Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
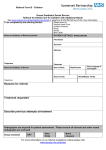
King's College Hospital NHS Foundation Trust. Dental Institute Dental Waiting List Office, Denmark Hill, London SE5 9RS email [email protected] Tel 020 3299 4988 Specialist Opinion only Specialist treatment Undergraduate treatment WHICH DISCIPLINE SHOULD SEE THE PATIENT: TICK ONE ONLY* Restorative -general Periodontology Endodontics Removable prosthodontics Fixed prosthodontics Tooth surface loss Hypodontia, cleft etc Other, please specify REASON FOR REFERRAL & RELEVANT MEDICAL / DENTAL HISTORY Radiographs: please include any relevant radiographs taken in past 12 months Yes No Is there any other information we need to know? General Medical Practitioner This information is required to identify the Primary Care Trust of referred patients and to enable the GP to be copied into relevant correspondence by the consultant. Patients’ should bring the details of their GP to the hospital when they attend Name: Practice Name & address of GP: Review date: March 2013 A. Patient Personal Details Date of Referral: Patient’s Date of Birth: Sex (please tick) Male Female Patient’s Surname: Patient’s Forename: Surname (family name) at birth (if different): Contact Address: House Name or Number and Street Name Town or City: Postcode: Daytime Phone: Mobile Phone: Home Phone: e-mail Address: Does your patient need to communicate in a language or mode other than English? If yes, please specify: GDP Stamp / Address I confirm that this patient referral comes within the current referral guidelines issued by Kings Dental Institute Please tick box to confirm Print Name (Dentist) Signed: (Dentist) if manual copy Review date: March 2013