Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
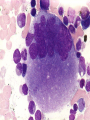
Thrombocytopenia In Intensive Care – Causes and Investigations Lau Ngee Siang Hospital Ampang Conflict of Interest! • NONE! Medscape • Disseminated Intravascular Coagulation Treatment & Management • Author: Marcel M Levi, MD; Chief Editor: Emmanuel C Besa, MD more... • Overview • Presentation • DDx • Workup • Treatment • Medication MEDSCAPE EDUCATION • Guidelines for Managing Thrombocytopenia in the ICU CME • News Author: Emma Hitt, PhD CME Author: Charles P. Vega, MD Definition • < 150 X 109/L. • Severe <50 • Less 30% from baseline???? • • • • Multifactorial Critically ill – marker of severity Higher MODS/APACHE score Inverse correlation with mortality and prolonged ICU stay. • D4 thrombocytopenia correlates with further severity? (some trials data) Dynamics of Platelets in ICU • Most Reducing, D1-D4 (Nadir) – post-op eg: Cardiac/Maj Trauma/Abd Surgery/Vasc Surg/Maj Orth Surg. • >D4 increasing 2-3X of baseline (REBOUND) and peak D14! • ***Intact Physiologic response to PLTs consumption! By MEGAKARYOCYTES! • Acute Consumption - Reduced PLTs – Increased Thrombopoietin – Megakaryocytosis – D3 start to release PLTs >D4 Thrombocytopenia post Surg • D4 thrombocytopenia mortality 33% • D14 thrombocytopenia mortality 66% • Post cardiac surg ICU: Mortality for D4 increasing PLT 1.3% VS D4 PLT<100 12% • >D4 need to determine cause: Infection, drug,… Management of Post-Surg Low PLTS • PLT >50/No Bleeding: Watch only! • On presentation: PLT 50 – 100 with GIT/Retroperitoneal haemorrhage/Acute trauma/Surgery: Loss/Consumption of PLTS! • Need intervention & try keep PLTs >80-100 • Hematocrit >30% • Tranexamic Acid 1g slow bolus and 1g infusion over 8 hours for trauma case (Lancet 2010)???? Thrombosis risk???? Medical ICU Thrombocytopenia • D3 40% <150 • D5 90% <150 • Important to determine cause to treat/manage appropriately • General rules: • 5-7 days slow & gradual: consumptive coagulopathy/marrow failure • 1-2 days Abrupt: Immunologic causes/ drug induced immune thrombocytopenia/adverse transfusion reaction (post-transfusion purpura/passive allo-immunization) ?Medical dynamic Medical Low PLTs • Most common cause:???? YOU KNOW!!!!! • PLTs < 50, DIC is frequently present! • Worseing PLT count – worsening underlying disease – MOF & Consumptive Coagulopathy DIC – Clinical & Lab Definition Thrombosis & Thrombocytopenia • • • • • • Mostly moderate thrombocytopenia Severe PE TTP/HUS Catastrophic APS (venous & arterial) HIT (if Heparin within last 10 days) DKA (arterial) PLT<20 • What’s next? • Consider the cause (Marrow failure, PE, TTP, ITP, Sepsis) • KIV Urgent FBP!!! • Pseudothrombocytopenia! (GPIIb/IIIa inhibitor inducerd?) • Give PLTs: May be diagnostic • If marrow failure: PLTs ++. If immunemediated PLTs_____. (1 hour post) Important Thrombocytopenia causes • TTP – PE • ITP • HIT – Related to Anti PF4-Heparin Complexes. Use Direct Thrombin Inhibitor (Lepirudin, Argatroban) or Heparanoid (Danaparoid) TTP blood film J Suriar 2012 PLT<20 • New rapid (after D4): Often immune mediated (Refer Chart) • GP Ilb/llla inhibitor in cardiac (within 10days) • Drug dependant (10 days) • Transfused BACTERIA contaminated product: PLT>PC>FFP • Post transfusion purpura (rare) • Transfusion induced alloimmune low PLT Case Study • A Splenic Marginal Zone Lymphoma with bulky splenomegaly, failed chemotherapy (R-CHOP & RICE). - Marrow: Infiltration, relatively preserved haemopoiesis. • Proposed splenectomy! Main bulk of disease! • Intro-op: Bleeding: 5L Blood loss! DIC. PLT post transfusions 30-50. Second look Surgery: 2L blood clots! (Pre-op PLT 80-100) • Prolonged PT/APTT & low fibrinogen. Management of DIC • Treat the underlying cause • Stabalize haemodynamically • Manage clinically with the assistance of laboratory support • Blood product as per necessary Role of antifibrinolytic Thank You