Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
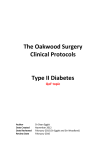
REVIEW Optimal dosing strategies for maximising the clinical response to metformin in type 2 diabetes JOHN HB SCARPELLO Abstract R ecently revised consensus targets for glycaemic management in patients with type 2 diabetes are challenging and require optimisation of dosing strategies for oral antidiabetic therapies. The demonstration of significant cardiovascular outcome benefits in metformin-treated type 2 diabetic patients enrolled in the United Kingdom Prospective Diabetes Study has established this agent as the first line oral therapy after diet failure in newly presenting overweight people with type 2 diabetes mellitus. The antihyperglycaemic efficacy of metformin increases with increasing daily doses between 500 mg and the upper limits of the recommended daily dosage ( ≥ 2000 mg/day). Although metformin is associated with gastrointestinal side-effects in up to 20% of patients, this is not generally dose related. Transient dose reduction, slower titration and taking the dose with meals may ameliorate the problem. Risk of lactic acidosis due to metformin is negligible when this agent is prescribed correctly, and is unrelated to the plasma metformin concentration. Intensification of metformin therapy within the dose range represents a rational and practical therapeutic strategy for optimising glycaemic control in patients who are suitable for, and tolerant of, metformin treatment. The recently introduced 1000 mg metformin tablet should facilitate the use of higher doses and may help treatment compliance. Key words: metformin, oral antidiabetic therapy, type 2 diabetes, dose-response relationships. Introduction The United Kingdom Prospective Diabetes Study (UKPDS) has shown beyond doubt that improving glycaemia in patients with Correspondence to: Dr John Scarpello Department of Diabetes and Endocrinology, City General Hospital, Stoke on Trent, ST4 6QG, UK Tel: +44 (0)1782 553425; Fax: +44 (0)1782 553427 E-mail: [email protected] Br J Diabetes Vasc Dis 2001;1:28–36 28 John Scarpello Table 1. Targets for glycaemic management in Europe and in the USA International Diabetes Federation (Europe)2 American Diabetes Association (USA)3 Fasting plasma glucose HbA1C ≤ 6 mmol/L ≤ 6.5% < 6.7 mmol/L < 7% type 2 diabetes reduces the risk of diabetic complications.1 As a result, challenging new targets for fasting plasma glucose (FPG) and glycated haemoglobin (HbA1C) in patients with diabetes have been agreed for routine clinical practice2,3 (table 1). Meeting these goals requires a new paradigm for the management of the person with type 2 diabetes. An ongoing survey of current standards achieved in routine clinical practice from Salford in the UK has shown that in a population of more than six thousand patients, less than 20% achieved an annual HbA1C < 7.0% over a six-year follow-up period (1993–1998).4 Achieving the new treatment targets requires optimisation of dosing strategies for oral antidiabetic agents, including combined therapies. Maximum dosage of oral antidiabetic therapy in individual patients is frequently limited by the risk-benefit profiles THE BRITISH JOURNAL OF DIABETES AND VASCULAR DISEASE REVIEW ce an ai n Fr Sp l ga rtu UK nd la er Po y an m itz 14% 0 A 21% Sw 41% 7% er 39% US 32% 1000 G 0.19 0.49 0.46 0.11 0.6 8% m 20% iu 0.017 0.011 0.0023 0.01 0.13 36% lg 42% ly p value Be ∆ risk* ria p value Metformin dose - UKPDS a 2000 st ∆ risk* 3000 Au Diabetes-related deaths All cause mortality Any diabetes-related endpoint Myocardial infarction Stroke Sulphonylurea/insulin therapies Metformin daily dose (mg) Metformin therapy Figure 1. Average metformin daily dosage in various countries Ita Table 2. Improved clinical outcomes following intensive glycaemic management with metformin compared with intensive glycaemic management with a sulphonylurea or insulin10 Majority of UKPDS patients allocated metformin received a dosage >2000 mg/day.10 Prescription analysis data (mean doses) kindly supplied by Merck-Lipha a *Compared with conventional therapy based on diet/exercise in overweight patients. of individual therapies, for example weight gain and hypoglycaemia associated with insulinotropic agents.5-7 Metformin is as effective as sulphonylureas,6,8,9 but its risk-benefit profile across the full therapeutic dose range of 500–3000 mg/day is less well described. In the UKPDS, significant improvements in macrovascular outcomes leading to fewer deaths were reported for overweight patients receiving metformin therapy for a median period of 10 years.10 The reduction in morbidity and mortality was much greater than that reported for patients treated with sulphonylureas and insulin despite there being no overall difference in glycaemic control. This landmark clinical trial emphasises the need to optimise therapy with metformin, so that these benefits can be more widely realised. This