Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
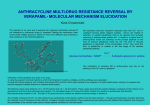
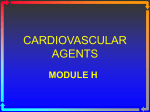
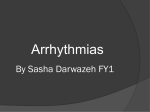
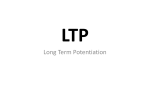
Journal of the American College of Cardiology © 2006 by the American College of Cardiology Foundation Published by Elsevier Inc. Vol. 48, No. 6, 2006 ISSN 0735-1097/06/$32.00 doi:10.1016/j.jacc.2006.04.092 Attenuation of the Negative Inotropic Effects of Metoprolol at Short Cycle Lengths in Humans Comparison With Sotalol and Verapamil Rebecca H. Ritchie, BSC(HONS), PHD,*† Christopher J. Zeitz, MBBS, PHD, FRACP,* Ronald D. Wuttke, BSC,* John T. Y. Hii, BMBS, FRACP,* John D. Horowitz, MBBS, PHD, FRACP* Adelaide and Melbourne, Australia This study sought to compare the influence of changes in systolic interval on the negative inotropic effects of metoprolol, sotalol, and verapamil in patients with ischemic heart disease. BACKGROUND The long-term symptomatic and prognostic effects of antiarrhythmic agents are not easily predicted on the basis of acute hemodynamic actions at rest, but may be unmasked during tachycardia. However, this has not been studied extensively in vivo. METHODS The force-interval relationship of the intact human left ventricle was examined before and 10 min after intravenous bolus administration of the negatively inotropic agents metoprolol, sotalol, or verapamil in patients undergoing diagnostic cardiac catheterization. RESULTS All three drugs similarly reduced maximal rate of increase of left ventricular pressures (LV⫹dP/dtmax) by approximately 10%, but diversely modified the force-interval relationship. The parameter c (the reduction in LV⫹dP/dtmax of a fixed premature stimulus on mechanical restitution) was significantly reduced by metoprolol (by 9 ⫾ 4%, p ⬍ 0.05), was increased by verapamil (by 6 ⫾ 2%, p ⬍ 0.05), and was not significantly changed by sotalol. Similarly, metoprolol had a minimal effect on the extent of frequency potentiation, whereas sotalol and verapamil attenuated frequency potentiation (the relative response to 10 s of rapid pacing was 1.19 ⫾ 0.58-fold, 0.07 ⫾ 0.35-fold, and 0.03 ⫾ 0.17-fold of the baseline response after 10 min of metoprolol, sotalol, or verapamil, respectively). CONCLUSIONS These results show that the negative inotropic effects of metoprolol are attenuated and those of verapamil are accentuated at short cycle lengths; sotalol is intermediate between the two. These properties may contribute to the relative safety of these agents in patients prone to hemodynamic deterioration during sustained tachycardia. (J Am Coll Cardiol 2006;48: 1234 – 41) © 2006 by the American College of Cardiology Foundation OBJECTIVES Onset of tachycardia in patients administered class I (sodiumchannel blocker) or class IV (calcium-channel antagonist) antiarrhythmic drugs is associated with increased risk of acute hemodynamic collapse, despite these agents being well tolerated in sinus rhythm (1,2). Changes in heart rate may thus unmask negative inotropic effects of cardioactive drugs not apparent at rest, which may contribute to increased mortality during treatment with such agents in patients with impaired left ventricular systolic function (3,4). Conversely, class II antiarrhythmic agents, beta-adrenoceptor antagonists, are not poorly tolerated at faster heart rates (5), suggesting differential modulation of the force-frequency relationship by antiarrhythmic agents. The relationship between alterations in stimulation rate and myocardial contractile performance can be studied using either frequency potentiation and/or mechanical restitution. Frequency potentiation, also known as the staircase or Treppe phenomenon, is commonly used in vitro (6,7), From the *Cardiology Unit, The Queen Elizabeth Hospital, University of Adelaide, Adelaide, Australia; and the †Baker Heart Research Institute, Melbourne, Australia. Supported by grants from the National Heart Foundation (Deakin, ACT, Australia) and the Merck Foundation (South Granville, NSW, Australia). Dr. Ritchie was a University of Adelaide (Adelaide, SA, Australia) and Queen Elizabeth Hospital Research Foundation (Woodville, SA, Australia) Postgraduate Scholar. Dr. Zeitz was a National Heart Foundation Postgraduate Scholar. Manuscript received July 8, 2005; revised manuscript received February 23, 2006, accepted April 4, 2006. and is illustrated by the incremental reductions in calciumchannel current and contractile force induced by verapamil in vitro with progressive increases in stimulation frequency (8,9). However, the sustained tachycardia of frequency potentiation in vivo may result in neurohumoral activation, changed loading conditions, ischemia, or