Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
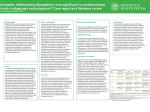
Infectious Myositis Secondary to Multidrug-Resistant Gram Negative Rods in Cancer Patients Nobuyoshi Mori, MD1, 2, Polly Williams, BS, MT(ASCP)1, Karen Vigil, MD2, Jeffrey Tarrand, MD1, Zhi-Dong Jiang, MD, PhD3, Herbert DuPont, MD, FIDSA2, 3, Javier Adachi, MD, FIDSA1, 2, 3 1 The University of Texas MD Anderson Cancer Center, 2 The University of Texas Health Science Center at Houston Medical School, 3 The University of Texas Health Science Center at Houston School of Public Health Abstract Background: Severe infections caused by multidrug-resistant gram negative rods (MDR-GNRs) are increasing healthcare problem worldwide, especially in immunocompromised patients. Infectious myositis is a primary infection of skeletal muscles, usually secondary to gram-positive bacteria, especially Staphylococcus aureus. Although myositis secondary to GNRs are uncommon, several cases secondary to Escherichia coli have been reported in cancer patients. Objectives: To describe the microbiological and clinical characteristics of infectious myositis secondary to MDR-GNRs in cancer patients. Methods: From January 2009 to December 2013 we retrospectively reviewed clinical isolates to identify cases of myositis secondary to MDRGNRs. The diagnosis of infectious myositis was based on clinical presentation (fever and/or pain in the involved muscle), confirmed by compatible radiologic findings and/or muscle biopsy. MDR-GNRs were defined by presence of ESBL or resistance to ≥ 3 of 4 groups (3rd-4th generation cephalosporins, carbapenems, piperacillin/tazobactam and/or quinolones). Resistance to carbapenems alone was also criteria for Carbapenem-Resistant Enterobacteriaceae (CRE) and MDRPseudomonas. Results: Seventeen cases of MDR-GNRs myositis were identified. Median age was 51 y.o. (10 - 83), with 14:3 male to female ratio. All patients had hematological malignancies (65% AML) and severe neutropenia, with 65% involvement of lower extremities. E. coli (47%) was the leading cause, followed by Klebsiella pneumoniae (24%), Enterobacter species (18%), Pseudomonas aeruginosa (6%) and Stenotrophomonas maltophilia (6%). Among 15 Enterobacteriacea isolates, 27% were CRE and 73% produced ESBL. 88% were diagnosed based on positive blood culture and imaging studies, and the remaining 12% were based on muscle biopsy. 82% received active combination antimicrobial therapy, whereas 18% had active single therapy. Only one patient (6%) expired. Conclusion: Infectious myositis secondary to MDR-GNRs has emerged as a serious problem among neutropenic patients with hematologic malignancy. Awareness of this emerging infection and causative organisms are essential to ensure early and appropriate therapy, to achieve the best possible clinical outcome. Materials and Methods Retrospective review of clinical isolates to identify cases of myositis secondary to MDR-GNRs at University of Texas MD Anderson Cancer Center (MDACC) from January 2009 to December 2013 Diagnosis of infectious myositis was based on: • Clinical presentation (fever and/or pain in the involved muscle) and • Confirmation by compatible radiologic findings (edema and/or inflammation in the muscle tissue by CT, MRI or ultrasound) and/or • Muscle biopsy MDR-GNRs were defined as follows: • Presence of ESBL (Extended-Spectrum-B-Lactamase); • Resistance to carbapenems alone; or • Resistance to 3 or more of the following antibiotics: 1. 3rd-4th generation cephalosporins 2. Carbapenems 3. Piperacillin/tazobactam 4. Fluoroquinolones Results 17 cases of infectious myositis secondary to MDR-GNRs Table 1: Demographics Background Age, y, median (range) 51 (10 – 83) Sex, male: female ratio 14 : 3 Severe infections caused by multidrugresistant gram negative rods (MDR-GNRs) are important healthcare problem worldwide, especially in immunocompromised patients [13]. Infectious myositis is a primary infection of skeletal muscles, usually secondary to grampositive bacteria, especially Staphylococcus aureus. [4-6] Although infectious myositis secondary to GNRs are uncommon, several cases caused by Escherichia coli have been reported in cancer patients. [7] Country, USA vs out of USA 14 : 3 Underlying