review explores the dose-relationship of the effects of metformin in patients with type 2 diabetes and summarises the evidence that metformin administered at higher doses provides additional glycaemic control, without the burden of additional side-effects. Optimising oral antidiabetic therapy for type 2 diabetes Benefits of titrating up metformin dose in the United Kingdom Prospective Diabetes Study The reductions in diabetic complications in metformin-treated patients in the UKPDS10 are summarised in table 2. Significant improvements were observed with metformin in all cause mortality (p=0.011), diabetes-related deaths (p=0.017), myocardial infarction (p=0.01) and any diabetes-related end point (p=0.0023). In contrast, no significant changes in these outcomes were observed in patients treated with insulin or a sulphonylurea, despite similar improvements in glycaemic control (table 2). It is important to note that the benefits observed in the UKPDS were achieved at a relatively high dose of metformin. Whilst more than half of the patients in the UKPDS received a daily dosage of 2550 mg/day, more than three quarters of patients received at least 1700 mg/day. The results of the UKPDS VOLUME 1 ISSUE 1 . AUGUST 2001 therefore lend support to the use of metformin at adequately titrated doses in order to improve clinical outcomes in patients with type 2 diabetes. In contrast, evidence from the literature11,12 and from the manufacturer of a branded form of metformin (figure 1) suggests that many patients may not achieve the expected benefit of metformin if it is not titrated to sufficient dosage. (figure 1). Dose-relationship of the efficacy of metformin in patients with type 2 diabetes Most large clinical trials with metformin have employed pragmatic study designs, with a flexible dose titration phase followed by a period of long-term maintenance treatment.8-10 While these studies have optimised therapy in their patient populations, within the dose ranges employed in each study, they tell us little of the dose-relationship of the effects of metformin per se. Some information about the relationship between the dose and antihyperglycaemic efficacy of metformin in people with type 2 diabetes can be acquired from smaller studies using either parallelgroup designs or titration within individual patients. A double-blind study13 investigated the effects of metformin in 75 patients with established type 2 diabetes and fasting plasma glucose (FPG) ≥ 6 mmol/L, who were randomised to receive placebo or metformin at doses of 1500 mg or 3000 mg for six months. FPG and glycated haemoglobin (HbA1C) increased in placebo-treated patients over the six-month study period (figure. 2). In contrast, metformin significantly reduced both parameters. The higher dose of metformin was significantly more effective in reducing FPG compared with the lower dose (p=0.02). The improvement in mean HbA1C values was 1.8% between patients receiving placebo and the higher dose of metformin (figure 2). A second parallel-group dose-response study14 randomised 451 patients with FPG of at least 10 mmol/L (180 mg/dl) despite prior treatment with diet or sulphonylurea to therapy with metformin at daily doses of 500 mg, 1000 mg, 1500 mg, 2000 mg or 2500 mg for 11 weeks. Statistically significant reductions in 29 REVIEW Figure 2. Effects of two doses of metformin on fasting plasma glucose (FPG) and HbA1C in patients with type 2 diabetes13 FPG 1 HbA1c -0.5 -1 -3 *** FPG (mmol/L) (placebo-corrected) -2 0 -1.5 *** 500 (n=73) 0 Placebo (n=23) Metformin, 1500 mg/day (n=25) Metformin, 3000 mg/day (n=27) Mean changes from baseline are shown. Significance versus placebo: ***p=0.001. Final daily dose of metformin 1500 2000 1000 (n=76) (n=73) (n=73) -2 ** -3 *** -4 *** -5 *** 0 500 (n=73) Final daily dose of metformin 1000 1500 2000 (n=73) (n=76) (n=73) 30 2500 (mg) (n=77) -0.5 -1.0 -1.5 *** *** -2.0 *** *** -2.5 *** Mean placebo-corrected differences from baseline are shown. FPG: fasting plasma glucose. Significance versus placebo: **p<0.01, ***p<0.001. Figure 4. Dose-related effects of metformin during dose titration in patients with type 2 diabetes15 3 dose titration 13 2 dose titration 12 11 FPG (mmol/L) FPG compared with placebo, occurred at doses of 1000 mg and above, with the greatest effects occurring at 2000 mg and 2500 mg/day. HbA1C was improved at all dosages studied. There was a decrease in HbA1C of more than 1.5% at doses of 1500 mg/day and above. Reductions in HbA1C and FPG increased with the dose of metformin up to a dose of 2000 mg which corresponded with reductions of 4.4 mmol/L and 2% respectively (figure 3). At the highest dose, 2500 mg, the net reduction in FPG and HbA1C was not significantly different from 2000 mg, although some individual patients achieved additional glycaemic benefit at the higher dose (figure 3). Two other studies15,16 have evaluated the dose-response relationships of metformin