Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Plateau principle wikipedia , lookup
Pharmacognosy wikipedia , lookup
Psychopharmacology wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Theralizumab wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Neuropharmacology wikipedia , lookup
Medroxyprogesterone acetate wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
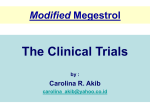
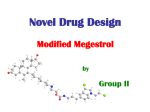
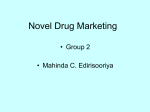
Biodrugs 2005; 19 (3): 179-187 1173-8804/05/0003-0179/$34.95/0 DRUG DELIVERY 2005 Adis Data Information BV. All rights reserved. The Science of Megestrol Acetate Delivery Potential to Improve Outcomes in Cachexia Robert A. Femia1 and Richert E. Goyette2 1 2 Scientific and Regulatory Affairs, Par Pharmaceutical, Inc., Spring Valley, New York, USA Consultant, Hematology/Oncology, Knoxville, Tennessee, USA Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179 1. Progesterone Physiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 1.1 Secretion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 1.2 Modulation of Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 1.3 Metabolic Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 2. Pharmacodynamics of Megestrol Acetate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 2.1 General Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181 2.2 Anticytokine Properties of Megestrol Acetate in Cachexia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182 2.3 Orexigenic Effects of Megestrol Acetate in Cachexia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182 3. Tolerability of Megestrol Acetate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183 4. Pharmacokinetics of Megestrol Acetate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183 4.1 General Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183 4.2 Megestrol Acetate Tablets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184 4.3 Megestrol Acetate Oral Suspension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184 5. Megestrol Acetate Nanocrystal Oral Suspension . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184 5.1 Preclinical Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185 6. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 185 Abstract Cachexia, usually defined as the loss of >5% of an individual’s baseline bodyweight over 2–6 months, occurs with a number of diseases that includes not only AIDS and advanced cancer but also chronic heart failure, rheumatoid arthritis, chronic obstructive pulmonary disease, Crohn disease, and renal failure. Anorexia is considered a key component of the anorexia-cachexia syndrome. Progestogens, particularly megestrol acetate, are commonly used to treat anorexia-cachexia. The mechanism of action of megestrol is believed to involve stimulation of appetite by both direct and indirect pathways and antagonism of the metabolic effects of the principal catabolic cytokines. Because the bioavailability of megestrol acetate directly affects its efficacy and safety, the formulation was refined to enhance its pharmacokinetics. Such efforts yielded megestrol acetate in a tablet form, followed by a concentrated oral suspension form, and an oral suspension form developed using nanocrystal technology. Nanocrystal technology was designed specifically to optimize drug delivery and enhance the bioavailability of drugs that have poor solubility in water. Megestrol acetate nanocrystal oral suspension is currently under review by the US FDA for the treatment of cachexia in patients with AIDS. Preclinical pharmacokinetic data suggest that the new megestrol acetate formulation has the potential to significantly shorten the time to clinical response and thus may improve outcomes in patients with anorexia-cachexia. 180 Femia & Goyette Progestational agents are used to treat the anorexia-cachexia syndrome and sometimes as salvage agents to treat hormonesensitive breast cancer and cancers of the endometrium, ovary, prostate, and other organs. Because oral progesterone is poorly absorbed, the agent is usually delivered intramuscularly in an oil carrier. Megestrol acetate (Megace 1, Par Pharmaceutical, Inc., Spring Valley, NY, USA), a synthetic progestogen currently available in tablet and suspension form, has physiologic activity similar to the natural hormone. First used in humans in 1968, megestrol acetate tablets became commercially available in the US in 1971 for the treatment of endometrial carcinoma. Since that time, megestrol acetate has been used as a component of oral contraceptive pills and in the treatment of malignant and nonmalignant conditions such as melanoma; cancers of the ovary, breast, kidney, and prostate; benign prostatic hypertrophy; and endometrial hyperplasia.[1] Cachexia is a condition of starvation characterized by depletion of muscle mass and, to a lesser extent, adipose tissue. Etymologically, cachexia is derived from ‘kakos’ and ‘hexis’—Greek words meaning ‘bad condition’.