately there are no data comparing Uro-vaxom1 with antibiotics in the prevention of recurrent UTI. Strovac1 is a whole cell bacterial extract derived from uropathogenic E. coli strains, P. mirabilis, M. morganii, K. pneumoniae and E. faecalis. The preparation is administered intramuscularly also for prevention of recurrent UTI. In an prospective, comparing study 41 patients with recurrent uncomplicated UTI were evaluated. The rate of reinfections within 6 months was 41% in patients treated with SulcoUrovac1 versus 96% in patients receiving placebo [16]. Follow-up studies, however should be carried out. 2.1.3. Probiotics The use of probiotics entails prophylaxis and treatment of UTI and is mainly concentrated on Lactobacilli. Conflicting results have been observed in clinical trials and animal studies mostly because unspecific strains of Lactobacilli have been used. Positive results have only been obtained using well characterized strains [17]. Application for prophylaxis can be intravaginal or oral. For treatment probiotics were mainly installed into the bladder. Clinical studies using vaginally administered Lactobacillus rhamnosis GR1 in combination with either L. reuteri B 54 or RC 14 resulted in reduced UTI recurrences. In one study of 52 women, UTI recurrences were reduced from an average of 6 per year to 1.6 with once weekly vaginal suppositories of GR-1/B-54 [18]. A clinical randomized, placebo controlled study of 64 women using daily oral intake of L. rhamnosus GR-1 and L. reuteri RC-14 led to a significant reduction in uropathogens and yeast in the vagina [19]. It can possibly be concluded from such findings that UTI might also be preventable by oral intake of specific lactobacilli. Few studies have shown positive results in the treatment of UTI by probiotics. One such animal study showed that after therapeutic application of Lactobacillus murinus bladder counts of treated mice were significantly lower although no significant differences were detected in P. mirabilis kidney colonisation of treated and non-treated animals [20]. 3. Future strategies in the treatment of bacterial UTI The current research goals comprise the following targets: - known substances are improved in terms of higher bioavailability, longer half life, better PK/PD performance, other formulations (i.e. extended/ gastric release formulation; liposomal formulation). - known substances are evaluated for other indications (i.e. UTI). - new derivatives of known substance classes are developed in order to enlarge the bacterial spectrum, improve bioavailability, improve antimicrobial action (i.e. younger generation substances). - new substance classes which should have new molecular targets are developed. - new strategies to improve susceptibility of bacteria are developed (i.e. efflux-pump inhibitors). european urology 49 (2006) 235–244 - new strategies to slow down the emergence of antimicrobial resistance are developed. - alternative antimicrobial substances are under discovery (e.g. bacteriophages, bacteriophage enzymes). - new compounds for vaccination in uncomplicated, and possibly as well as in complicated UTI are developed. Bacteria exhibit an enormous repertoire of different resistance mechanisms. Unspecific mechanisms such as reduced permeability or efflux alter the tolerance to antibiotic substances less than specific mechanisms, such as inactivation of the antibiotic for example. However the antibiotic spectrum targeted is much more extensive. On the other hand unspecific mechanisms can also be induced by non antibiotic substances such as salicylates. Low-level resistance can thus be confered and give bacteria a selection-advantage [10]. What parameters should be assessed for new drugs to become included in the treatment of UTI? Although there are no exact quantitative prerequesites, the following qualities should be considered: - coverage of the respective bacterial spectrum (uncomplicated versus complicated UTIs) - antimicrobial activity in urine in an acidic as well as alkaline environment - sufficient urinary excretion of the drug 3.1. Emerging vaccines Vaccination theoretically is the best strategy to prevent bacterial infections. There are however some pitfalls in the vaccination against UTIs: Complicated UTIs show a highly heterogenous bacterial spectrum. In uncomplicated UTIs E. coli is the predominant pathogen. However infections and recurrent infections are usually caused by a variety of E. coli strains. All uropathogenic E. coli as a common feature have a FimH-chaperone-adhesin on the tip of their type 1 fimbriae. A FimH adhesion-based vaccine, which showed promising results in animal and in vitro studies [24,25], so far could not