Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Drug discovery wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Prescription costs wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Discovery and development of direct Xa inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Psychopharmacology wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
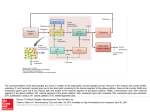
Jack DeRuiter, Principles of Drug Action 2, Fall 2004 GABAMINERGIC NEUROTRANSMISSION: INTRODUCTION 1. Introduction The CNS contains uniquely high concentrations of certain amino acids, notably glutamate and gamma-aminobutyric acid (GABA). The dicarboxylic amino acids (e.g. glutamate, aspartate) mediate excitatory responses while the monocarboxylic acids (GABA, glycine) mediate inhibitory stimuli. Several therapeutic classes have, in recent years, been found to elicit their pharmacologic and therapeutic effects by modulating neurotransmission in the CNS of these amino acid neurotransmitters. It is generally believed that the overall excitability of the CNS is modulated by balanced physiologic activity of two amino acid neurotransmitters, (gamma-aminoglutamic acid (inhibitory) and glutamic acid (excitatory). Glycine, a second inhibitory amino acid neurotransmitter, is primarily localized in the brainstem and spinal cord. Hence, drugs that depress CNS excitability such as the sedative/hypnotics and anxiolytics may do so by (1) enhancing/facilitating GABA neurotransmission or (2) reducing/interfering with glutamate neurotransmission. Drug actions that could theoretically achieve a GABAmimetic/minerigc response include (1) stimulants of biosynthesis and/or release, (2) GABA receptor agonists and (3) inhibitors of GABA metabolism. 2. GABA Receptors: GABAA receptors: A ligand gated receptor. Stimulation results in increased permeability to Cl- raising the postsynaptic membrane threshold potential (inhibitory). This receptor is a heterogenous pentamer consisting of various numbers and types of α, β and γ subunits. At least six different αs, three different βs, three different γs and other subunits have been identified. Different types and combinations of subunits confer different pharmacologic properties on different different receptors; i.e. different affinities for BDZs as described in more detail in the Benzodiazepine Chapter GABAA binding sites include: • α subinits: BDZ receptor: Several subtypes characterized including the BZ1 and BZ2 subtypes (see Benzodiazepine Chapter) • β subunits: Involved in binding GABA (GABA receptor) and also involved in the binding of barbiturates and picrotoxin. GABAB receptors: Presynaptic linked to G proteins which increase K+ conductance (hyperpolarization), inhibits voltage-senstive Ca++ channels (inhibition of transmitter release) 1 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 3. GABA Biosynthesis, Storage and Release • GABA is directly biosynthesized from L-glutamate by the action of glutamic acid decarboxylase (GAD). L-glutamate is available from α-ketoglutarate, a product of glucose metabolism. Glucose is a normal nutrient supplied to the CNS via the blood via active transport. • GABA is stored in synaptic vesicles and is released in a Ca++-dependent manner upon depolarization of the presynaptic membrane GABA Biosynthesis and Metabolism: O O Succinic semialdehyde Dehydrogenase NADP+ OO Succinic acid (SA) O GABA GABA Transaminase PLP PLP O - O- H2N O- H Succinic semialdehyde (SSA) O O O Glutamic Acid Decarboxylase O O- O- H2N O - O alpha-ketoglutarate O OL-Glutamate KREBS CYCLE 4. Termination of GABA Neurotransmission • Reuptake into presynaptic terminals and/or surrounding glial cells is the primary mechanism of termination. • GABA catabolism by GABA-transaminase (aminotransferase, GABA-T) occurs once the neurotransmitter is taken up into tissues. The mechanism for this reaction is shown on the next page. The succinic semialdehyde formed from GABA can be oxidized to succinic acid which enters the Krebs cycle and is eventually utilized to synthesize additional GABA supplies (refer to Figure above). • Neuronal uptake of GABA involves highly specific transmembrane transporters as is observed for other neurotransmitters. 