within individual patients during dose titration. One double-blind study included a group of 37 patients with type 2 diabetes (FPG ≥ 6.7 mmol/L after two months of diet therapy) randomised to monotherapy with metformin, given as an initial daily dose of 1000 mg.15 The dose of metformin was increased in two further titration steps, at two-weekly intervals, to a maximum of 3000 mg/day if FPG remained at or above 6.7 mmol/L. Patients were divided into two groups depending on whether the glycaemic target was achieved after three titration steps, or whether only two titration steps were needed. Not surprisingly, the patients requiring more than two titration steps had more severe diabetes at baseline, as indicated by a higher mean FPG (figure 4). In both groups progressive increases in antihyperglycaemic efficacy were observed with each dose increment, including titration to the maximum dose of 3000 mg/day (figure 4). Figure 4 also shows that mean FPG in patients receiving more titration steps remained in excess of 9 mmol/L despite the maximum therapeutic dose of metformin. The observed improvement in glycaemia of between 25–30% is consistent with other metformin studies which have employed doses of up to 3000 mg per day. 8,17,18 It must be noted that it may not be practical to 2500 (mg) (n=77) -1 *** HbA1c (%) (placebo-corrected) -1 -4 1 0.5 (% units) (mmol/L) 0 Figure 3. Effects of metformin administered at doses between 500 and 2500 mg/day on glycaemic parameters in patients with type 2 diabetes14 10 9 8 7 6 0 1000 2000 3000 Metformin daily dose (mg) Mean values of fasting plasma glucose (FPG) are shown. Patients were divided into those able to achieve a glycaemic target of FPG ≤ 6.7 mmol/L after two dose titration steps, and those who required at least three titration steps, as indicated. use the full dose range of metformin particularly if this is unlikely to achieve the glycaemic target. In the latter situation, the dosage should revert to the lowest dose to achieve the maximum effect and consideration given to combination therapy.19 Metformin-based combination therapy has proved to be a rational and effective strategy for enhancing glycaemic control in THE BRITISH JOURNAL OF DIABETES AND VASCULAR DISEASE REVIEW Baseline Metformin 500 mg/day Metformin 1500 mg/day Metformin 3000 mg/day 300 15 FPG (mmol/L) 20 Plasma glucose (mmol/L) Figure 6. Effects of increasing doses of metformin on fasting plasma glucose (FPG, left-hand ordinate) and on 24-hour plasma glucose (right-hand ordinate) in patients with type 2 diabetes16 15 10 * * *† *† 10 *† *† 100 5 5 B L 200 3000 0 500 1500 Daily dose of metformin (mg) D 24-hour plasma glucose (AUC) (mmol.h/l) Figure 5. Mean 24-hour plasma glucose profiles during titration of the dose of metformin in nine patients with type 2 diabetes16 0 0 6 12 18 24 Hours B = breakfast; L = lunch; D = dinner. patients with type 2 diabetes20 and more than 60% of patients in this study switched to metformin-glibenclamide combinations went on to achieve FPG ≤ 6.7 mmol/L. A further study compared the effects on glycaemia of escalating doses of metformin in nine patients with type 2 diabetes.16 The metformin daily dose was commenced at 500 mg and then increased in a stepwise manner at two-weekly intervals to 1500 mg and then 3000 mg. FBG, 24-hour glucose profiles and glucose utilisation rates were evaluated at the end of each two week treatment period. The twenty-four hour glucose profiles demonstrated a clear dose-response relationship, with reduced plasma glucose concentrations with each increase in the dose of metformin (figure 5). Measurements of mean FBG and mean 24-hour plasma glucose, measured as the area under the glucose concentration–time curve, confirm this observation (figure 6). Both parameters were significantly reduced at all metformin doses, compared with baseline (p<0.01). Whilst the 1500 mg and 3000 mg doses of metformin were significantly more effective than the 500 mg dose in reducing both fasting and 24-hour plasma glucose concentrations (p<0.02), the benefits observed with 3000 mg/day were not statistically significantly greater than with 1500 mg/day (figures 5 and 6). Metformin at 3000 mg, but not at lower doses, significantly reduced the magnitude of the plasma glucose excursion following breakfast (p<0.05), although no significant effects of metformin were observed at other meal times. The greater effect of metformin on plasma glucose at higher doses was reflected in an increased rate of glucose utilisation during studies employing the euglycaemic hyperinsulinaemic glucose clamp. Glucose uptake rates at baseline and following treatment with metformin at doses of 500 mg, 1500 mg and 3000 mg were (means ± SEM) 10.3±1.5, 11.1±2.8, 12.7±2.2 and 32 Means + SEM are shown. Significance of results: *p<0.01 versus 0 mg/day; †p<0.02 versus 500 mg/day. AUC: area under the 24-hour plasma glucosetime curve. Figure 7. Dose-relationship of effects of metformin on postprandial glucose in a single-dose study in patients with type 2 diabetes22 4 Postprandial plasma glucose (mmol/L) 0 3 * 2 * 1 0 Placebo 850 1700 2550 Dose of metformin (mg) Means + SEM are shown. Postprandial glucose was measured during the period 1–3 hours after lunch and changes in this parameter are shown relative to fasting plasma glucose; *p<0.05 versus placebo. 