[2] Although there are various definitions of cachexia in the medical literature, it commonly refers to an involuntary loss of approximately ≥5% of an individual’s baseline bodyweight over a defined period, usually 2–6 months. Cachexia develops in approximately one half of patients with cancer, and when it does, it can substantially shorten survival time.[2] It is often associated with other debilitating symptoms such as chronic nausea, asthenia and weakness, autonomic failure, cognitive impairment, psychologic distress, and poor/unsatisfactory quality of life.[3] Tissue changes associated with cachexia predispose patients to other comorbidities; for example, insufficient nutrition and loss of fatty hip pads in patients with cachexia increase the risk of hip CNS ct re nic ige ex Di Or CH3 TNF IL-6 IL-1 C=O CH3 Anti-TNF Anti-IL-6 Anti-IL-1 CH3 OCOCH3 H H H O= CH3 Muscle tissue Megestrol acetate Patient with cachexia Fatty tissue Fig. 1. The mechanism of action of megestrol acetate in anorexia/cachexia. IL = interleukin; TNF = tumor necrosis factor. 1 The use of trade names is for product identification purposes only and does not imply endorsement. 2005 Adis Data Information BV. All rights reserved. Biodrugs 2005; 19 (3) Enhancing Megestrol Acetate Delivery for Cachexia 181 CH3 fractures due to falls, and compromise patients’ ability to retain body heat.[4] The word cachexia often evokes the image of a patient with advanced cancer or a disadvantaged individual with extensive protein-calorie malnutrition in a Third World nation; however, cachexia is common in devloped countries and in patients with diseases other than cancer. Cachexia is a manifestation of AIDS, chronic heart failure, rheumatoid arthritis, chronic obstructive pulmonary disease, Crohn disease, chronic renal disease, and other chronic disorders.[2,5-10] Anorexia is a key component of cachexia, and accumulating data suggest that the anorexia-cachexia syndrome is a cytokinederived process manifested by loss of appetite and cytokine-driven hypercatabolism.[11] Megestrol acetate is commonly used to treat anorexia-cachexia and is the only FDA-approved treatment of cancer- and AIDS-related anorexia-cachexia syndrome. Other less common interventions include dronabinol, glucocorticoids, anabolic steroids, antiserotonergic drugs, and prokinetic medications.[12] Until recently, the mechanism of action of megestrol acetate in anorexia-cachexia was poorly understood, but it is now believed that megestrol acetate acts by stimulating appetite, by both direct and indirect mechanisms, and by antagonizing the metabolic effects of the main or most relevant catabolic cytokines (figure 1). Since the efficacy and safety of megestrol acetate is directly linked to the drug’s bioavailability,[13] this article reviews the science of megestrol acetate delivery and describes recent advances in the therapeutic area, focusing on the numerous metabolic effects of physiologic levels of progesterone and the specific effects of pharmacologic amounts of the hormone on processes associated with cachexia. 1. Progesterone Physiology 1.1 Secretion Progesterone is a naturally occurring steroid hormone secreted by the ovary, testes, placenta, and adrenal gland.[14] In menstruating women, endogenous progesterone is secreted from the ovarian follicle just before ovulation and thereafter from the corpus luteum, with concentrations peaking approximately 7 days after ovulation. If a fertilized ovum does not implant, progesterone concentrations fall to basal levels immediately prior to menstruation.[14] Progesterone has a variety of physiologic activities in the reproductive tract, mammary gland, and central nervous system that are beyond the scope of this article. 2005 Adis Data Information BV. All rights reserved. C=O CH3 CH3 OCOCH3 H H H O= CH3 Fig. 2. Chemical structure of megestrol acetate. 1.2 Modulation of Activity Progesterone enters the cell by passively diffusing through the plasma membrane.[14] The actions of the hormone are mediated by binding to progesterone receptor (PR)-A and -B, which are isoforms of the progesterone nuclear factor (NF) receptor coded by a single PR gene. Unligated, the PR isoforms exist as monomers bound to heat shock proteins. These proteins dissociate after binding, and the receptors are phosphorylated and dimerize as either homodimers or heterodimers. These dimers subsequently bind to progesterone response elements on various target genes and, through steps involving transcriptional activators and coactivators and proteins with histone deacetylase activity, chromatin is remodeled and general transcription factors become accessible to transcription proteins such as RNA polymerase II. The biologic activities of PR-A and -B are a function of the target genes. However, PR-A generally acts as a transcriptional inhibitor and PR-B as a stimulator of other steroid response elements. Although the major activities of progesterone are mediated genomically, some nongenomic mechanisms are also operative.[14] 1.3 Metabolic Activity Progesterone exerts myriad metabolic effects on carbohydrate and lipid metabolism.