2 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 Mechanism of GABA Biosynthesis GAD H N H NH2 O H O HOOC O- L-Glutamate H O O N PLP B N H H2N O H - N H NH2 CO2 BH NH2 H H N H BH N H O O - O- O N N H H N H H H BH H H H2N N + O- O GABA H 3 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 Mechanism of GABA Transamination: Succinic Semialdehyde (SSA) Formation (Termination) GABA-T H NH2 N H O H2N H N H O- B H GABA N PLP O O H - N H NH2 BH OH2 H N H H NH2 H+ H N H O O BH - O- O N N H H NH2 BH H N H H H H + O O N O- Succinic Semialdehyde H 4 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 5. Inhibitors of GABA Biosynthesis: "PLP Trappers" • A number of drugs inhibit the GAD enzyme required for GABA biosythesis. These can be divided into two structural types the hydrazines (hydrazinopropionic acid, allylglycine) and allylglycine derivatives. Currently none of these compounds are used as therapeutic agents in the US. O NHNH2 H2N NH CH2 COOH Hydrazinopropionic Acid CH CH2 CH COOH NH2 Allylglycine N Isonicotinic Acid Hydrazide Hydrazine Inhibitors • Hydrazine mechanism of action: Recognition at the catalytic site of the enzyme and reaction between the drug hydrazine group and the aldehyde moiety of the PLP cofactor. This mechanism is very similar to that described for carbidopa and LAAAD (see Dopamine Biosynthesis Chapter). • Allylglycine mechanism of action: Recognition at the catalytic site of the enzyme which catalyzes the initial steps of the normal reaction, generating a reactive unsaturated iminium species that alkylates the enzyme (similar to that for Vigabatrin as described below). 6. Drug Affecting GABA Release (Indirect GABA-minergic drugs) a. Baclofen (Lioresal, Kemstro) Cl H2N CH2 CH CH2 COOH Baclofen • Baclofen is a structural analog of the inhibitory neurotransmitter gammaaminobutyric acid (GABA) and may exert its effects by stimulation of the GABAB receptor subtype or inhibiting GABA release. While it’s precise mechanism is unknown, baclofen can inhibit both monosynaptic and polysynaptic reflexes at the spinal level, possibly by hyperpolarization of afferent terminals, although actions at supraspinal sites may also contribute to its clinical effect. Baclofen also has CNS depressant properties as indicated by production of sedation with tolerance, somnolence, ataxia and respiratory and cardiovascular depression. 5 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 • Baclofen is used to alleviate spasticity resulting from multiple sclerosis, particularly for the relief of flexor spasms, concomitant pain, clonus and muscular rigidity. It may be of some value in patients with spinal cord injuries and other spinal cord diseases. Baclofen may be used intrathecally to manage severe spasticity of spinal cord origin in patients who are unresponsive to oral baclofen therapy or who experience intolerable CNS side effects at effective doses. When introduced directly into the intrathecal space, effective CSF concentrations are achieved with resultant plasma concentrations 100 times less than those occurring with oral administration. • Baclofen is well absorbed (100%) orally and not metabolized to any significant degree. It is excreted primarily unchanged in the kidney, thus dose adjustment in renal impairment may be necessary!!!! b. Gabapentin (Neurontin) OH H2N O Gabapentin • Gabapentin is a GABA derivative with a lipophilic cyclohexyl group to promote distribution to the CNS. Gabapentin does not interact with GABA receptors, it is not converted metabolically into GABA or a GABA agonist, and it is not an inhibitor of GABA uptake or degradation. It has been proposed that this drug promotes the release of GABA. • Indications: Adjunctive therapy in the treatment of partial seizures with and without secondary generalization in patients > 12 years of age with epilepsy. Also indicated as adjunctive therapy for partial seizures in children 3 to 12 years of age. Unlabeled uses: Tremors associated with multiple sclerosis; neuropathic pain; bipolar disorder; migraine prophylaxis. • Gabapentin displays moderate oral bioavailability (60%) due to its polarity (not first pass, little metabolism occurs!). It displays minimal plasma protein binding (<3%) and CSF concentrations reach about 20% of the corresponding plasma concentrations. (Minimal plasma protein drug interactions!) • Gabapentin is eliminated from the systemic circulation by renal excretion as unchanged drug; it is not appreciably metabolized. Thus dosage adjustment in patients with compromised renal function is necessary. Its elimination half-life is 5 to 7 hours (no significant hepatic component!!!). 