13.3±2.4 µmol/kg/min, respectively. Other studies confirm the improvement of postprandial glucose by higher doses of metformin (1500–2550 mg/day).21-24 One of these studies included an evaluation of the effects of different single doses of metformin on postprandial glucose.22 The effect on postprandial glucose increased with increasing dose, achieving statistical significance at doses of 1700 mg and 2550 mg (figure 7). Larger improvements in postprandial glucose were observed following five days of treatment with metformin at a dose of 2550 mg/day. Interestingly, postprandial THE BRITISH JOURNAL OF DIABETES AND VASCULAR DISEASE REVIEW Table 3. Gastrointestinal adverse events and treatment discontinuations for gastrointestinal adverse events in patients receiving different doses of metformin14 Final daily dose of metformin Placebo n=79 Abdominal pain Diarrhoeaa Nausea Dyspepsia Anorexia Combined digestive disturbancesa,b 500 mg n=73 1000 mg n=73 1500 mg n=76 2000 mg n=73 2500 mg n=77 I D I D I D I D I D I D 0% 5% 5% 1% 1% 0% 0% 0% 0% 0% 3% 8% 7% 1% 0% 0% 0% 0% 0% 0% 1% 21% 10% 1% 1% 1% 4% 3% 0% 0% 4% 12% 8% 9% 3% 1% 3% 3% 0% 0% 0% 19% 1% 3% 1% 0% 3% 1% 0% 0% 3% 14% 12% 4% 5% 0% 5% 5% 3% 1% 13% 0% 16% 0% 29% 5% 24% 3% 23% 4% 29% 10% Figures show the incidence of gastrointestinal adverse events (I) and rates of discontinuation (D) for this reason; a significantly different (p<0.05) for metformin versus placebo (all doses); b includes diarrhoea, dyspepsia, nausea and anorexia (abdominal pain was classified as a ‘whole body’ adverse event). glucose was more sensitive to the effects of metformin than FPG in this study (figure 7). It is likely, therefore, that reductions in postprandial glucose contribute to the improvements in HbA1C observed during treatment with higher metformin doses. Since postprandial glucose is an independent risk factor for the development of diabetic complications, including coronary heart disease, retinopathy or renal dysfunction,25-27 this might be one mechanism whereby metformin proved so effective in the UKPDS trial. Safety and tolerability Gastrointestinal adverse events The majority of adverse events associated with metformin therapy are gastrointestinal, and usually appear soon after the initiation of therapy. They can lead to discontinuation of therapy in up to 5% of patients.17 These effects are usually transient, and tend to subside over several months of continued therapy.28 The impact of gastrointestinal adverse events during initiation of metformin therapy may be minimised by titrating from an initial dose of 500 mg, and by taking metformin with or immediately after food. The biological mechanism underlying metformin-induced gastrointestinal side-effects has not been fully elucidated, but increased colonic concentrations of bile salts29 and increased intestinal 5-hydroxytryptamine (serotonin) release30 appear to be involved. The tolerability of different doses of metformin was analysed in detail in the parallel-group study in 451 patients,14 described above. Table 3 shows the incidence of gastrointestinal adverse events from this study, and the percentages of patients discontinuing therapy as a result. Above 500 mg/day, there is no clear evidence of a dose relationship for either the incidence of individual or pooled gastrointestinal side-effects, or for treatment discontinuations arising from an adverse drug event. In this study, the good tolerance to metformin was attributed to gradual dose escalation at weekly intervals, and VOLUME 1 ISSUE 1 . AUGUST 2001 administration with meals (table 3). This lack of association between metformin dosage and drug related side-effects confirms the findings of one of the earlier studies15 but is in contrast to the observations of another.13 A questionnaire-based study of 285 randomly selected type 2 outpatients11 provides further evidence for the lack of dose-response for gastrointestinal side-effects. Although 20% of responders receiving metformin complained of diarrhoea, there were no differences in incidence between patients receiving low and high doses. In the case of patients with intractable symptoms, transient reduction in the dose and subsequent gradual re-titration can lead to improved tolerance.31 The drug is best withdrawn in patients with persistent diarrhoea. Lactic acidosis A relatively high incidence of lactic acidosis led to the withdrawal of the biguanide phenformin in most countries, and an association between this adverse event and biguanides in general has often been made in reviews