[14] Although the hormone does not alter glucose tolerance, it increases basal insulin levels and the insulin response to carbohydrate load. It also stimulates the activity of lipoprotein lipase and may enhance fat deposition and alter plasma lipids and lipoprotein levels, but the physiologic consequences of the latter effect are unknown. Progesterone also modulates body temperature. Elevated levels of progesterone raise core temperatures after ovulation, presumably through the temperature regulatory activity of the hypothalamus.[14] 2. Pharmacodynamics of Megestrol Acetate 2.1 General Characteristics Megestrol acetate is a synthetic derivative of naturally occurring progesterone, chemically designated 17α-(acetoxy)-6-methylpregna-4,6-diene-3,20-dione (figure 2).[15] A white, Biodrugs 2005; 19 (3) 182 Femia & Goyette crystalline solid, megestrol acetate is delivered in both tablet and suspension form. The suspension is generally preferred over the tablet because it has significantly greater bioavailability as well as a lower cost, which tends to improve adherence.[12] Considerable evidence demonstrates the efficacy of megestrol acetate in the treatment of cachexia, the key characteristics of which are decreased appetite and low bodyweight.[16,17] Megestrol acetate significantly increases both appetite and bodyweight. In doses ranging from 160 to 1600 mg/day, megestrol acetate has been shown to stimulate appetite, increase caloric intake, induce a sense of wellbeing, and produce weight gain (for details see review in Drugs[18]). Weight gain occurs predominantly in the form of fat, which is potentially beneficial because the caloric stores in fatty tissue provide more kilocalories per gram than similar amounts of either protein or carbohydrate (i.e. 9.0 kcal vs 4.0 kcal and 4.0 kcal, respectively). Fat also helps stabilize core body temperatures and protects bony tissue; for example, the fat pads in the hips can help protect debilitated patients from hip fractures secondary to falls. The benefits of megestrol acetate are dose related. Although dosages up to 1600 mg/day of megestrol acetate have been used, the drug’s effects on anorexia-cachexia tend to plateau at 800 mg/ day.[18] Thus, current recommendations are that treatment be titrated from 160 mg/day (40mg four times daily) up to 800 mg/day according to clinical response.[18-20] 2.2 Anticytokine Properties of Megestrol Acetate in Cachexia The principal cytokines involved in cachexia include tumor necrosis factor (TNF)-α, interleukin (IL)-1, IL-6, and interferon (IFN)-γ.[2] TNF-α is believed to work through numerous mechanisms to produce much of the severe cachexia that occurs in patients with chronic infections and cancer.[21] At low concentrations (≤1 U/mL) in C2C12 myotubes in cell culture, TNF-α has been shown to exert a clearly catabolic effect, decreasing both total and myofibrillar protein content.[22] Additional data suggest TNF-α and other inflammatory cytokines contribute to muscle wasting through inhibition of myogenic differentiation via an NFκB-dependent pathway.[23] TNF-α also increases levels of mitochondrial uncoupling proteins, thus providing an energy sink,[24,25] and it inhibits lipoprotein lipase activity and directly stimulates lipolysis.[26] Both IL-6 and IL-1 interact with other cytokines in the development of cachexia. In nude mice transplanted with human cachexiainducing tumors, administration of a monoclonal antibody to IL-6 either essentially abrogated weight loss or resulted in a net weight gain.[27] Binding of IL-1 to its receptors induces a variety of effects 2005 Adis Data Information BV. All rights reserved. within the central nervous system and liver, including anorexia, acute-phase protein synthesis, and downregulation of hepatic production of albumin and other ‘housekeeping’ proteins. Some of the anorexigenic effects of IL-1 are due to the ability of the cytokine to stimulate leptin release, an effect that is blocked by administration of soluble IL-1 receptor.[28] Megestrol acetate appears to have direct anticytokine properties. The drug significantly antagonizes the effects of cytokines such as TNFα, IL-6, and IL-1. In patients with cancer, megestrol acetate has been shown to significantly reduce serum levels of IL-1α and β and reduce IL-6 production in peripheral blood mononuclear cells.[29,30] In humans, anti-IL-6 monoclonal antibody therapy has been shown to decrease the incidence of cancer-related anorexia/cachexia.[31] Experimentally, in Naval Medical Research Institute (NMRI) mice, megestrol acetate has been shown to prevent the weight loss induced by TNF-α and a cachexia-inducing tumor (MAC-16).[32] In patients with advanced metastatic cancer, the drug has been shown to reverse anorexia and weight loss associated with IFNα- and IL-2-based therapies.[33] 2.3 Orexigenic Effects of Megestrol Acetate in Cachexia The mechanisms of anorexia-cachexia are complex. The disorder appears to be associated with disruption in a number of neurohumoral orexigenic signaling pathways including hypothalamic neuropeptides and possibly melanocortin signaling. Physiologically, low plasma levels of leptin, a hormone of adipocyte origin associated with loss of body fat, increase orexigenic signals within the hypothalamus, decrease neurohormonal anorexigenic signals, and suppress energy expenditures.