6 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 7. GABA Reuptake inhibitors S CH3 H CH3 N N OH S OH O Nipecotic Acid O Tiagabine (GabitrilTM) ♦ Tiagabine developed from observations that nipecotic acid possesses GABA reuptake inhibitory activity. Tiagabine is indicated for the adjunctive therapy for treatment of partial seizures. This drug.reportedly binds to the GABA reuptake protein, thereby blocking GABA uptake into presynaptic neurons and permitting more GABA to be available for receptor binding on the surfaces of post-synaptic cells. This suggests that tiagabine prevents the propagation of neural impulses that contribute to seizures by a GABA-ergic action. Based on in vitro binding studies, tiagabine does not significantly inhibit the uptake of other neurotransmitters (DA, NE, ACh, 5-HT) nor does it have significant affinity for other neurotransmitter receptors. It also lacks significant affinity for sodium or calcium channels. ♦ Good absorption (95% - minimal first pass and peak plasma levels within an hour. Food can reduce Cmax and Tmax ♦ Relatively high plasma protein binding (96%). Competitive plasma protein binding interactions possible (i.e.Valproic acid)!!! ♦ Metabolism: Two metabolic pathways: 1) thiophene ring oxidation (cytochrome P450 3A) leading to the formation of 5–oxo-tiagabine; and 2) glucuronidation. The 5–oxotiagabine metabolite does not contribute to the pharmacologic activity of tiagabine. 5 Equivalent thiophene substituents!!!! S CH3 CH3 N S OH 5 Acid Glucuronidation! O Tiagabine Metabolism 7 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 ♦ Elimination half-life of 7 to 9 hours. The elimination half-life decreased by 50% to 65% in hepatic enzyme-induced patients with epilepsy (carbamazepine, phenytoin, primidone and phenobarbital) compared to uninduced patients with epilepsy. ♦ Approximately 2% of an oral dose of tiagabine is excreted unchanged, with 25% and 63% of the remaining dose excreted into the urine and feces, respectively, primarily as metabolites. ♦ Potential Drugs interactions: Cytochrome inducers and high plasma protein bound drugs! 8. Inhibitors of GABA metabolism: GABA-Transaminase (GABA-T) Inhibitors CH2 CH CH CH2 CH2 NH2 γ-VinylGABA COOH H2N COOH Gabaculine (Experimental) a. Vigabatrin (Vinyl-GABA, Sabril) • Vigabatrin is a second generation antiepileptic which exerts its mechanism of action by increasing brain GABA levels by inhibition of GABA-transaminase-mediated metabolism via suicide inhibition (mechanism-based inhibition): See next page!! • Vigabatrin is a GABA analogue containing an alpha-vinyl group that is critical for expression of activity. Due to its structural similarity to the normal substrate, vigabatrin is recognized at the active site of GABA-T which initiates the transamination reaction. During this reaction a reactive unsaturated iminium species forms which can alkylate the enzyme as shown in the Figure on the next page. Vigabatrin is marketed as a racemate and virtually all of its GABA-T inhibtory activity appears to reside in the S-(+)-enantiomer. • Vigabatrin's mechanism of action may also be attributed to its ability to decrease excitation-related amino acids, aspartate, glutamate and glutamine concentrations in the brain but these same changes do not occur in the CSF. • • • Oral bioavailability: about 90%. Minimal first pass! Distribution: not bound to plasma proteins and distributes into the CSF Metabolism: None (amino acid derivative!!). Also not an inhibitor or inducer or cytochrome isozymes!!!! Eliminated unchanged in the urine (Amino acid derivative): Dose reductions in renal impairment (CrCL <60 mL/min!) • 8 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 Mechanism of Vigabatrin HO 1. Pridoxal Kinase 2. Pyridoxine Phosphate Oxidase OH CH3 H O CH2NH2 N HO OPO 3-- CH 3 Pyridoxine (B6) N Pyridoxal Phosphate (PLP) Cofactor (PLP) binds to Enzyme (GABA-T) PLP Site H2N H Substrate Site H H B N COO- HO PLP Site H Imine Formation between Inhibitor and PLP Substrate Site H H2N COO- HO OPO3CH 3 B H N OPO3- N CH3 N H Vinyl-GABA Inhibitor binds to GABA-T