of oral antidiabetic therapy. The incidence of lactic acidosis with metformin is very rare and reported as between 3–9 cases per 100 000 patient-years of treatment with 2–4 deaths/100 000 patient-years and is up to 20 times lower than the incidence described in patients treated with phenformin.32-34 Several reports indicate increased lactate production during metformin treatment in type 2 diabetes patients, although this has not been observed in all studies.35-37 There is good evidence that neither plasma metformin nor lactate concentrations are of any help in predicting clinical outcomes, even in patients with very high lactate levels.37-39 Due to the co-morbidity associated with type 2 diabetes, it is anticipated that some cases of lactic acidosis in patients receiving metformin are unrelated to the therapy with this agent.40-41 A review of all published cases of lactic acidosis in patients receiving metformin has recently been published.38 Twenty-one 33 REVIEW reports over a five-year period, including information on 26 patients, are included in this review. Four cases did not fit criteria for true lactic acidosis (arterial lactate > 5 mmol/L, blood pH ≤ 7.35), lactic acidosis was not associated with metformin accumulation in another eight, and was of uncertain origin in a further two cases. Metformin accumulation was considered to have contributed to the development of lactic acidosis in 12 cases, of whom all had acute or chronic renal dysfunction. Importantly, the true aetiology of the lactic acidosis strongly influenced the eventual clinical outcomes of these patients. Of the eight cases of documented lactic acidosis that were not associated with metformin, seven patients died. In contrast, the only death among the 12 patients with lactic acidosis considered to be metformin-related occurred as a result of the patient’s refusal to undergo renal dialysis. Although a link is often drawn between metformin accumulation and lactic acidosis, the plasma concentration of metformin is of no prognostic benefit in patients with this condition. In a study of 49 metformin-treated patients with lactic acidosis, the median metformin plasma concentration in 27 patients who survived (20.6 mg/l) was considerably higher than the corresponding concentration in 22 patients who died (6.3 mg/l).39 Given that the maximal plasma concentration of metformin achieved after an 850 mg oral dose is in the range 1.5–2.0 mg/l,17 it follows that even metformin concentrations well above the normal therapeutic range were not associated with a poorer outcome in these patients. The development of lactic acidosis during metformin therapy therefore often results from the presence of intercurrent disease, rather than from the use of metformin itself. Furthermore, the incidence of genuine metformin-related lactic acidosis appears to be lower than that cited in the literature. Nevertheless, it remains important to minimise the risk of lactic acidosis with metformin by paying careful attention to the contraindications and special precautions associated with metformin use, especially with regard to renal or hepatic impairment and alcohol abuse. Conditions precluding the use of metformin are not uncommon in type 2 diabetic patients42 and evidence from surveys suggests that a substantial proportion of patients who have received metformin have absolute contraindications, intercurrent conditions or other risk factors incompatible with metformin therapy, although no cases of lactic acidosis were reported in these surveys.43,44 The risk of lactic acidosis with metformin is low if the prescribing instructions for metformin are followed correctly.34,37 Careful assessment of patients at the time of initiation of metformin therapy, and regular surveillance of patients to detect the development of contraindications to metformin form an essential part of successful long-term management of type 2 diabetes with metformin. Vigilance is required at the time of radiological investigations involving intravascular administration of iodinated contrast materials as these agents can precipitate renal failure. Metformin therapy should be discontinued at the time of the procedure, withheld for a minimum of 48 hours, and reinstated only after renal function is confirmed as normal.32 34 Clinical implications of optimising metformin therapy Risk versus benefit of higher doses of metformin Taken together, the four dose ranging studies described above indicate that the antihyperglycaemic efficacy of metformin is dose-related, and that this relationship extends to daily doses of metformin at the upper limits of the recommended daily dosage ( > 2000 mg/day ). On the other hand, the evidence suggests that increasing the metformin dose beyond 1500–2000 mg/day does not markedly increase the risk of gastrointestinal sideeffects or lactic acidosis, and fear of these side-effects should not prevent the achievement of optimal dosage levels