malignancy 83 (100) Objectives To describe the microbiological and clinical characteristics of infectious myositis secondary to MDR-GNRs in cancer patients. Hematologic 17 (100) Solid 0 (0) Matched unrelated donor 6% 6% 6% 65% 5 AML ALL CML Lymphoma Myeloma 17% 3 2 1 0 < 14 14 to 30 > 60 days 30 to 60 • Duration (days), median (range): 38 (5 – 150) • ANC nadir (/mm3), median (range): 0 (0 – 200) Table 2: Clinical Manifestations No. (%) Fever 14 (82) Muscle pain 17 (100) Table 3: Diagnosis No. (%) Upper extremity 5 (30) Lower extremity 10 (59) Blood culture 15 (88) Both extremities 1 (6) Muscle biopsy 2 (12) Others (neck) 1 (6) Imaging study 16 (94) Concomitant abscess 5 (30) MRI 12 (71) Sepsis* 9 (53) CT 3 (18) Severe sepsis** 8 (47) Ultrasound 1 (6) Figure 3: Microbiology 16% 25% E. coli P. aeruginosa 24% E. cloacae 2 1 GvHD 1 S. maltophilia 35% Table 4: Management Neutropenia 16 (94) Admission within 1 month prior to diagnosis 17 (100) ID consult 17 (100) Antibiotic use within 1 month prior to diagnosis 17 (100) Active therapy 17 (100) Corticosteroid use within 1 month prior to diagnosis 15 (88) High dose 4 (24) Low 11 (64) 17 (100) 11 (73%) K. pneumoniae ESBL Carbapenem resistant enterobacteriacea (CRE) No. (%) Combination therapy 15 (88) Single therapy 2 (12) Duration, median (range) 28 (14 – 63) Intervention 4 (80) Seventeen cases of MDR-GNRs myositis were identified. Median age was 51 (10 - 83), with 14:3 male to female ratio. All patients had hematological malignancies (65% AML) and 94% had severe neutropenia, with 65% involvement of lower extremities. E. coli (47%) was the leading cause, followed by Klebsiella pneumoniae (24%), Enterobacter species (18%), Pseudomonas aeruginosa (6%) and Stenotrophomonas maltophilia (6%). Among 15 Enterobacteriacea isolates, 27% were CRE and 73% produced ESBL. 88% were diagnosed based on positive blood culture and imaging studies, and the remaining 12% were based on muscle biopsy. 30% had concomitant abscess formation. 82% received active combination antimicrobial therapy, whereas 18% had active single therapy. Median duration of therapy was 28 days. Among 5 patients with abscess formation, 80% underwent drainage or aspiration. Only one patient (6%) expired. Myositis secondary to MDR-GNRs has emerged as a serious problem among neutropenic patients with hematologic malignancy. Awareness of this emerging infection and causative organisms are essential to ensure early and appropriate therapy, improving the clinical outcome. 4 (27%) 6% Results Conclusions Figure 3-1: Enterobacteriacea 3 (18) Haploidentical Central venous catheter insertion 4 *Sepsis: ≥2of: HR>90, RR>20, BT>38 or <36, WBC>1,2000 or <4000 **Severe sepsis: with hypotension responsive to fluid boluses No. (%) Stem cell transplant Figure 2: Duration of neutropenia Figure 1: Type of Cancer Table 5: Outcome No. (%) Relapse within 3 months 0 (0) Renal failure 4 (24) ICU stay, infection-related 2 (12) Drainage tube placement 1 Mortality, overall 1 (6) Aspiration 3 Mortality, infection-related 1 (6) Future Steps Perform virulence factor, molecular and genomic study to analyze the risk factor for causing infectious myositis in cancer patients. References 1) Kallen AJ, et al. Current Epidemiology of Multidrug-Resistant Gram-Negative Baccili in the United States. Infect Control Hosp Epidemiol. 2010 Nov;31 Suppl 1:S51-4. 2) Romberg PR, et al. Summary trends for the Meropenem Yearly Susceptibility Test Information Collection Program: a 10-year experience in the United States (1999-2008). Diagn Microbiol Infect Dis. 2009 Dec;65(4):414-26. 3) Gudiol C, et al. Changing Aetiology, Clinical Features, Antimicrobial Resistance, and Outcomes of Bloodstream Infection in Neutropenic Cancer Patients. Clin Microbiol Infect. 2013 May;19(5):474-9 4) Ansaloni L. Tropical pyomyositis. World J Surg. 1996 Jun;20(5):613-7. 5) Chiedozi LC. Pyomyositis. Review of 205 cases in 112 patients. Am J Surg. 1979 Feb;137(2):2559. 6) Christin L, et al. Pyomyositis in North America: case reports and review. Clin Infect Dis. 1992 Oct;15(4):668-77. 7) Vigil KJ, Adachi JA, et al. Escherichia coli Pyomyositis: an emerging infectious disease among patients with hematologic malignancies. Clin Infect Dis. 2010 Feb 1;50(3):374-80.