enter larger vaccination trials in humans. A somewhat different approach is made by using a vaginal vaccine containing 10 heat killed uropathogenic bacteria. A placebo-controlled phase II clinical trial was performed in 54 women. Women receiving immunisation experienced an infection in 45%, whereas the placebo treated women experienced an infection in 89% [26]. Based on this result vaginal mucosal vaccine seem to be effective. P. mirabilis is a difficult to treat pathogen causing complicated UTIs especially in patients with permanent catheters or stents. The urease produced by this organism leads to stone formation and catheter blockage. The primary surface antigen is the MR/P fimbria is a good candidate for vaccination. In vitro studies with a MrpH vaccine showed promising results [27]. Emerging chemotherapeutics Emerging compounds are discussed in Table 2 regarding the following parameters: Substance, class, mode of action, bacterial spectrum, pharmacokinetics with emphasis on urinary excretion, opinion about success. The target and mechanism of actions of future chemotherapeutic drugs are shown in Fig. 1. 3.2. 3.3. 239 4. Prevention of emergence of antibiotic resistance The most important draw-back in the treatment of UTIs is the development of antimicrobial resistance. The prevention of emergence of resistance in human medicine entails several strategies: Emerging novel strategies Bacteriophage lytic enzymes are highly evolved molecules produced by bacterial viruses to digest the bacterial cell wall for bacteriophage progeny release [21]. These enzymes have been used successfully in animal models to treat bacterial infections in blood and mucosal surfaces. Phages or their enzymes are very specific for the pathogen without disturbing the normal flora. These novel antimicrobial strategies have shown very interesting in vitro results [22,23]. The further development might be promising, because this strategy involves highly conserved evolutionary mechanisms that have proven to be efficacious in nature over millions of years. - decrease of antibiotic consumption antibiotic cycling new dosing strategies for antibiotics combination of two classes of antibiotics All strategies not specifically designed for antimicrobial therapy of UTI may have to be adjusted accordingly. 4.1. Decrease of antibiotic consumption To lower antibiotic consumption in UTI three strategies are developed and are evidence based by several good clinical studies: (i) asymptomatic 240 european urology 49 (2006) 235–244 Table 2 – Emerging compounds are discussed regarding substance-name, antibiotic class and characteristics (mode of action, bacterial spectrum, pharmacokinetics with emphasis on urinary excretion, opinion about success) Antibiotic substance Antibiotic class Characteristics Daptomycin (intravenous) Lipopetide-antibiotic Exerts its antibacterial activity by disrupting multiple aspects of the bacterial membrane function. Specific activity against Gram-positive pathogens including MRSA and VRE, not active against Gram-negative bacteria. Urinary excretion is 78%. Clinically relevant toxicities are limited to skeletal muscle effects, at higher dose levels, peripheral nerve effects. The high urinary excretion promises activity in UTI, however the large molecule might hinder distribution into urinary tract tissues. The specific Gram-positive activity restricts the substance to treatment of a relative small proportion of UTIs [32–37]. Tigecycline (intravenous) Glycylcyline Exerts its antibacterial activity by inhibiting protein synthesis. Good activity against Gram-positive pathogens including MRSA and VRE, and against E. coli, Klebsiella spp., Enterobacter spp. and C. freundii, including ESBL producing organisms. Less active against P. aeruginosa, Proteus spp., M. morganii and S. marcsecens because of efflux-mechanisms. Urinary excretion is approximately 14%. Side effects observed in general were mild. The substance covers an interesting bacterial spectrum for the treatment of UTI, although difficult to treat organisms, such a P. aeruginosa or Proteus spp. are more resistant because of efflux pump activity. The relatively low urinary excretion might be a potential drawback in the treatment of UTI [38]. Cefozopran (intravenous) Cephalosporin Strong activity against P. aeruginosa. Because of the specific activity against P. aeruginosa this compound is of potential interest for the treatment of complicated UTI [39]. Ceftobiprole (intravenous) Cephalosporin Anti-MRSA cephalosporin. Against Gram-negative bacteria comparable activity to group 3 and 4 cephalosporins. The spectrum of activity towards P. aeruginosa resembles that of ceftazidime. Limited activity