in patients with type 2 diabetes. The additional efficacy available from higher metformin doses is potentially important in the prevention of long-term diabetic complications. Evidence from the UKPDS indicates that each 1% decrease in HbA1C is likely to yield clinically important reductions in the risk of diabetic complications, including diabetes related death (by 21%), myocardial infarction (by 14%), peripheral vascular disease (by 43%), microvascular disease (by 37%) and cataract extraction (by 19%).1 It is therefore most important that HbA1C is controlled adequately. Importantly, the intensive glycaemic management of patients receiving metformin achieved by UKPDS can be realised in routine clinical management of such patients, as demonstrated by a three-year community-based study which reduced baseline HbA1C by 1.5%.12 In addition to being an effective antihyperglycaemic agent, metformin improves other cardiovascular risk factors related to the insulin resistance syndrome, also referred to as ‘metabolic syndrome’ or ‘syndrome X’, in diabetic patients.9,17,32 For example, dose-related improvements in fibrinolytic parameters (plasminogen activator inhibitor-1 [PAI-1] activity, PAI-1 antigen, tissue plasminogen activator [tPA] activity and tPA antigen) were observed after six months of metformin therapy at doses of up to 3000 mg/day.13 Improved fibrinolysis is likely to reduce the risk of intravascular thrombotic events, such as myocardial infarction, and may contribute to the beneficial cardiovascular effects of metformin in type 2 diabetic patients.45,46 Metformin also improves lipid profiles in many patients, including beneficial effects on LDL, VLDL and HDL cholesterol, free fatty acids and triglycerides.32 Maintained quality of life during intensive metformin therapy The impact of intensive glycaemic management and of the presence or absence of diabetic complications on quality of life was measured in the UKPDS.47 Individual questionnaires were used to evaluate patients’ quality of life relating to satisfaction with work, mood, symptoms and cognitive function, while the generic EQ5D questionnaire was used to explore patients’ general well-being. There were no significant differences in the scores for any dimension of quality of life in patients receiving intensive therapy with metformin, compared with patients receiving conventional, diet-based therapy. In contrast, the presence of macrovas- THE BRITISH JOURNAL OF DIABETES AND VASCULAR DISEASE REVIEW cular complications significantly impaired general well-being, and the presence of microvascular complications significantly impaired quality of life relating to mood and symptoms. Therefore, the presence of complications impairs quality of life in patients with type 2 diabetes, while intensive glycaemic management with metformin does not. Compliance issues Polypharmacy, defined as the long-term use of two or more pharmacologic therapies, is common, especially in elderly patients with diabetes who are at increased risk of other diseases of ageing, such as hypertension, ischaemic heart disease or arthritis. Indeed, age and diabetes have been shown to be highly significant risk factors for receiving polypharmacy (p=0.0002 and p=0.0001, respectively) in a study of data from 1,544 patients over a three-year period.48 It is well accepted that polypharmacy is a clinically significant barrier to good compliance with therapeutic regimens, especially where patients take several doses of medication per day, and non-adherence to therapy is common among patients with diabetes.49,50 This has been demonstrated quantitatively in patients with type 2 diabetes, by the Diabetes Audit and Research in Tayside, Scotland (DARTS) Study, which recorded the medication details of 2,920 patients for 12 months.51 Data on prescriptions were used to define an Adherence Index, which provided an estimate of the proportion of the year for which patients had adequate therapeutic cover from their medication. Adequate adherence to therapy was defined as an Adherence Index of 90% or greater, after adjustment for hospitalisation. The median Adherence Indices in patients receiving either of two oral antidiabetic monotherapies were 300 and 302 days. When the agents were given together as a free combination, involving an increase in the number of tablets taken per day, the Adherence Index fell to 266 days (p<0.01 for the difference between monotherapy and combination therapy). It follows, therefore, that increasing the dose of oral antidiabetic therapy could hinder patient compliance with therapy if this involved the administration of a greater number of tablets per day. The benefits of simplifying the dosage regimen for metformin have been demonstrated in a crossover study involving some 64 patients.52 Patients stabilised and maintained on 1500–2000 mg per day of metformin were switched to 850 mg twice-daily, whilst those on 2500–3000 mg were