Substrate Site H GABA-Transaminase GABA-Transaminase Initiation of catalysis: Removal of Acidic H PLP Site H2N H PLP Site Substrate Site H BH H2N Formation of reactive species (vinyliminium) N COOOPO3- CH3 N N H H GABA-Transaminase GABA-Transaminase PLP Site H2N H Substrate Site H B N ETC BH HO OPO3CH 3 H N COO- HO H Substrate Site COO- HO Alkylation of enzyme nucleophile by vinyl iminium species OPO3CH3 N H GABA-Transaminase 9 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 9. Inhibitors of GABA metabolism: Succinic Semialdehyde Inhibitors: a. Valproic Acid (Depakote) CH3CH2CH2 - + CH COO Na CH3CH2CH2 Sodium Valproate (Valproic Acid) • Indications: ♦ Epilepsy: For use as sole and adjunctive therapy in the treatment of simple and complex absence seizures and adjunctively in patients with multiple seizure types that include absence seizures; as monotherapy and adjunctive therapy in the treatment of patients with complex partial seizures that occur either in isolation or in association with other types of seizures (divalproex sodium, valproate sodium injection). Valproate sodium injection is indicated as an IV alternative in patients for whom oral administration of valproate products is temporarily not feasible. ØMania (divalproex sodium delayed-release tablets): ♦ Manic episodes associated with bipolar disorder. ♦ Migraine (divalproex sodium delayed-release and extended-release tablets): As prophylaxis of migraine headaches. ♦ Unlabeled uses: May be effective alone or in combination in the treatment of absence, myoclonic, and grand mal seizures. It may also be effective in patients with intractable status epilepticus who have not responded to other therapies (adults: 200 to 1200 mg every 6 hours rectally with phenytoin and phenobarbital; children: 15 to 20 mg/kg). For minor incontinence after ileoanal anastomosis (subchronic administration). • Mechanism of Action: Prolongs the recovery of voltage-gated sodium channnels and thus inhibits neuronal firing, and the T-currents of calcium channels (thalamus). Also reported to inhibit GABA-transaminase (aminotransferase) and succinic semialdehyde dehydrogenase, enzymes involved in the synthesis and degradation of GABA. However, this proposed mechanism of action has been disputed since the concentrations of the drug are reportedly too low for significant enzyme inhibition to occur with therapeutic doses, and increases in synaptosomal GABA are reportedly too small to account for anticonvulsant effects. Valproate also • Valproate products display variable oral bioavailability, and peak plasma levels are attained in 1-8 hrs (formulation dependent). Dependent on product solubility and variable metabolism in patients! • Valproate is highly plasma protein bound (90%) as is typical for most organic acids. Because of its polarity CNS distribution is low (10% of plasma concentration). 10 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 • Metabolism: CYP-mediated oxidation of the propyl side chain(s): 2-propyl-3-ketopentanoic acid, 2-propyl-hydroxypentanoic acids as shown below: • Elimination: 70% of a dose is excreted renally, mainly as glucuronides (t1/2 15hrs) OH CH3CH2CH CH COO CH3CH2CH2 CH3CH2CH2 - CH COOGluc CH3CH2CH2 β-Oxidation (40%) Glucuronidation (30-40%) CH3CH2CH2 CH COO - CH3CH2CH2 Sodium Valproate ω-1 15-20% ω OH CH3CHCH2 CH COO - Further Oxidation (OR) O Further Oxidation (OR) HOOCCH2CH2 CH3CCH2 CH COO • CH COO CH3CH2CH2 CH3CH2CH2 CH3CH2CH2 HOCH2CH2CH2 - CH COO - CH3CH2CH2 Drug Interactions: 1. GI Tract: Adsorbants (Charcoal, bile acid sequestrants) may absorb valproate and reduce it's absorption (anion=cation interactions with quaternary sequestrants) 2. Cytochrome inhibition by valproate may increase levels of other drugs administered concurrently (phenobarbital, phenytoin, carbamazepine, etc. 3. Cytochrome induciton by inducers (rifampin, phenobarbital, phenytoin, carbamazepine) may incerase oxidative clearance of valproate 4. Competitive plasma protein binding: Valproate may displace, or be displaced, by other highly protein bound drugs, especially acids 11 Jack DeRuiter, Principles of Drug Action 2, Fall 2004 12
















![Anti-GABA antibody [5A9] ab86186 Product datasheet 1 Abreviews 1 Image](http://s1.studyres.com/store/data/008296205_1-9b8206993c446f240db0ef9ab99a7030-150x150.png)