[11,12,34-36] Cytokines may contribute to the anorexia component of the anorexia-cachexia syndrome by stimulating the expression and release of leptin or mimicking the hypothalamic effects of excess leptin on orexigenic neuropeptides such as neuropeptide Y, galanin, opioids, melaninconcentrating hormone, orexin, and agouti-related peptide.[12] In addition, a disruption in energetics leads to an imbalance in energy intake and expenditure. Megestrol acetate has significant orexigenic properties. Although the precise mechanism of action of megestrol acetate has not been fully elucidated, the drug is believed to alter levels of central neurotransmitters involved in appetite regulation (e.g. neuropeptide Y). This effect may be mediated by modulation of calcium channels in the satiety center of the ventromedial hypothalamus or directly through increased levels of neuropeptide Y. Neuropeptide Y is a 36-amino-acid peptide present in significant amounts in the hypothalamus and other areas of the brain.[36] Acting directly, through a variety of interconnected pathways, Biodrugs 2005; 19 (3) Enhancing Megestrol Acetate Delivery for Cachexia neuropeptide Y stimulates release of other orexigenic neuropeptides and may itself be intrinsically orexigenic.[12] Alterations in endogenous opioid-mediated receptors and response mechanisms have also been implicated in the pathogenesis of anorexia-cachexia.[37] Megestrol acetate has been reported to stabilize declining cerebrospinal fluid levels of β-endorphin in the elderly, as well as to increase plasma and cerebrospinal fluid levels of the appetite-stimulatory neuropeptide Y.[38,39] A direct sex hormone effect may also be operative in megestrol acetate-induced appetite stimulation. Whereas estrogen has been shown to decrease food intake in animal models, progestational agents such as megestrol acetate antagonize this effect.[40] 183 associated with high-dose megestrol acetate therapy and speculate a causative relationship. As previously noted, discontinuation of megestrol acetate is seldom required; however, a few precautions are indicated. For example, in patients with a history of thromboembolic disease or heart disease or a serious risk of fluid retention, megestrol acetate should be administered only after a thoughtful risk-benefit assessment.[46] 4. Pharmacokinetics of Megestrol Acetate 4.1 General Characteristics 3. Tolerability of Megestrol Acetate Megestrol acetate is generally well tolerated, with mild adverse effects that rarely lead to drug discontinuation.[12] However, megestrol acetate can induce thromboembolic phenomena in patients with risk factors for venous thromboembolic disease.[12] This appears to be partly a result of the drug’s ability to increase availability of thrombin receptors on smooth muscle cell membrane and thus markedly potentiate the procoagulant effects of thrombin.[41] A hormone-induced decrease in tissue factor pathway inhibitor may also play a role in the development of venous thromboembolic disease.[42] In addition, progestogens may increase venous distensibility and capacitance, resulting in reduced blood flow and stasis,[43] and are likely to induce breakthrough endometrial bleeding.[12] Nonprogestational effects of megestrol acetate may account for sporadic case reports of Addison disease and exacerbation of glucose intolerance, which appear to be manifestations of the steroid’s intrinsic activity at corticosteroid and glucocorticoid hormone receptors. In this setting, Addison disease results from receptor ligation with either stimulation or blockade, and exacerbations of glucose intolerance is a function of the ability of megestrol acetate to stimulate gluconeogenesis or insulin secretion, or both. In a study of patients treated with megestrol acetate 160–800 mg/day, Loprinzi et al.[44] found that the drug reversibly inhibited the hypothalamic-pituitary-adrenal axis and decreased serum cortisol concentrations. This effect is generally asymptomatic and patients do not acquire Cushingoid symptoms while receiving megestrol acetate. Furthermore, Addisonian crisis requiring abrupt discontinuation of therapy has not been reported despite the widespread use of megestrol acetate for decades. In addition to its glucocorticoid effect, megestrol acetate significantly suppresses plasma levels of estradiol. Wermers et al.[45] have reported two cases of osteoporosis and multiple vertebral fractures 2005 Adis Data Information BV. All rights reserved. Megestrol acetate is absorbed rapidly from the gastrointestinal tract. However, studies in patients given the oral suspension demonstrate considerable variability in the rate and degree of absorption;[47] a factor that may be more significant in patients receiving the tablet formulation. In some patients, absorption is slower, with the more sustained plasma drug levels seen in a 1-compartment model. In others, absorption is rapid, with a 2-compartment-like elimination curve.