even hemodynamic deterioration (10 –13). Such effects could distort the force-interval relationship, and thus limit utility of frequency potentiation. The force-interval relationship can also be examined (both in vitro and in vivo) using mechanical restitution curves (MRC). Mechanical restitution is the recovery of myocardial contractility after a non–steady-state beat (7). We have recently described a mathematical model of the MRC that has proven highly reproducible in patients under investigation for ischemic heart disease (14,15). In the current investigation, we studied the acute effects of 3 pharmacologically different antiarrhythmic agents on the forceinterval relationship, metoprolol (a selective 1-adrenoceptor antagonist), d,l-sotalol (a nonselective -adrenoceptor antagonist with additional outward delayed rectifier potassium current blocking properties) and verapamil (an L-type calcium-channel antagonist). All three drugs elicit negative inotropic effects in sinus rhythm. Using both MRC construction and frequency potentiation analysis, we tested the hypothesis that the negative inotropic effects of metoprolol, JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 Abbreviations and Acronyms CI ⫽ confidence interval ECG ⫽ electrocardiographic LV⫹dP/dtmax ⫽ maximal rate of increase of left ventricular pressures MAP ⫽ mean arterial pressure MRC ⫽ mechanical restitution curve but not those of verapamil, were independent of changes in R-R interval in patients with ischemic heart disease. Although previous data have suggested that the negative inotropic effects of verapamil might be accentuated at higher stimulation frequencies (9,10), clinically based hemodynamic comparisons of these agents have been lacking. METHODS Study population. Patients with stable symptoms were selected from those undergoing routine diagnostic cardiac catheterization and coronary arteriography for the investigation of chest pain. Exclusion criteria included unstable angina pectoris, significant left main coronary artery stenosis, electrocardiographic (ECG) evidence of abnormal conduction intervals, clinically significant valvular disease, recent myocardial infarction (in the last 3 months), and severe impairment of left ventricular systolic function (ejection fraction ⬍30%), in addition to clinically significant renal or hepatic disease. The protocol was approved by the Ethics of Human Research Committee of The Queen Elizabeth Hospital, and prior informed consent was obtained. Catheterization protocol. Administration of all betaadrenoceptor and calcium-channel antagonists was ceased at least 5 half-lives before the study. Oral diazepam and diphenhydramine were administered approximately 30 min before cardiac catheterization as premedication. Right and left cardiac catheterization and coronary arteriography were performed under local anesthesia (1% lidocaine) using the Judkins approach via femoral arterial (16) and venous sheaths. The research procedure commenced at the end of the routine catheterization. A bipolar pacing lead was positioned in the right atrium, and a 4-F micromanometer-tipped catheter (Millar Instruments, Houston, Texas) was inserted via the femoral artery sheath into the left ventricle for measurement of left ventricular pressure and maximal rate of increase of left ventricular pressures (LV⫹dP/dtmax). A 7-F Swan-Ganz catheter was positioned in the pulmonary artery for determination of cardiac output via thermodilution. Incremental radiation exposure associated with the research procedure was minimal, limited to screening to check Millar catheter position. Patients underwent continuous baseline atrial pacing at a rate 7 ⫾ 1% above spontaneous heart rate to maintain a constant heart rate throughout the procedure. Cardiac output (the average of at least three readings at each time point), mean arterial pressure (MAP), ECG parameters, and left ventricular Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship 1235 pressure and its first derivative LV⫹dP/dtmax were recorded continuously. After acquisition of baseline data, including MRC and frequency potentiation determination, patients were sequentially allocated to receive metoprolol (4 mg; n ⫽ 15), sotalol (20 mg; n ⫽ 15), or verapamil (4 mg; n ⫽ 17) as a rapid intravenous bolus. Sodium nitroprusside was also investigated in an additional subgroup of patients (10 to 20 g/min intravenous infusion until approximately a 10% reduction in MAP was observed, n ⫽ 5) to determine the influence, in isolation, of altered loading conditions on the MRC. The dose of each agent was chosen from the lower end of the dosage range used clinically. Hemodynamic measurements and serial MRCs were obtained