against putative ESBL poducers but good activity against putative high-level AmpC producers. Urinary excretion is about 90%. Because of the wide range of activity against most uropathogens and the high urinary excretion, the substance is of potential interest in the treatment of UTI [40]. Doripenem (intravenous) Carbapenem Exerts activity against Gram-positive bacteria except MRSA and enterococci and Gram-negative bacteria including imipenem resistant P. aeruginosa. Urinary excretion is 75%. Doripenem is highly excreted in urine and shows excellent activity against P. aeruginosa. Therefore it is of potential interest for treatment of complicated UTI [41]. Not indicated b-lactamase inhibitors Novel b-lactamase inhibitors are under development for the potential treatment of UTI. Because of the increasing prevalence of ESBL-producing enterobacteria in UTIs, novel b-lactamase inhibitors might be promising. Ciprofloxacin XR (extended release) (oral) Fluoroquinolone Exerts identical antibacterial activity as ciprofloxacin targeting predominantly Gram-negative pathogens with good activity against P. aeruginosa. Urinary excretion is 40%. Ciprofloxacin XR is a once daily formulation, overall comparable to twice daily ciprofloxacin [42–44]. Balofloxacin (oral) Fluoroquinolone Exerts good antibacterial activity against Gram-positive pathogens, but in comparison to other fluoroquinolones decreased activity against Gram-negative pathogens. Urinary excretion is 86%. Balofloxacin is in the treatment of UTI probably not superior to other fluoroquinolones [45]. european urology 49 (2006) 235–244 241 Table 2 (Continued ) Antibiotic substance Antibiotic class Characteristics Garenoxacin (oral and intravenous) Des-F(6)-quinolone Not indicated Dihydrofolate reductase inhibitors Exerts good antibacterial activity against Gram positive pathogens. Activity against Gram-negative pathogens is comparable to fluoroquinolones, such as ciprofloxacin or levofloxacin, activity against P. aeruginosa is poor. It seems that garenoxacin exerts also activity against fluoroquinolone resistant strains. The ability to induce resistance in vitro is apparently less than with fluoroquinolones such as levofloxacin. Urinary excretion is 30 to 40%. In view of the increasing quinolone resistance, substances of this class with decreased cross resistance and less susceptibility to resistance emergence are needed. Des-F(6)-quinolone derivatives like garenoxacin are promising substances for the treatment of UTI [46]. Novel dihydrofolate reductase inhibitors are under discovery. The novel compounds are more active against Gram-positive pathogens. Because of the long lasting activity of trimethoprim, novel dihydrofolate reductase inhibitors are generally of interest in the treatment of UTI. Not indicated MurA inhibitors Not indicated Bacterial efflux pump inhibitors Not indicated Siderophore-b-lactam conjugates Exert activity against Gram-positive and Gram-negative organisms to a variable degree. They target the bacterial enzyme MurA and thus inhibit cell wall synthesis. In view of the increasing antimicrobial resistance novel acting antibiotics are of interest for all kinds of bacterial infections [47]. Exert activity in combination with other antimicrobials against bacterial species that overexpress efflux pumps, such as P. aeruginosa. Efflux pump inhibitor agents have provided proof-of-principle of potentiation of other animicrobials both in vitro and in vivo. The initial practical application of improving activity against P. aeruginosa confirms that existing antibiotics can be potentiated by inhibition of efflux pumps, and suggests that efflux pump inhibitors may be a possible future treatment option that would address an unmet medical need. In addition efflux pumps contribute to a large extent to the emergence of resistance against different antibiotic classes. Efflux pump inhibitors can narrow the mutant selection window and thus slow down emergence of antibiotic resistance [48]. Novel strategy for the potential treatment of Gram-negative bacterial infections, including P. aeruginosa. Siderophore substances are covalently bound to aminopenicillins. Because of the bacterial spectrum covered, siderophore-b-lactam conjugation is a novel strategy of interest for the treatment of UTIs [49]. bacteriuria must not be treated in general (there are some exceptions), (ii) short-term therapy of uncomplicated UTI by suitable antimicrobial agents, and iii) low dose prophylaxis in uncomplicated recurrent UTI, respectively development of effective vaccines. 