[47] Megestrol acetate is completely metabolized in the liver to free steroids and the metabolites are conjugated with glucuronic acid. Metabolites account for only 5–8% of the administered dose, which is considered negligible.[15] The major route of drug elimination in humans is renal.[15] The effects of megestrol acetate on weight gain appear to be a function of at least four factors: (i) duration of administration; (ii) patient morbidities; (iii) concomitant medications; and (iv) pharmacokinetic effects, particularly those related to bioavailability. Studies in patients with cancer have shown that weight gain continues with longer duration of therapy.[48,49] In patients with AIDS, absorption of megestrol acetate shows significant interpatient variability,[47] possibly owing to comorbidities such as enteropathy, achlorhydria, and other disorders that alter gastrointestinal tract physiology. Concomitant medications affect megestrol acetate pharmacodynamics; for example, drugs such as azoles affect the rate or extent of megestrol acetate metabolism and thus alter efficacy. According to Graham et al.,[47] the area under the plasma concentration-time curve (AUC) of megestrol acetate was not directly correlated with weight gain; instead, a significant relationship was observed between weight gain and the percentage of the 24-hour administration interval that plasma megestrol acetate levels exceeded 300 ng/mL. That is, at least during the early stages of megestrol acetate therapy, weight gain requires plasma megestrol acetate concentrations >300 ng/mL for ≥40% of a 24-hour administration interval. Alterations in the formulation of megestrol acetate have produced three formulations of drug, a progresBiodrugs 2005; 19 (3) 184 Femia & Goyette sion associated with increased bioavailability and thus improved efficacy in the treatment of anorexia-cachexia. 4.2 Megestrol Acetate Tablets Megestrol acetate was formulated as a tablet requiring administration four times daily.[15] In humans, the rate of excretion of radiolabeled megestrol acetate 4–90mg given in tablet form was 56.5–78.4% (mean 66.4%) in urine and 7.7–30.3% (mean 19.8%) in feces within 10 days of administration. The total recovered radioactivity varied between 83.1% and 94.7% (mean 86.2%). At least part of the radioactivity not found in the urine and feces may have been excreted by respiration as labeled carbon dioxide or held in fat storage.[15] Absorption of megestrol acetate 160 mg/day (40mg tablets given four times daily) varied among 23 healthy male volunteers.[15] Peak plasma drug concentrations (Cmax) after the first 40mg dose ranged from 10 to 56 ng/mL (mean 27.6 ng/mL), and the times to Cmax (tmax) ranged from 1 to 3 hours (mean 2.2 hours). Plasma elimination half-life ranged from 13 to 104.9 hours (mean 34.2 hours). Steady-state plasma drug concentrations with a megestrol acetate 40mg four times daily regimen have not been established.[15] 4.3 Megestrol Acetate Oral Suspension To obviate the need for administration of multiple tablets, a megestrol acetate preparation was formulated as a concentrated oral suspension.[15] Plasma steady-state pharmacokinetics of megestrol acetate oral suspension were evaluated in 10 adult male patients with AIDS and cachexia manifesting as involuntary weight loss >10% from baseline.[47] Patients received oral megestrol acetate 800mg once daily for 21 days, and plasma concentrations were measured up to 48 hours after the last dose on day 21. Data analysis showed that mean ± 1 SD Cmax was 828 ± 513 ng/ mL,[47] and mean AUC0–24h was 11 250 ± 7305 ng•hr/mL, results similar to those reported in the megestrol acetate oral suspension (40 mg/mL) package insert (Cmax 753 ± 539 ng/mL and AUC 10 476 ± 7788 ng•hr/mL).[15] The median tmax was 5 hours. All patients reported an increase in appetite, and 8 of 10 patients gained weight by the end of 3 weeks of treatment.[47] These data underscore the clinical significance of the pharmacokinetic profile of megestrol acetate. The two patients who did not gain weight had the lowest Cmax, trough plasma concentration (Cmin), and AUC in the study. A statistically significant relationship was observed between weight gain and the percentage of the 24-hour administration interval that plasma concentrations of megestrol acetate exceeded 300 ng/mL. No correlation could be made between weight gain and AUC, and investigators suggested that early weight gain can be anticipated when plasma megestrol acetate concentrations exceed 300 ng/mL for at least 40% (10 hours) of a 24-hour administration interval.[47] In another study, megestrol acetate oral suspension 750mg was administered once daily for 14 days in 24 asymptomatic HIVseropositive men. On pharmacokinetic evaluation, the mean Cmax was found to be 490 ± 238 ng/mL and the mean AUC was 6779 ± 3048 ng•hr/mL. The mean Cmin was 202 ± 101 ng/mL, with a median tmax of 3 hours. The mean percentage of fluctuation was 107% ± 40%.[15] The relative bioavailability of megestrol acetate 40mg tablets or oral suspension and the effect of food on the bioavailability of the oral megestrol acetate suspension have not been evaluated.