at frequent intervals up to 10 min after administration. Frequency potentiation was re-examined at 10 min. Mechanical restitution. The MRCs were constructed as previously described (14,15). Briefly, premature stimuli of twice the threshold strength were inserted every 8 beats during baseline pacing, at progressively shorter R-R intervals, until refractoriness prevented impulse conduction. The contractile strength of each beat, LV⫹dP/dtmax, was plotted as a function of the R-R interval. The LV⫹dP/dtmax was expressed as a percent of that observed in the drug-free state during baseline pacing, and R-R interval as a percent of the cycle length of the baseline-pacing rate. This was then fitted to one-half of a rectangular hyperbolic function, described by: y ⫽ a ⫺ 关c (100 ⫺ d) (60 ⫺ d)兴 ⁄ 关40 (x ⫺ d)兴 where x is the R-R interval of the premature stimulus and y is LV⫹dP/dtmax. The horizontal and vertical asymptotes are represented by a and d, respectively. The parameter c, the difference between the calculated values of LV⫹dP/dtmax from the fitted curve when the R-R interval is 100%, and Figure 1. A theoretical mechanical restitution curve (MRC): a (units are percent baseline LV⫹dP/dtmax) and d (units are percent baseline R-R interval) represent the horizontal and vertical asymptotes, respectively; the parameter c (units are percent baseline LV⫹dP/dtmax) represents the reduction in LV⫹dP/dtmax with a 40% reduction in R-R interval (13). LV⫹dP/dtmax ⫽ maximal rate of increase of left ventricular pressures. 1236 Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship 60% (illustrated in Fig. 1), describes contractile sensitivity to reductions in R-R interval for each patient (14). We then calculated the change in the parameter c 10 min after treatment by subtracting it from the pretreatment value, to obtain ⌬-parameter c. Thus, an increase in c after drug administration (i.e., positive ⌬-parameter c) would indicate directly rate-dependent negative inotropic effects. Frequency potentiation. The force-interval relationship was also assessed using frequency potentiation by determining the influence of 1 min of rapid pacing (34 ⫾ 2% above the rate of baseline pacing) on LV⫹dP/dtmax in 10-s intervals. This protocol was not performed in patients with severe angina pectoris, and was precluded by the development of atrioventricular block in some patients. We then further analyzed the frequency potentiation response by expressing the pacing-induced increase in LV⫹dP/dtmax after drug administration in each patient as a ratio of the response observed before treatment for each of metoprolol, sotalol, and verapamil to calculate the relative frequency potentiation response. Statistical analyses. Results were expressed as mean ⫾ SE. The goodness-of-fit of the MRC model for each individual patient was determined using residual standard deviations. Confidence intervals (Cis) at 95% were derived for these standard deviations. One-factor analysis of variance was used to compare patient characteristics at baseline in the four groups, and with repeated measures analysis (Dunnett), to examine the time course of LV⫹dP/dtmax and c as appropriate. Paired t tests were used to compare the hemodynamic and ECG effects of the drugs studied, before and 10 min after injection. The differential effects of the three agents, metoprolol, verapamil, and sotalol, on MRC analysis were examined via one-way analysis of variance of ⌬-parameter c across all three patient groups. To determine whether the 3 agents attenuated the frequency potentiation response, we compared the relative frequency potentiation response across all three patient groups using a 1-way analysis of variance. Statistical significance was accepted at the p ⬍ 0.05 level. RESULTS Patient characteristics. The clinical characteristics before drug injection of all 52 patients studied are summarized in Table 1. The groups were generally well matched, with predominantly normal left ventricular systolic function, and JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 Figure 2. Time course of changes in LV⫹dP/dtmax (percent baseline) induced by metoprolol, sotalol, or verapamil during baseline pacing before (open bars), 5 min after (hatched bars), and 10 min after (solid bars) injection. Asterisks indicate statistical significance compared with baseline (analysis of variance with repeated measures). Abbreviations as in Figure 1. no significant differences in characteristics between the groups. Clinically significant coronary artery disease (stenosis ⱖ50% in at least 1 major branch of a coronary artery) was present in 36 patients. The procedure was well tolerated in all patients. Hemodynamic effects during baseline