4.2. Antibiotic cycling For antibiotic cycling there are practically no reliable studies available concerning treatment of UTI. There is, however, a more or less general agreement that the overuse of one group of antibiotics selecting for similar resistance genes should be avoided especially in a hospital of institutional setting. Therefore good guidelines recommend in general alternative substances as well, to allow antibiotic cycling. 4.3. Antibiotic dosing The key idea of the third strategy, however yet clinically untested, is based on the use of antibiotic concentrations that require bacterial cells to obtain two concurrent resistance mutations for growth. That concentration has been called mutant prevention concentration (MPC) because no resistant bacterial colony is recovered even when high numbers of bacterial cells are plated. Resistant mutants are selected exclusively within a vulnerable concentration range (mutant selection window) that extends from the point where growth inhibition begins, approximately by the minimal inhibitory concentration, up to the mutant prevention concentration [28]. If the antibiotic dose given is high enough also to kill the mutant population, the selection of clinically resistant mutants could be restricted [29]. A further idea in this respect is to narrow the mutant selection window by developing appropriate substances, for example those which lower the MPC, or those that lower these concentrations of other drugs (e.g. efflux pump inhibitors). Therefore drugs with the most favourable pharmacokinetic/pharmacodynamic characteristics should be used as first-line 242 european urology 49 (2006) 235–244 agents in order to preserve the potential of a specific drug class and, most importantly, to provide the patient with an optimally effective regimen. On the other hand the dosing of an antibiotic should be aimed high enough to reach the MPC. 4.4. Combination of two classes of antibiotics For some organisms or in some infections it is difficult to find antibiotics that can be dosed high enough to prevent emergence of antibiotic resistance. A typical example is antibiotic treatment of M. tuberculosis where combination therapy with two or more antibiotic substances of different classes is recommended. In order to become resistant against two antibiotic substances, two concurrent mutations are required for bacterial growth, which has a very low probability to occur [28]. Clinical studies in UTIs however are very scarce. In one study combination therapy with a macrolide and ciprofloxacin showed higher efficacy in eliminating uropathogens than the single therapy with ciprofloxacin [30]. The success of the macrolide in this study however was more attributed to the specific biofilm inhibiting effect of the macrolide [30]. - The low dose antibiotic prophylaxis in recurrent UTIs is effective, however the emergence of antibiotic resistant pathogens might be underestimated, although the idea of antibiotic prophylaxis is to use low dosages that do not fall within the mutant selection window and thus theoretically should not cause emergence of resistance. - Vaccination will be an important issue in the future. The most experience has been made with vaccines in recurrent uncomplicated cystitis, because a single species E. coli causes more than 90% of episodes. Desirable would be more attempts for vaccination in complicated UTIs, especially with difficult to treat organisms like P. aeruginosa. The ongoing process in the treatment of infectious diseases is highly dynamic. The substantial difference to non-infectious diseases is that the management of an infection in a single patient allways has an effect on the environment. Considering this, the management of infectious diseases must be highly responsible. References 5. Conclusion There are a number of new derivatives of classes in use. In most cases these derivatives are subject to cross resistance inherent to the whole substance class. Therefore new classes of antibiotics with unrelated mode of action are a more valuable development. The indications for treatment of such novel substances should be selected very carefully, in order to conserve new substance classes as long as possible. For a variety of reasons however new substance classes will be increasingly difficult to launche. Therefore new derivatives of classes in use should be thoroughly screened for their potential to induce resistance. Substances with a low potential to select resistant strains will be highly welcome. Very important in that respect will be combinatory agents that impede general widespread mechanisms of resistance, such as efflux pump inhibitors. Novel antimicrobial strategies, such as the use of bacteriophagal enzymes urgently need to be evaluated further. The best strategy in infection in general is the prevention of the disease. In UTI there is a variety of concepts involved: - Hygienic issues and catheter materials are predominantly important in complicated, health-care associated UTIs. [1] Warren JW, Abrutyn E, Hebel JR, Johnson JR, Schaeffer AJ, Stamm WE. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Infectious Diseases Society of America (IDSA). Clin Infect Dis 1999;29(4):745–58. [2] Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med 2002; 113(Suppl. 1A):5S–13S. [3] Mazzulli T. Resistance trends in urinary tract pathogens and impact on management. J Urol 2002;168(4 Pt 2):1720–2. [4] Gales AC, Jones RN, Gordon KA, et al. Activity and spectrum of 22 antimicrobial agents tested against urinary tract infection pathogens in hospitalized patients in Latin America: report from the second year of the SENTRY antimicrobial surveillance program (1998). J Antimicrob Chemother 2000;45(3):295–303. [5] Ruden H, Gastmeier P, Daschner FD, Schumacher M. Nosocomial and community-acquired infections in Germany. Summary of the results of the First National Prevalence Study (NIDEP). Infection 1997;25(4):199–202. [6] Maki DG, Tambyah PA. Engineering out the risk for infection with urinary catheters. Emerg Infect Dis 2001; 7(2):342–7. [7] Patton JP, Nash DB, Abrutyn E. Urinary tract infection: economic considerations. Med Clin North Am 1991; 75(2):495–513. [8] Lai KK, Fontecchio SA. Use of silver-hydrogel urinary catheters on the incidence of catheter-associated urinary tract infections in hospitalized patients. Am J Infect Control 2002;30(4):221–5. european urology 49 (2006) 235–244 [9] Naber KG. Which fluoroquinolones are suitable for the treatment of urinary tract infections? Int J Antimicrob Agents 2001;17(4):331–41. [10] Wagenlehner F, Naber KG. Antibiotics and resistance of uropathogens. EAU Update Series 2004;2:125–35. [11] Abraham E, Chain E. An encyme from bacteria able to destroy penicillin. Nature 1940;146:837. [12] Bauer H, Bleßmann GS, Pitrow DB, Rahlfs VW. Prevention of recurrent urinary tract infections with immunoactive E. coli fractions. Eur J Obstet Gyn 1999;86:33. [13] Bauer HW, Rahlfs VW, Lauener PA, Blessmann GS. Prevention of recurrent urinary tract infections with immuno-active E. coli fractions: a meta-analysis of five placebo-controlled double-blind studies. Int J Antimicrob Agents 2002;19(6):451–6. [14] Bauer HW, Alloussi S, Egger G, Blumlein HM, Cozma G, Schulman CC. A long-term, multicenter, double-blind study of an Escherichia coli extract (OM-89) in female patients with recurrent urinary tract infections. Eur Urol 2005;47(4):542–8, discussion 548. [15] Albert X, Huertas I, Pereiro II, Sanfelix J, Gosalbes V, Perrota C. Antibiotics for preventing recurrent urinary tract infection in non-pregnant women. Cochrane Database Syst Rev (3):2004. p. CD001209. [16] Riedasch G, Mo¨hring K. Immunisierungstherapie rezidivierender Harnwegsinfekte der Frau. Therapiewoche 1986;6:896–900. [17] Reid G, Bruce RW. Probiotics to prevent urinary tract infections: the rationale and evidence. World J Urol in press. [18] Reid G, Bruce AW, Taylor M. Instillation of Lactobacillus and stimulation of indigenous organisms to prevent recurrence of urinary tract infections. Microecol Ther 1995;23:32–45. [19] Reid G, Charbonneau D, Erb J, et al. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: randomized, placebocontrolled trial in 64 healthy women. FEMS Immunol Med Microbiol 2003;35(2):131–4. [20] Fraga M, Scavone P, Zunino P. Preventive and therapeutic administration of an indigenous Lactobacillus sp. strain against Proteus mirabilis ascending urinary tract infection in a mouse model. Antonie Van Leeuwenhoek 2005;88(1):25–34. [21] Fischetti VA. Bacteriophage lytic enzymes: novel antiinfectives. Trends Microbiol 2005;13(10):491–6. [22] Cheng Q, Nelson D, Zhu S, Fischetti VA. Removal of group B streptococci colonizing the vagina and oropharynx of mice with a bacteriophage lytic enzyme. Antimicrob Agents Chemother 2005;49(1):111–7. [23] Yoong P, Schuch R, Nelson D, Fischetti VA. Identification of a broadly active phage lytic enzyme with lethal activity against antibiotic-resistant Enterococcus faecalis and Enterococcus faecium. J Bacteriol 2004;186(14):4808–12. [24] Langermann S, Mollby R, Burlein JE, et al. Vaccination with FimH adhesin protects cynomolgus monkeys from colonization and infection by uropathogenic Escherichia coli. J Infect Dis 2000;181(2):774–8. [25] Meiland R, Geerlings SE, Langermann S, Brouwer EC, Coenjaerts FE, Hoepelman AI. Fimch antiserum inhibits [26] [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] [37] [38] [39] [40] [41] 243 the adherence of Escherichia coli to cells collected by voided urine specimens of diabetic women. J Urol 2004;171(4):1589–93. Uehling DT, Hopkins WJ, Elkahwaji JE, Schmidt DM, Leverson GE. Phase 2 clinical trial of a vaginal mucosal vaccine for urinary tract infections. J Urol 2003;170(3):867–9. Li X, Mobley HL. Vaccines for Proteus mirabilis in urinary tract infection. Int J Antimicrob Agents 2002;19(6):461–5. Zhao X, Drlica K. Restricting the selection of antibioticresistant mutants: a general strategy derived from fluoroquinolone studies. Clin Infect Dis 2001;33(Suppl. 