[15] 5. Megestrol Acetate Nanocrystal Oral Suspension Megestrol acetate nanocrystal oral suspension was designed to optimize drug delivery and enhance the performance of drugs with poor water solubility. This megestrol acetate formulation is currently under review by the US FDA for the treatment of cachexia in patients with AIDS.[50] Compared with micronized drug particles, nanocrystalline particles produced with nanocrystal technology have significantly increased surface area per unit mass. The manufacturing process uses a conventional high-energy medial milling technique to process a mixture of megestrol acetate, water, and stabilizers, creating a colloidal dispersion of megestrol acetate Table I. Pharmacokinetic parameters of megestrol acetate in beagle dogs.[51] Four megestrol acetate formulations were given by gavage tube to male beagle dogs (n = 3 per formulation) in fed or fasted state. All data are presented as mean (CV%) Parameter Cmax (ng/mL) tmax (h) Nanocrystal formulation #1 Nanocrystal formulation #2 Oral suspension (BMS) Oral suspension (Par) fed fed fed fed fasted 3777.3 1.67 2209.7 fasted 2875.8 1563.0 fasted 2577.8 339.9 fasted 2180.7 485.0 0.8 3.0 0.5 0.8 2.7 1.0 18.7 AUC0–t (ng•hr/mL) 48 543.6 37 774.2 36 687.9 21 857.7 31 397.2 10 094.3 27 332.1 17 394.9 AUC0–inf (ng•hr/mL) 61 734.9 49 408.9 42 787.7 27 863.6 40 218.7 12 007.11 31 721.0 6948.5 AUC = area under the plasma concentration-time curve; BMS = Bristol-Myers Squibb; Cmax = peak plasma concentration; CV = coefficient of variation; Par = Par Pharmaceutical, Inc.; tmax = median time to Cmax. 2005 Adis Data Information BV. All rights reserved. Biodrugs 2005; 19 (3) Enhancing Megestrol Acetate Delivery for Cachexia 185 Megestrol acetate nanocrystal oral suspension #1, 10 mg/kg Megestrol acetate nanocrystal oral suspension #2, 10 mg/kg Megestrol acetate oral suspension, 10 mg/kg (BMS) Megestrol acetate oral suspension, 10 mg/kg (Par) 2200 2000 1800 Plasma levels (ng/mL) 1600 1400 1200 1000 800 600 400 200 0 0 10 20 30 40 50 60 70 80 Time (h) Fig. 3. Mean plasma megestrol acetate levels in male beagle dogs given megestrol acetate nanocrystal oral suspension formulation #1 (n = 3), megestrol acetate nanocrystal oral suspension formulation #2 (n = 3), megestrol acetate oral suspension by Bristol-Myers Squibb (BMS; n = 3), or megestrol acetate oral suspension by Par Pharmaceutical, Inc. (PAR; n = 3) by oral gavage tube, 1 hour after a high-fat meal. to obtain a mean particle size of <200nm. During milling, aggregation of the nanocrystalline particles is prevented by stabilizing the mixture with hydroxypropyl methylcellulose and docusate sodium. Since the absorption of megestrol acetate is dissolution-rate limited, the nanocrystalline particles increase the rate of absorption and decrease absorption variability when the drug is taken with food. 5.1 Preclinical Pharmacokinetics A study was conducted in 12 male beagle dogs to determine the pharmacokinetic characteristics of megestrol acetate when administered as a 10 mg/kg suspension or colloidal dispersion by oral gavage.[51] The assay was calibrated over the range of 1–512 ng/ mL. The following four formulations were evaluated at a dose of 10 mg/kg: (i) nanocrystal formulation #1; (ii) nanocrystal formulation #2; (iii) megestrol acetate oral suspension manufactured by Bristol-Myers Squibb; and (iv) megestrol acetate nanocrystal oral suspension manufactured by Par Pharmaceutical, Inc. Each product was available in a concentration of 40 mg/mL, so all study treatments were administered in equal volumes by oral gavage to a group of three dogs, first under fasted conditions and then under fed conditions, after a 14-day washout. Before administration on day 1, all dogs were fasted 12–16 hours. On day 14, the dogs were fed a high-fat meal approximately 1 hour before administration, and on days 1 and 14, blood samples were collected pre-administration and at 0.25, 0.5, 1, 2, 3, 4, 6, 8, 24, 48, and 72 hours after administration to determine plasma megestrol acetate concentrations and calculate pharmacokinetic parameters. 2005 Adis Data Information BV. All rights reserved. In the fasted state, the nanocrystal formulations of megestrol acetate produced 4- to 6-fold higher Cmax values >2 hours earlier than the two currently available suspensions (table I). As reflected in the AUC, exposure to the drug was 2- to 4-fold higher with the nanocrystal formulations than with the suspensions, and variability was lower, particularly with nanocrystal formulation #2. Administration after a high-fat meal markedly increased bioavailability; peak concentrations were 5- to 7-fold higher and occurred earlier, and AUC values were 2- to 3-fold higher (figure 3). Although a high-fat meal increased the bioavailability of all formulations, the increase was of a lower magnitude for the nanocrystal formulations, with only 1- to 2-fold higher Cmax and AUC values; however, the resultant concentrations were still higher than those seen with the suspensions. A high-fat meal also raised average tmax values by 1–2 hours. 