pacing. The doses for each of metoprolol, sotalol, and verapamil used in the present study were chosen with the intention of achieving similar negative inotropic effects at baseline pacing: the three negatively inotropic drugs induced approximately a 10% reduction in LV⫹dP/dtmax (Fig. 2). Table 2 summarizes the hemodynamic and ECG effects of all drugs studied during baseline pacing, at the time of peak effect (10 min after drug injection for metoprolol, sotalol, and verapamil, and at the time of maximal hypotensive effect for sodium nitroprusside). The MAP was significantly reduced by both verapamil and sodium nitroprusside (as a requirement of the length of the infusion period), but not by either metoprolol or sotalol. Sodium nitroprusside had no additional hemodynamic effects, although pulmonary capillary wedge pressure also tended to decrease (from 13 ⫾ 2 mm Hg to 10 ⫾ 1 mm Hg, p ⫽ NS). Force-interval relationship. The influence of metoprolol, sotalol, and verapamil on the MRC is shown in Figure 3 before and 10 min after injection (the time of peak effect). The residual SDs of the model (the measure of goodnessof-fit) for these drugs were 4.9 (95% CI 3.3 to 6.4), 5.1 (95% CI 3.5 to 6.7), and 8.3 (95% CI 5.9 to 10.6; p ⬍ 0.05 vs. metoprolol and verapamil) for metoprolol, verapamil, Table 1. Patient Characteristics at Baseline Metoprolol Sotalol Verapamil Sodium Nitroprusside (n ⴝ 15) (n ⴝ 15) (n ⴝ 17) (n ⴝ 5) Age (yrs) Gender (male/female) Coronary disease* Left ventricular ejection fraction (%) Pulmonary capillary wedge pressure (mm Hg) Paced relative risk interval (ms) 56 ⫾ 2 11/4 10 (67%) 63 ⫾ 3 8⫾1 800 ⫾ 40 54 ⫾ 2 10/5 11 (73%) 72 ⫾ 2 7⫾1 780 ⫾ 30 61 ⫾ 3 9/8 12 (71%) 69 ⫾ 3 8⫾1 730 ⫾ 30 61 ⫾ 6 1/4 3 (60%) 65 ⫾ 3 13 ⫾ 1 710 ⫾ 40 *Greater than 50% stenosis in at least 1 coronary artery (left anterior descending, circumflex, or right coronary artery). Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 1237 Table 2. Hemodynamic and Electrocardiographic Effects During Baseline Atrial Pacing of Each Drug Studied, at Time of Peak Effect (10 Min After Injection for Metoprolol, Sotalol, and Verapamil; Approximately 5 Min After Infusion Stopped for Sodium Nitroprusside) Metoprolol 2 Cardiac index (l/min/m ) Mean arterial pressure (mm Hg) PR interval (ms) QT interval (ms) LV⫹dP/dtmax (% baseline) Sotalol Verapamil Sodium Nitroprusside Before After Before After Before After Before After 2.6 ⫾ 0.1 101 ⫾ 4 182 ⫾ 6 367 ⫾ 11 100 ⫾ 0 2.6 ⫾ 0.1 103 ⫾ 3 190 ⫾ 6* 365 ⫾ 10 88 ⫾ 3* 2.7 ⫾ 0.1 109 ⫾ 3 193 ⫾ 9 379 ⫾ 8 100 ⫾ 0 2.5 ⫾ 0.1 110 ⫾ 3 201 ⫾ 8* 386 ⫾ 7 89 ⫾ 3* 3.1 ⫾ 0.1 109 ⫾ 4 210 ⫾ 8 356 ⫾ 8 100 ⫾ 0 3.1 ⫾ 0.1 104 ⫾ 4* 215 ⫾ 9 360 ⫾ 6 93 ⫾ 2* 2.9 ⫾ 0.1 117 ⫾ 11 186 ⫾ 19 370 ⫾ 7 100 ⫾ 0 2.7 ⫾ 0.1 105 ⫾ 9* 182 ⫾ 18 370 ⫾ 9 95 ⫾ 4 *p ⬍ 0.05 vs. before drug. LV⫹dP/dtmax ⫽ maximal rate of increase of left ventriclar pressures. and sotalol, respectively. Although all three drugs exerted a similar negative inotropic effect during baseline pacing (Fig. 2), these effects differed on MRC analysis. Metoprolol decreased LV⫹dP/dtmax by 12 ⫾ 3% during baseline pacing. However, this negative inotropic effect became less marked at shorter R-R intervals, and was completely abolished when the R-R interval was reduced to 60%. On the fitted MRC, LV⫹dP/dtmax was 72 ⫾ 4% and 70 ⫾ 3% at an R-R interval of 60% before and after metoprolol, respectively (Fig. 3A). This was reflected by a significant reduction in c from 28 ⫾ 4% to 21 ⫾ 3% (Fig. 4A; p ⬍ 0.05). In the group of patients allocated to receive sotalol, LV⫹dP/dtmax was reduced by 11 ⫾ 3% during baseline pacing. On MRC analysis, the negative inotropic effect of sotalol was virtually unchanged as the R-R interval decreased. The LV⫹dP/ dtmax on the fitted MRC was 72 ⫾ 6% and 59 ⫾ 7% at an R-R interval of 60% before and after sotalol, respectively (Fig. 3B), and c did not fluctuate significantly (from 29 ⫾ 6% to 31 ⫾ 7%, p ⫽ NS) (Fig. 4B). In contrast with metoprolol and sotalol, verapamil tended to induce a divergence of the MRC, with the negative inotropic effect (8 ⫾ 2% reduction in LV⫹dP/dtmax at baseline) progressively accentuated as the R-R interval decreased. On the fitted MRC, LV⫹dP/dtmax was 81 ⫾ 4% and 67 ⫾ 5% at an R-R interval of 60% before and after verapamil, respectively (Fig. 3C). This corresponded to an increase in c from 18 ⫾ 4% at baseline to 24 ⫾ 4%, indicative of a rate-dependent effect (p ⬍ 0.05) (Fig. 4C). Moreover, when ⌬-parameter c after 10 Figure 3. Mechanical restitution curve (MRC) curve-fitting analysis for (A) metoprolol, (B) sotalol, and (C) verapamil. The left-hand panel shows representative raw and fitted data obtained from one patient in each group, before (closed circles, solid curve) and 10 min after (open circles, dashed curve) drug administration. The right-hand panel shows mean data from the fitted MRC before (closed circles) and after (open circles) drug administration. Abbreviations as in Figure 1. 