converted to 850 mg three times daily. Three months after conversion, no significant changes were noted in glycaemic control, and some 90% of patients reported nothing untoward and were willing to continue medication with the high dosage strength. Simplifying the antidiabetic regimen to reduce the number of metformin tablets per day would therefore seem practical, straightforward and safe. The recently introduced 1000 mg tablet should, in principle, allow the delivery of higher doses of metformin without adding to the already arduous burden of polypharmacy in these patients. VOLUME 1 ISSUE 1 . AUGUST 2001 Key messages ● UKPDS has established metformin as a preferred first line agent for pharmacological treatment of type 2 diabetes ● Adequate titration of metformin is required, taking the drug with meals to reduce GI side effects ● Metformin offers benefits against cardiovascular disease in type 2 diabetes Conclusions The UKPDS showed that metformin improves clinical outcomes in type 2 diabetic patients by controlling glycaemia, and through additional as yet undefined cardiovascular protective effects. Metformin is therefore established as the first line component of oral antidiabetic therapy for patients without contraindications to this drug. We also know from the UKPDS that the degree of protection from complications is determined by the magnitude of the reduction in HbA1C. The efficacy of metformin in controlling glycaemia is related to dose, generally requiring titration up to 2000 mg/day or above to achieve optimal effect. Therapy should however be individualised, and with this objective the full therapeutic dose range of metformin should be exploited where appropriate in order to optimise the benefits of therapy. At all times vigilance should be maintained to ensure safety of use during intensification of metformin therapy. The recently introduced 1000 mg metformin tablet will facilitate the use of higher doses of metformin with the potential to improve compliance. References 1. Stratton IM, Adler AI, Neil HAW et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-12. 2. European Diabetes Policy Group. A desktop guide to type 2 diabetes mellitus. Diabet Med 1999;16:716-30. 3. American Diabetes Association. Clinical Practice Recommendations. Diabetes Care 1999;22(Suppl 1):S1-114. 4. New JP, Hollis S, Campbell F et al. Measuring clinical performance and outcomes from diabetes information systems: an observational study. Diabetologia 2000;43:836-43. 5. Krentz AJ, Ferner RE, Bailey CJ. Comparative tolerability profiles of oral antidiabetic agents. Drug Saf 1994;11:223-41. 6. Bailey CJ. Antidiabetic Drugs. Br J Cardiol 2000;7:350-60. 7. Schatz H. Preclinical and clinical studies on the safety and tolerability of repaglinide. Clin Exp Endocrinol Diabetes 1999;107(Suppl 4):S144-8. 8. Campbell IW, Howlett HC. Worldwide experience of metformin as an effective glucose-lowering agent: a meta-analysis. Diabetes Metab Rev 1995;11(Suppl 1):S57-62. 9. Johansen K. Efficacy of metformin in the treatment of NIDDM. Metaanalysis. Diabetes Care 1999;22:33-7. 10. UK Prospective Diabetes Study Group. Effect of intensive blood glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352:854-65. 11. Dandona P, Fonseca V, Mier A, Beckett AG. Diarrhea and metformin in a diabetic clinic. Diabetes Care 1983;6:472-4. 35 REVIEW 12. Stades AM, Heikens JT, Holleman F, Hoekstra JB. Effect of metformin on glycaemic control in type 2 diabetes in daily practice: a retrospective study. Neth J Med 2000;56:86-90. 13. Grant PJ. The effects of high- and medium-dose metformin therapy on cardiovascular risk factors in patients with type II diabetes. Diabetes Care 1996;19:64-6. 14. Garber AJ, Duncan TG, Goodman AM, Mills DJ, Rohlf JL. Efficacy of metformin in type II diabetes: results of a double-blind, placebo-controlled, dose-response trial. Am J Med 1997;103:491-7. 15. Hermann LS, Schersten B, Melander A. Antihyperglycaemic efficacy, response prediction and dose-response relations of treatment with metformin and sulphonylurea, alone and in primary combination. Diabet Med 1994;11:953-60. 16. McIntyre HD, Ma A, Bird DM, Paterson CA, Ravenscroft PJ, Cameron DP. Metformin increases insulin sensitivity and basal glucose clearance in type 2 (non-insulin dependent) diabetes mellitus. Aust NZ J Med 1991; 21:714-9. 17. Cusi K, DeFronzo RA. Metformin: a review of its metabolic effects. Diabetes Reviews 1998;6:89-131. 18. Davidson MB, Peters AL. An overview of metformin in the treatment of type 2 diabetes mellitus. Am J Med 1997;102:99-110. 19. Garber AJ. Using dose-response characteristics of therapeutic agents for treatment decisions in type 2 diabetes. Diabetes, Obesity and Metabolism 2000;2:139-47. 20. Campbell IW. Need for intensive, early glycaemic control in patients with type 2 diabetes. Br J Cardiol 2000;7:625-31. 21. Leatherdale BA, Bailey CJ. Acute antihyperglycaemic effect of metformin without alteration of gastric emptying. IRCS Med Sci 1986;14:1086-6. 