6. Conclusions Progestational agents have long been used in the treatment of the anorexia-cachexia syndrome, a component of numerous diseases including AIDS, cancer, chronic heart failure, rheumatoid arthritis, chronic obstructive pulmonary disease, Crohn disease, and chronic renal disease. Megestrol acetate, the preferred progestational agent for the treatment of anorexia-cachexia, has been shown to be effective in stabilizing weight loss or even producing weight gain. However, the tablet and oral suspension formulations of the drug are accompanied by pharmacokinetic characteristics that may have limited optimal use. Biodrugs 2005; 19 (3) 186 Femia & Goyette The improved bioavailability of megestrol acetate nanocrystal oral suspension has the potential to address unmet needs in the treatment of anorexia-cachexia. By rapidly increasing plasma megestrol acetate concentrations, this formulation may have the potential to produce a more rapid clinical response and significantly improve outcomes in patients with this common and potentially deadly disorder. Acknowledgments Robert A. Femia is the Executive Vice President, Scientific and Regulatory Affairs for Par Pharmaceutical, Inc. Dr Goyette is not an employee, shareholder, or retained consultant of Par Pharmaceutical, Inc. There is no conflict of interest. References 1. Schacter L, Rozencweig M, Canetta R, et al. Megestrol acetate: clinical experience. Cancer Treat Rev 1989; 16 (1): 49-63 2. Tisdale MJ. Biology of cachexia. J Natl Cancer Inst 1997; 89 (23): 1763-73 3. Strasser F, Bruera ED. Update on anorexia and cachexia. Hematol Oncol Clin North Am 2002; 16 (3): 589-617 4. Akner G, Cederholm T. Treatment of protein-energy malnutrition in chronic nonmalignant disorders. Am J Clin Nutr 2001; 74 (1): 6-24 5. Milani RV, Mehra MR, Endres S, et al. The clinical relevance of circulating tumor necrosis factor-alpha in acute decompensated chronic heart failure without cachexia. Chest 1996; 110 (4): 992-5 6. Ferrari R. The importance of cachexia in the syndrome of heart failure. Eur Heart J 1997; 18 (2): 187-9 7. Roubenoff R, Roubenoff RA, Cannon JG, et al. Rheumatoid cachexia: cytokinedriven hypermetabolism accompanying reduced body cell mass in chronic inflammation. J Clin Invest 1994; 93 (6): 2379-86 8. Lewis MI. Apoptosis as a potential mechanism of muscle cachexia in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2002; 166 (4): 434-6 9. Rigaud D, Angel LA, Cerf M, et al. Mechanisms of decreased food intake during weight loss in adult Crohn’s disease patients without obvious malabsorption. Am J Clin Nutr 1994; 60 (5): 775-81 10. Mitch WE. Robert H Herman Memorial Award in Clinical Nutrition Lecture, 1997: mechanisms causing loss of lean body mass in kidney disease. Am J Clin Nutr 1998; 67 (3): 359-66 11. Inui A. Cancer anorexia-cachexia syndrome: are neuropeptides the key? Cancer Res 1999; 59 (18): 4493-501 12. Inui A. Cancer anorexia-cachexia syndrome: current issues in research and management. CA Cancer J Clin 2002; 52 (2): 72-91 13. Farinha A, Bica A, Tavares P. Improved bioavailability of a micronized megestrol acetate tablet formulation in humans. Drug Dev Ind Pharm 2000; 26 (5): 567-70 14. Loose-Mitchell DS, Stancel GM. Estrogens and progestins. In: Hardman JG, Limbird LE, Gilman AG, editors. Goodman and Gilman’s the pharmacological basis of therapeutics. 10th ed. New York: McGraw-Hill, 2001: 1597-634 15. Par Pharmaceutical. Megestrol acetate oral suspension. Spring Valley (NY): Par Pharmaceutical, Inc., 2004 [online]. Available from URL: http:// www.parpharm.com/downloads/megestroloral_po.pdf [Accessed 2005 Apr 5] 16. Pascual Lopez A, Figuls M, Urrutia Cuchi G, et al. Systematic review of megestrol acetate in the treatment of anorexia-cachexia syndrome. J Pain Symptom Manage 2004; 27 (4): 360-9 17. Tomiska M, Tomiskova M, Salajka F, et al. Palliative treatment of cancer anorexia with oral suspension of megestrol acetate. Neoplasma 2003; 50 (3): 227-33 18. Gagnon B, Bruera E. A review of the drug treatment of cachexia associated with cancer. Drugs 1998; 55 (5): 675-88 19. Mantovani G, Maccio A, Massa E, et al. Managing cancer-related anorexia/ cachexia. Drugs 2001; 61 (4): 499-514 2005 Adis Data Information BV. All rights reserved. 20. Loprinzi CL, Michalak JC, Schaid DJ, et al. Phase III evaluation of four doses of megestrol acetate as therapy for patients with cancer anorexia and/or cachexia. J Clin Oncol 1993; 11 (4): 762-7 21. Beutler B, Cerami A. The biology of cachectin/TNF: a primary mediator of the host response. Annu Rev Immunol 1989; 7: 625-55 22. Alvarez B, Quinn LS, Busquets S, et al. Direct effects of tumor necrosis factor alpha (TNF-alpha) on murine skeletal muscle cell lines: bimodal effects on protein metabolism. Eur Cytokine Netw 2001; 12 (3): 399-410 23. Langen RC, Schols AM, Kelders MC, et al. Inflammatory cytokines inhibit myogenic differentiation through activation of nuclear factor-kappaB. FASEB J 2001; 15 (7): 1169-80 24. Jezek P. Possible physiological roles of mitochondrial