1238 Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 Figure 4. Time course of changes in the parameter c from mechanical restitution curve (MRC) curve-fitting analysis (the decrease in LV⫹dP/dtmax with a 40% reduction in R-R interval from the fitted MRC model) for each of (A) metoprolol, (B) sotalol, and (C) verapamil. Asterisks indicate statistical significance compared with baseline (analysis of variance with repeated measures). (D) The increment in parameter c after drug treatment. Verapamil induces a significantly different response to metoprolol (analysis of variance). Abbreviations as in Figure 1. min was compared among metoprolol, sotalol, and verapamil, the MRC response to metoprolol was significantly different than that obtained with verapamil (p ⬍ 0.05) (Fig. 4B). The significant decrease in MAP induced by sodium nitroprusside, however, was not accompanied by significant alterations in LV⫹dP/dtmax either during baseline pacing (⫺5 ⫾ 4% vs. baseline, p ⫽ NS) or at shorter R-R intervals. No significant fluctuations in the parameter c were observed (from 43 ⫾ 6% to 43 ⫾ 7%, p ⫽ NS, results not shown). Frequency potentiation. The force-interval relationship was also investigated using frequency potentiation analysis before and 10 min after administration of each of the three negatively inotropic drugs. Figure 5 shows the time course of LV⫹dP/dtmax during rapid pacing. Before drug administration, the effects of rapid pacing were comparable in the 3 treatment groups, showing an initial increase of approximately 20% in LV⫹dP/dtmax, which was preserved for the full minute. As with MRC analysis, all three agents examined showed different effects on the extent of frequency potentiation (Fig. 5), especially evident after 10 s of rapid pacing. Metoprolol did not affect the frequency potentiation response: the pacing-induced increases in LV⫹dP/dtmax before and after the drug were maintained (Fig. 5A). This was not the case for verapamil: the pacing-induced increase in LV⫹dP/dtmax seemed to be markedly suppressed during the 1 min of rapid pacing (Fig. 5C). The results for sotalol were intermediate between those of metoprolol and verapamil (Fig. 5C). As shown in Figure 5D, the relative frequency potentiation response after metoprolol was un- changed after 10 s of rapid pacing; conversely, both sotalol and verapamil significantly attenuated the relative frequency potentiation response (p ⬍ 0.005). After 60 s of rapid pacing (at which time ischemia and/or neurohumoral activation may be evident [10,12]), sotalol, however, no longer the attenuated the frequency potentiation response (results not shown). DISCUSSION The results of the current study show that the negative inotropic effects during tachycardia of a pharmacologically heterogeneous group of antiarrhythmic drugs cannot be predicted on the basis of their observed effects in the resting state. Metoprolol, sotalol and verapamil were administered acutely at doses that elicited comparable negative inotropic effects at rest (Fig. 2) and minimal changes in pulmonary capillary wedge pressure. However, these three agents exerted markedly different negative inotropic effects at shorter R-R intervals, as determined from both MRC (Figs. 3 and 4) and frequency potentiation analysis (Fig. 5). The negative inotropic effects of metoprolol were markedly attenuated at short cycle lengths on MRC analysis, and metoprolol did not attenuate the inotropic response associated with frequency potentiation. Conversely, verapamil exerted directly rate-dependent negative inotropic effects, virtually ablating the frequency potentiation response; accentuation of verapamil’s negative inotropy was also evident at short R-R intervals on MRC analysis. The effects of sotalol were JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship 1239 Figure 5. Influence of negatively inotropic agents on frequency potentiation for each of (A) metoprolol, (B) sotalol, and (C) verapamil. Time course of LV⫹dP/dtmax during rapid pacing before (closed circles) and after (open circles) drug injection. Results are expressed as a percent of LV⫹dP/dtmax observed immediately before the onset of rapid pacing. (D) The relative frequency potentiation (FP) response after drug treatment (the increase in LV⫹dP/dtmax after 10-s rapid pacing, observed 10 min after treatment as a ratio of the response observed previously). Both sotalol and verapamil (but not metoprolol) significantly attenuated the frequency potentiation response (analysis of variance). Abbreviations as in Figure 1. intermediate between those of metoprolol and verapamil, relatively independent of R-R interval on MRC analysis and some attenuation of the frequency potentiation response. Construction of MRCs was the primary methodology used in the current study for the quantitative examination of drug effects on the force-interval relationship. We have previously shown that this is highly reproducible, with significant determinants of the parameter c including R-R interval (held constant in the present investigation) and left ventricular ejection fraction (14,15). Sodium nitroprusside, used in part because of the known insensitivity of the force-frequency relationship to nitric oxide (17), exerted no significant effects on mechanical restitution, suggesting that the parameter c is relatively independent of small changes in preload and afterload. Nevertheless, it remains possible that differential effects on preload might have influenced some of the observed differences between verapamil and metoprolol/ sotalol. The use of additional measures of the inotropic state, and in particular the simultaneous measurement of left ventricular pressure and volume, would have provided more load-independent assessment of drug effect. The reductions in LV⫹dP/dtmax induced by metoprolol and sotalol in the present study are consistent with previous investigations in humans (18 –21). However, we now show that the negative inotropic effect of metoprolol is reverse rate-dependent on MRC analysis. These data are consistent with recent suggestions that metoprolol normalizes the ventricular forcefrequency relationship in patients with heart failure (5). Conversely, sotalol did not significantly influence MRC. Also on MRC analysis, we quantitatively showed that the negative inotropic effect of verapamil was accentuated at shorter R-R intervals in humans in vivo. The ratedependent nature of this negative inotropic effect has been clearly defined in animal models in vitro (8,9). However, no evidence of this type for verapamil or any other calcium antagonist in humans was previously available. Clinical experience with the acute administration of verapamil has suggested the potential for acute hypotensive and negative inotropic sequelae (2,4), a complication that is rarely observed in the absence of tachyarrhythmias. The most appropriate examination of the effects of all three agents on frequency potentiation is after 10 s of rapid pacing (Fig. 5D) because more prolonged tachycardia may induce ischemia (12) and/or neurohumoral activation (10) in some patients. Nevertheless, the three agents examined disparate effects on frequency potentiation irrespective of the period of rapid pacing considered. Metoprolol had no detectable effect, whereas verapamil significantly (and sotalol to a lesser extent) impaired the frequency potentiation response. These disparate effects of the agents examined may reflect the underlying physiological changes involved in mechanical restitution and frequency potentiation. Frequency potentiation in an intact circulation represents a complex model comprising both negative (mechanical restitution-like) and positive inotropic (Treppe-like) components. The cellular correlates of this model cannot be ascertained in the current setting. Nevertheless, the rank order of rate-related negative inotropic effects (verapamil ⬎ 1240 Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship sotalol ⬎ metoprolol) was identical to that seen with MRC analysis. The incomplete MRC, the principal measure of the force-interval relationship used in the present study, reflects availability of calcium for contractile performance. Conventionally it has been regarded that a major determinant of mechanical restitution at low stimulation frequencies is calcium release from the sarcoplasmic reticulum, whereas trans-sarcolemmal calcium flux becomes increasingly important at high stimulation frequencies (8,9,22,23). The diverse effects of metoprolol and verapamil at shorter R-R intervals observed in the current study may simply reflect different sites of action on frequency-dependent cellular physiology. The interaction between verapamil and the L-type calcium channel per se is frequency-dependent: the drug binds preferentially to its receptor when the channel is in the open state (8). No analogous cellular phenomenon has been observed for beta-adrenoceptor ligands. The major finding of attenuation of the negative inotropic effect of metoprolol at short cycle lengths is of great interest. Superficially, this is a somewhat paradoxical observation because previous studies in a range of myocardial preparations (24) have suggested that