3): S147–56. Drlica K. Antibiotic resistance: can we beat the bugs? Drug Discov Today 2001;6(14):714–5. Sano M, Takahashi S, Nishimura M, et al. A clinical study on combination therapy of antimicrobial agents for complicated urinary tract infection–with special reference to combination with clarithromycin. Nippon Hinyokika Gakkai Zasshi 1997;88(6):596–604. Vogel F, Naber KG, Wacha H, Shah P, So¨rgel F, Kayser FH, et al. Parenterale Antibiotika bei Erwachsenen. Chemotherapie J 1999;8:2–49. Snydman DR, Jacobus NV, McDermott LA, Lonks JR, Boyce JM. Comparative In vitro activities of daptomycin and vancomycin against resistant gram-positive pathogens. Antimicrob Agents Chemother 2000;44(12):3447–50. Laganas V, Alder J, Silverman JA. In vitro bactericidal activities of daptomycin against Staphylococcus aureus and Enterococcus faecalis are not mediated by inhibition of lipoteichoic acid biosynthesis. Antimicrob Agents Chemother 2003;47(8):2682–4. Fuchs PC, Barry AL, Brown SD. In vitro bactericidal activity of daptomycin against staphylococci. J Antimicrob Chemother 2002;49(3):467–70. Louie A, Kaw P, Liu W, Jumbe N, Miller MH, Drusano GL. Pharmacodynamics of daptomycin in a murine thigh model of Staphylococcus aureus infection. Antimicrob Agents Chemother 2001;45(3):845–51. Woodworth JR, Nyhart Jr EH, Brier GL, Wolny JD, Black HR. Single-dose pharmacokinetics and antibacterial activity of daptomycin, a new lipopeptide antibiotic, in healthy volunteers. Antimicrob Agents Chemother 1992;36(2):318–25. De Bruin MF, Tally FP. Efficacy and safety of daptomycin for the treatment of bacteremia and serious infections due to Gram-positive bacteria. in 4th Decennial International Conference on Nosocomial and Healthcare-Associated Infections, 2000 Vol. Abstract 594, 2000. Rubinstein E, Vaughan D. Tigecycline: a novel glycylcycline. Drugs 2005;65(10):1317–36. Kumamoto Y, Tsukamoto T, Matsukawa M, et al. Comparative studies on activities of antimicrobial agents against causative organisms isolated from patients with urinary tract infections (2002). I. Susceptibility distribution. Jpn J Antibiot 2004;57(3):246–74. Heinzl S. Neue Antibiotika Chemotherapie Journal 2005;14:54–7. Jones RN, Sader HS, Fritsche TR. Comparative activity of doripenem and three other carbapenems tested against 244 [42] [43] [44] [45] european urology 49 (2006) 235–244 Gram-negative bacilli with various beta-lactamase resistance mechanisms. Diagn Microbiol Infect Dis 2005; 52(1):71–4. Henry Jr DC, Bettis RB, Riffer E, et al. Comparison of oncedaily extended-release ciprofloxacin and conventional twice-daily ciprofloxacin for the treatment of uncomplicated urinary tract infection in women. Clin Ther 2002;24(12):2088–104. Wagenlehner FM, Kinzig-Schippers M, Tischmeyer U, Wagenlehner C, Sorgel F, Dalhoff A, Naber KG. Pharmacokinetics of ciprofloxacin XR (1000 mg) versus volunteers receiving a single oral dose. Int J Antimicrob Agents 2005;Dec 9, [Epub ahead of print]. Talan DA, Naber KG, Palou J, Elkharrat D. Extendedrelease ciprofloxacin (Cipro XR) for treatment of urinary tract infections. Int J Antimicrob Agents 2004;23(Suppl. 1):S54–66. Rubinstein E. History of quinolones and their side effects. Chemotherapy 2001;47(Suppl. 3):3–8, discussion 44–48. [46] Dalhoff A, Schmitz FJ. In vitro antibacterial activity and pharmacodynamics of new quinolones. Eur J Clin Microbiol Infect Dis 2003;22(4):203–21. [47] Eschenburg S, Priestman MA, Abdul-Latif FA, Delachaume C, Fassy F, Schonbrunn E. A novel inhibitor that suspends the induced fit mechanism of UDP-N-acetylglucosamine enolpyruvyl transferase (MurA). J Biol Chem 2005;280(14):14070–5. [48] Kaatz GW. Inhibition of bacterial efflux pumps: a new strategy to combat increasing antimicrobial agent resistance. Expert Opin Emerg Drugs 2002;7(2):223–33. [49] Heinisch L, Wittmann S, Stoiber T, Scherlitz-Hofmann I, Ankel-Fuchs D, Mollmann U. Synthesis and biological activity of tris- and tetrakiscatecholate siderophores based on poly-aza alkanoic acids or alkylbenzoic acids and their conjugates with beta-lactam antibiotics. Arzneimittelforschung 2003;53(3):188–95. [50] Neu HC. The crisis in antibiotic resistance. Science 1992;257(5073):1064–73.