uncoupling proteins: UCPn. Int J Biochem Cell Biol 2002; 34 (10): 1190-206 25. Busquets S, Sanchis D, Alvarez B, et al. In the rat, tumor necrosis factor alpha administration results in an increase in both UCP2 and UCP3 mRNAs in skeletal muscle: a possible mechanism for cytokine-induced thermogenesis? FEBS Lett 1998; 440 (3): 348-50 26. Berg M, Fraker DL, Alexander HR. Characterization of differentiation factor/ leukaemia inhibitory factor effect on lipoprotein lipase activity and mRNA in 3T3-L1 adipocytes. Cytokine 1994; 6 (4): 425-32 27. Zaki MH, Nemeth JA, Trikha M. CNTO 328, a monoclonal antibody to IL-6, inhibits human tumor-induced cachexia in nude mice. Int J Cancer 2004; 111 (4): 592-5 28. Francis J, MohanKumar PS, MohanKumar SM, et al. Systemic administration of lipopolysaccharide increases plasma leptin levels: blockade by soluble interleukin-1 receptor. Endocrine 1999; 10 (3): 291-5 29. Mantovani G, Maccio A, Bianchi A, et al. Megestrol acetate in neoplastic anorexia/ cachexia: clinical evaluation and comparison with cytokine levels in patients with head and neck carcinoma treated with neoadjuvant chemotherapy. Int J Clin Lab Res 1995; 25 (3): 135-41 30. Mantovani G, Maccio A, Esu S, et al. Medroxyprogesterone acetate reduces the production of cytokines and serotonin involved in anorexia/cachexia and emesis by peripheral blood mononuclear cells of cancer patients. Biochem Soc Trans 1997; 25 (2): 296S 31. Trikha M, Corringham R, Klein B, et al. Targeted anti-interleukin-6 monoclonal antibody therapy for cancer: a review of the rationale and clinical evidence. Clin Cancer Res 2003; 9 (13): 4653-65 32. Beck SA, Tisdale MJ. Effect of megestrol acetate on weight loss induced by tumour necrosis factor alpha and a cachexia-inducing tumour (MAC16) in NMRI mice. Br J Cancer 1990; 62 (3): 420-4 33. Ackermann M, Kirchner H, Atzpodien J. Low dose megestrol acetate can abrogate cachexia in advanced tumor patients receiving systemic interferon-alpha and/or interleukin-2 based antineoplastic therapy. Anticancer Drugs 1993; 4 (5): 585-7 34. Flier JS. Clinical review 94: what’s in a name? In search of leptin’s physiologic role. J Clin Endocrinol Metab 1998; 83 (5): 1407-13 35. Schwartz MW, Dallman MF, Woods SC. Hypothalamic response to starvation: implications for the study of wasting disorders. Am J Physiol 1995; 269 (5 pt 2): R949-57 36. Schwartz MW, Seeley RJ. Seminars in medicine of the Beth Israel Deaconess Medical Center: neuroendocrine responses to starvation and weight loss. N Engl J Med 1997; 336 (25): 1802-11 37. Morley JE, Silver AJ. Anorexia in the elderly. Neurobiol Aging 1988; 9 (1): 9-16 38. Martinez M, Hernanz A, Gomez-Cerezo J, et al. Alterations in plasma and cerebrospinal fluid levels of neuropeptides in idiopathic senile anorexia. Regul Pept 1993; 49 (2): 109-17 39. Karcic E, Philpot C, Morley JE. Treating malnutrition with megestrol acetate: literature review and review of our experience. J Nutr Health Aging 2002; 6 (3): 191-200 40. Morley JE. Orexigenic and anabolic agents. Clin Geriatr Med 2002; 18 (4): 853-66 41. Herkert O, Kuhl H, Sandow J, et al. Sex steroids used in hormonal treatment increase vascular procoagulant activity by inducing thrombin receptor (PAR-1) expression: role of the glucocorticoid receptor. Circulation 2001; 104 (23): 2826-31 42. Bladbjerg EM, Skouby SO, Andersen LF, et al. Effects of different progestin regimens in hormone replacement therapy on blood coagulation factor VII and tissue factor pathway inhibitor. Hum Reprod 2002; 17 (12): 3235-41 43. Kuhl H. Effects of progestogens on haemostasis. Maturitas 1996; 24 (1-2): 1-19 Biodrugs 2005; 19 (3) Enhancing Megestrol Acetate Delivery for Cachexia 44. Loprinzi CL, Jensen MD, Jiang NS, et al. Effect of megestrol acetate on the human pituitary-adrenal axis. Mayo Clin Proc 1992; 67 (12): 1160-2 45. Wermers RA, Hurley DL, Kearns AE. Osteoporosis associated with megestrol acetate. Mayo Clin Proc 2004; 79 (12): 1557-61 46. Nelson KA. The cancer anorexia-cachexia syndrome. Semin Oncol 2000; 27 (1): 64-8 47. Graham KK, Mikolich DJ, Fisher AE, et al. Pharmacologic evaluation of megestrol acetate oral suspension in cachectic AIDS patients. J Acquir Immune Defic Syndr 1994; 7 (6): 580-6 48. Aisner J, Parnes H, Tait N, et al. Appetite stimulation and weight gain with megestrol acetate. Semin Oncol 1990; 17 (6 Suppl. 9): 2-7 49. Aisner J, Tchekmedyian NS, Moody M, et al. High-dose megestrol acetate for the treatment of advanced breast cancer: dose and toxicities. Semin Hematol 1987; 24 (2 Suppl. 1): 48-55 2005 Adis Data Information BV. All rights reserved. 187 50. Par Pharmaceutical, Inc. FDA accepts for filing Par Pharmaceutical’s NDA for megestrol acetate oral suspension NCD. Press release 2004 Sep 16 [online]. Available from URL: http://www.parpharm.com/html/nf/PR_ 20040916.html [Accessed 2005 Apr 5] 51. Data on file, Par Pharmaceutical, Inc., 2004 Correspondence and offprints: Dr Robert A. Femia, Scientific and Regulatory Affairs, Par Pharmaceutical, Inc., One Ram Ridge Road, Spring Valley, NY 10977, USA. E-mail: [email protected] Biodrugs 2005; 19 (3)