the positive inotropic response to beta-adrenoceptor agonists increases with stimulation frequency. Available data for betaadrenoceptor antagonists, however, are consistent with our observations: both chronic therapy of heart failure patients with metoprolol and acute propranolol treatment in intact canine ventricles are associated with attenuated negative inotropic effects at increased heart rates (5,25). The effects of sotalol on MRC and frequency potentiation clearly differed from those of metoprolol in the present study. The only previously reported investigation of sotalol effects in human ventricular myocardium (26) failed to show any effect of either d,l-sotalol or of d-sotalol (which lacks effects at the beta-adrenoceptor while retaining potassiumchannel blockade), but the potential for rate-related inotropic interactions was not examined. The results of the current study imply that the potassium-channel blocking actions of sotalol modulate its inotropic effects, resulting in incremental negative inotropy during tachycardia. Study limitations. This was essentially a study of patients with intact left ventricular systolic function (by nature of the selection criteria). It is possible that studying patients with impaired systolic function would produce different results with respect to the relationship between MRC and frequency potentiation data: such patients might show an underlying defect of intracellular calcium availability (27,28), the consequences of which would increase progressively as heart rate increased (29). Furthermore, we did not investigate the mechanisms underlying the attenuation of frequency potentiation effects (attributed to progressive induction of ischemia and counter-regulatory neurohumoral activation). The use of a pacing regimen that was sufficiently brief as to be associated with no overt ischemia in any patient clearly does not preclude the possibility that some patients might have developed subclinical ischemia during the JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 latter stages of the frequency potentiation protocol. On the other hand, it is unlikely that the abolition of bradycardiarelated anti-ischemic effects (in the cases especially of metoprolol and sotalol) would have differentially influenced the current results. Lastly, the potential for a correlation between changes in the force-interval relationship and simultaneous evaluation of cellular electrophysiology, difficult to accurately obtain in vivo, was not sought. Nevertheless, such information might have provided additional insight, particularly in the case of sotalol. Conclusions. In summary, we have shown that the negative inotropic effects of metoprolol are attenuated at short cycle lengths. This would in theory be a salutary effect as regards maintenance of hemodynamic status during tachycardia, especially in the presence of impaired ventricular function, but might limit the effectiveness of the drug as an antianginal agent. Conversely, verapamil shows the potential for hemodynamic deterioration during tachycardia in susceptible individuals. This may limit its utility in patients with angina plus left ventricular dysfunction (30). Heterogeneity between effects of metoprolol and sotalol may also be important, illustrated by the deleterious effects of d-sotalol (31). Furthermore, the methodology used in this study might well prove useful both during preclinical studies and in phase 1 human investigations of new cardioactive agents to identify potential for hemodynamic deterioration during tachycardia. Acknowledgments The authors acknowledge the assistance of Professor Richard Jarrett, Department of Statistics, The University of Adelaide. The authors thank the staff of the Cardiac Catheterization Laboratory, The Queen Elizabeth Hospital, for assistance with the experimental procedure, and Mr. J. Pearce and Mr. B. Braysher for assistance with the mathematical mechanical restitution curve model. Reprint requests and correspondence: Dr. John D. Horowitz, Cardiology Unit, The Queen Elizabeth Hospital, 28 Woodville Road, Woodville, SA 5011, Australia. E-mail: jhorowitz@ medicine.adelaide.edu.au. REFERENCES 1. Sharma AD, Purves P, Yee R, et al. Hemodynamic effects of intravenous procainamide during ventricular tachycardia. Am Heart J 1990;199:1034 – 41. 2. Rankin AC, Rae AP, Cobbe SM. Misuse of intravenous verapamil in patients with ventricular tachycardia. Lancet 1987;ii:472– 4. 3. Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med 1991;324:781– 8. 4. Danish Multicenter Study Group on Verapamil in Myocardial Infarction. Verapamil in acute myocardial infarction. Am J Cardiol 1984; 54:24E– 8E. 5. Andersson B, Stromblad SO, Lomsky M, Waagstein F. Heart rate dependency of cardiac performance in heart failure patients treated with metoprolol. Eur Heart J 1999;20:575– 83. 