22. Sambol NC, Chiang J, O’Conner M et al. Pharmacokinetics and pharmacodynamics of metformin in healthy subjects and patients with noninsulin-dependent diabetes mellitus. J Clin Pharmacol 1996;36:1012-21. 23. Hollenbeck CB, Johnston P, Varasteh BB, Chen Y-DI, Reaven GM. Effects of metformin on glucose, insulin and lipid metabolism in patients with mild hypertriglyceridaemia and non-insulin dependent diabetes mellitus by glucose tolerance test criteria. Diabete & Metabolisme (Paris) 1991;17:483-9. 24. Jeppesen J, Chen Y-DI, Zhou M-Y, Reaven GM. Effect of metformin on postprandial lipemia in patients with fairly to poorly controlled NIDDM. Diabetes Care 1994;17:1093-9. 25. Turner RC, Millns H, Neil HAW et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom prospective diabetes study (UKPDS 23). BMJ 1998;316:823-8. 26. Klein R, Klein BE, Moss SE, Cruickshanks KJ. Relationship of hyperglycemia to the long-term incidence and progression of diabetic retinopathy. Arch Intern Med 1994;154:2169-78. 27. Klein R, Klein BE, Moss SE, Cruickshanks KJ. Ten-year incidence of gross proteinuria in people with diabetes. Diabetes 1995;44:916-23. 28. Haupt E, Knick B, Koschinsky T, Liebermeister H, Schneider J, Hirche H. Oral antidiabetic combination therapy with sulphonylureas and metformin. Diabete Metab 1991;17:224-31. 29. Scarpello JH, Hodgson E, Howlett HC. Effect of metformin on bile salt circulation and intestinal motility in type 2 diabetes mellitus. Diabet Med 1998;15:651-6. 30. Cubeddu LX, Bonisch H, Gothert M et al. Effects of metformin on intestinal 5-hydroxytryptamine (5-HT) release and on 5-HT3 receptors. Naunyn 36 Schmiedebergs Arch Pharmacol 2000;361:85-91. 31. Bailey CJ. Biguanides and NIDDM. Diabetes Care 1992;15:755-72. 32. Howlett HC, Bailey CJ. A risk-benefit assessment of metformin in type 2 diabetes mellitus. Drug Saf 1999;20:489-503. 33. Stang M, Wysowski DK, Butler-Jones D. Incidence of lactic acidosis in metformin users. Diabetes Care 1999;22:925-7. 34. Chan NN, Brain HPS, Feher MD. Metformin-associated lactic acidosis: a rare or very rare clinical entity. Diabet Med 1999;16:273-81. 35. Cusi K, Consoli A, DeFronzo RA. Metabolic effects of metformin on glucose and lactate metabolism in non insulin-dependent diabetes mellitus. J Clin Endocrinol Metab 1996;81:4059-67. 36. Fery F, Plat L, Balasse EO. Effects of metformin on the pathways of glucose utilization after oral glucose in non-insulin-dependent diabetes mellitus patients. Metabolism 1997;46:227-33. 37. Lalau JD, Race JM. Lactic acidosis in metformin therapy: searching for a link with metformin in reports of ‘metformin-associated lactic acidosis’. Diabetes, Obesity and Metabolism 2000;2:1-7. 38. Lalau JD, Race JM. Lactic acidosis in metformin therapy. Drugs 1999;58(Suppl 1):55-60. 39. Lalau JD, Race JM. Lactic acidosis in metformin-treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations. Drug Saf 1999;20:377-84. 40. Bailey CJ, Turner RC. Drug therapy: Metformin. N Engl J Med 1996;334: 574-9. 41. Brown JB, Pedula K, Barzilay J et al. Lactic acidosis rates in type 2 diabetes. Diabetes Care 1998;21:1659-63. 42. Sulkin TV, Bosman D, Krentz AJ. Contraindications to metformin therapy in patients with NIDDM. Diabetes Care 1997;20:925-8. 43. Emslie-Smith AM, Boyle DIR, Evans JMM et al. Contraindications to metformin therapy in patients with Type 2 diabetes - a population-based study of adherence to prescribing guidelines. Diabet Med 2001;18:483-8. 44. Holstein A, Nahrwold D, Hinze S, Egberts E-H. Contra-indications to metformin are largely disregarded. Diabet Med 1999;16:692-6. 45. Grant PJ, Stickland MH, Booth NA, Prentice CR. Metformin causes a reduction in basal and post-venous occlusion plasminogen activator inhibitor-1 in type 2 diabetic patients. Diabet Med 1991;8:361-5. 46. Landin-Wilhelmsen K. Metformin and blood pressure. J Clin Pharm Ther 1992;17:75-9. 47. UK Prospective Diabetes Study Group. Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). Diabetes Care 1999;22:1125-36. 48. Veehof L, Stewart R, Haaijer-Ruskamp F, Jong BM. The development of polypharmacy. A longitudinal study. Fam Pract 2000;17:261-7. 49. Paes AHP, Bakker A, Soe-Agnie S-J. Impact of dosage frequency on patient compliance. Diabetes Care 1997;20:1512-17. 50. Brown JB, Nichols GA, Glauber HS, Bakst A. Ten-year follow-up of antidiabetic drug use, nonadherence, and mortality in a defined population with type 2 diabetes mellitus. Clin Ther 1999;21:1045-57. 51. Morris AD, Brennan GM, Macdonald TM, Donnan PT. Population-Based Adherence to Prescribed Medication in Type 2 Diabetes: A Cause for Concern. Diabetes 2000;49(Suppl 1):A76. 52. Menzies DG, Campbell I, McBain A, Brown IRF. Metformin efficacy and tolerance in obese non-insulin dependent diabetics: a comparison of two dosage schedules. Curr Med Res Opin 1989;11:273-8. THE BRITISH JOURNAL OF DIABETES AND VASCULAR DISEASE