6. Koch-Weser J, Blinks JR. The influence of the interval between beats on myocardial contractility. Pharmacol Rev 1963;15:601–52. JACC Vol. 48, No. 6, 2006 September 19, 2006:1234–41 7. Seed WA, Walker JM. Review. Relation between beat interval and force of the heart beat and its clinical implications. Cardiovasc Res 1988;22:303–14. 8. Chappell SP, Henderson AH, Lewis MJ. Frequency-dependent depression of myocardial contractility by slow calcium channel blocking drugs. Eur J Pharmacol 1985;110:129 –32. 9. Borzak S, Murphy S, Marsh JD. Mechanisms of rate staircase in rat ventricular cells. Am J Physiol 1991;260:H884 –92. 10. Twidale N, Rayner TE, Menadue MF, et al. Atrial natriuretic factor release during rapid ventricular pacing: interplay between autonomic and hemodynamic stimulants. Am Heart J 1993;125:1638 – 44. 11. Aroesty JM, McKay RG, Heller GV, et al. Simultaneous assessment of left ventricular systolic and diastolic dysfunction during pacinginduced ischemia. Circulation 1985;71:889 –900. 12. Linhart JW, Hildner FJ, Barold SS, Lister JW, Samet P. Left heart hemodynamics during angina pectoris induced by atrial pacing. Circulation 1969;40:483–92. 13. Hamer AWF, Rubin SA, Peter T, Mandel WJ. Factors that predict syncope during ventricular tachycardia in patients. Am Heart J 1984; 107:997–1005. 14. Ritchie RH, Wuttke RD, Hii JTY, et al. The force-interval relationship of the left ventricle: quantitative description in patients with ischemic heart disease. J Card Fail 1995;1:273– 84. 15. Zeitz CJ, Ritchie RH, Jarrett RG, et al. The positive inotropic effects of milrinone but not of digoxin are attenuated at short cycle lengths. J Cardiovasc Pharmacol 2000;35:427–33. 16. Barry WJ, Levin DC, Green LH, et al. Left heart catheterization and angiography via the percutaneous femoral approach using an arterial sheath. Catheter Cardiovasc Diagn 1979;5:401–9. 17. Cotton JM, Kearney MT, MacCarthy PA, et al. Effects of nitric oxide synthase inhibition on basal function and the force-frequency relationship in the normal and failing human heart in vivo. Circulation 2001;104:2318 –23. 18. Bourdillon PD, Canepa-Anson R, Rickards AF. Hemodynamic effects of intravenous metoprolol. Am J Cardiol 1979;44:1195–200. 19. Ritchie RH, Wuttke RD, Stafford I, Horowitz JD. Relation between acute myocardial uptake and hemodynamic and electrocardiographic effects of metoprolol in humans. J Cardiovasc Pharmacol 1994;23:57– 65. Ritchie et al. Negative Inotropes Modulate the Force-Interval Relationship 1241 20. Hutton I, Lorimer AR, Hillis WS, et al. Haemodynamics and myocardial function after sotalol. Br Heart J 1972;34:787–90. 21. Ritchie RH, Sallustio BC, Hii JTY, Horowitz JD. Acute myocardial uptake of d- and l-sotalol in humans. Relation to hemodynamic and electrophysiological effects. J Cardiovasc Pharmacol 1998;31: 885–93. 22. Cooper IC, Fry CH. Mechanical restitution in isolated mammalian myocardium. species differences and underlying mechanisms. J Mol Cell Cardiol 1990;22:439 –20. 23. Wier WG, Yue DT. Intracellular calcium transients underlying the short-term force-interval relationship in ferret ventricular myocardium. J Physiol 1986;376:507–30. 24. Ross J Jr. Adrenergic regulation of the force-frequency effect. Basic Res Cardiol 1998;93 Suppl 1:95–101. 25. De Pauw M, Vilaine JP, Heyndrickx GR. Role of force-frequency relation during AV-block, sinus node block and beta-adrenoceptor block in conscious animals. Basic Res Cardiol 2004;99:360 –71. 26. Holubarsch C, Schneider R, Pieske B, et al. Positive and negative inotropic effects of DL-sotalol and D-sotalol in failing and nonfailing human myocardium under physiological experimental conditions. Circulation 1995;92:2904 –10. 27. Pieske B, Sutterlin M, Schmidt-Schweda S, et al. Diminished postrest potentiation of contractile force in human dilated cardiomyopathy. J Clin Invest 1996;98:764 –76. 28. Hasenfuss G. Alterations of calcium-regulatory proteins in heart failure. Cardiovasc Res 1998;37:279 – 89. 29. Richard S, Leclercq F, Lemaire S, Piot C, Nargeot J. Ca2⫹ currents in compensated hypertrophy and heart failure. Cardiovasc Res 1998;37: 300 –11. 30. Hansen JF. Treatment with verapamil after an acute myocardial infarction. Review of the Danish studies on verapamil in myocardial infarction (DAVIT I and II). Drugs 1991;42 Suppl 2:43–53. 31. Waldo AL, Camm AJ, deRuyter H, et al. Effect of d-sotalol on mortality in patients with left ventricular dysfunction after recent and remote myocardial infarction. The SWORD Investigators. Survival With Oral d-Sotalol. Lancet 1996;348:7–12.