Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
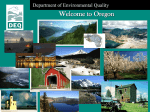
MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS January 2016 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Table of Contents Introduction and Rationale ......................................................................... 2 Objectives ................................................................................................... 3 Chapter 1: Service Tiers .............................................................................. 4 Chapter 2: Calling the member.................................................................... 7 Chapter 3: Deliverables for each Tier .......................................................... 9 Appendix A: Vignette Guidelines ............................................................... 10 Page 1 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Introduction and Rationale As you learned from Module 1a, Best Doctors offers a variety of services to best meet a member’s needs. In some instances, a case will be triaged to a specific service line (e.g. InterConsultation) before your involvement. The MA, the Lead MD or other operational team members involved in the case, may do this. In these instances you should always look at the totality of information provided and consider whether a different service line would provide the member with the information they need in a more efficient way (e.g. a less intensive service line). For some cases, you may be asked to triage cases at the pre-intake stage. This will require reviewing a pre-intake form completed by an MA. As much as possible these will be organized by specialty (e.g. GI, ID, Cardiology, Oncology) so that physicians can select those they are best able to support. In other cases you make actually do an intake and triage while on the telephone with the member. In all cases, you should triage the case to the tier that tis most efficient. Efficiency in this context means choosing the service line that is able to meet the member’s needs, with high quality, in the minimum amount of time. In recognizing that two key areas that impact member satisfaction are the quality of what we deliver and the timeliness, you should also choose the most streamlined tier that can meet the member’s needs. The greatest drivers of extended case timelines are the collection of extensive medical records and the integration of these records into detailed summaries. Therefore, service lines that utilize no records or only focused records, are generally more efficient. This module will guide you through general service tiers, provide guidance with regard to triage, and provide guidance as to how to perform an intake/triage call. Page 2 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Objectives At the end of this manual, you will: Understand the rationale behind MD Triage Understand the different service tiers Understand the requirements and deliverables for each tier Be able to choose between the different tiers Be able to call a member to perform an Intake/Triage Page 3 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Chapter 1: Service Tiers An outline of service tiers are below and shown in Figure 1. Please note that services at Best Doctors change dynamically as needed to better serve our members and sometimes based on specific needs from large clients. So, when you start working the names of services (e.g. Tier 1 or Tier 2) may change and elements of Tiers (e.g. how many records or questions) may also change. You will be informed and should always ask your Lead if uncertain. As you review the tiers below please note that with each subsequent tier that there is increasing resource intensity, complexity of workflow, and record collection. This leads to longer timelines in general. Therefore the lowest tier that can meet the member’s needs should be selected. Service Tiers Tier 1—Real-time Clinical Information o The Associate Physician provides general information to answer a member’s query without providing any specific management recommendations o The AP writes a brief summary of the discussion which is furnished to the member and also kept for internal records/auditing o Whenever possible pre-approved educational materials are sent to the member o If applicable (and available) you can suggest a Find Best Doctor (FBD) which identify local specialists that the member can see in person Tier 2—Expert Review Without Records o The AP/MA creates a clinical vignette from the intake call. o No medical record collection required. o Expert input is obtained on 3-5 questions in the vignette, and specific recommendations can be provided o No UPW/BDRS o No report discussion (RD) Tier 3—Expert Review With Focused Records o The AP/MA creates a clinical vignette from the intake call and directs MRC o Up to 3 records (labs, single imaging study, 1-2 office notes) are collected o Defaults to member MRC (specialist in records collection) o Vignette and primary records are furnished to the expert o Expert input is obtained on 3-5 questions in the vignette, and specific recommendations can be provided o No UPW/BDRS Page 4 of 19 Best Doctors o MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS RD with MA Tier 3R— Expert Review With Focused Records Including Primary Imaging o The AP/MA creates a brief clinical vignette from the intake call o Defaults to member MRC (imaging and original report required) o 2 questions posed: Please provide your interpretation of the imaging Any additional imaging recommended? o Radiology report furnished to the member. o No UPW, BDRS o No RD Tier 4— Expert Review With Extended Focused Records o The AP/MA performs an intake and creates a clinical vignette o More extensive records, (up to 4 imaging studies and up to 3 sets of office notes), are collected o Clinical vignette and primary records are furnished to the expert o Expert input is obtained on 4-7 questions in the form of a Best Doctors Report (BDR) which is sent ot the member o +/- UPW, no BDRS o MD or MA RD Tier 5—Formerly known as InterConsultation (See Module 2 – MD Intake) o The AP performs an intake and completes the intake template o The AP directs MRC with regard to record collection o The AP provides extensive input with regards to expert selection o Extensive records are collected o After record review a formal Clinical summary (CS) is created by the AP o CS and imaging are furnished to the expert o Expert input is obtained on 6-12 questions o +UPW, + BDRS o MD RD Page 5 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Figure 1 – Service Tiers MEC +/- Clinical Support AP/MA Calls Member Schedules with AP/MA with Specialty Matching Member Ini ates Service Specialty-matched MD Determines Op mal Service Tier No MRC Tier 1 Real- me Clinical Informa on Internal Metrics Summary of Discussion and Educa onal Materials to Member Tier 2 Expert Review based on Vigne e Clinical Vigne e with 3-5 ques ons, Case approval Increasing complexity MRC Tier 3 Expert Review based on Vigne e and Limited Records Tier 3R Radiology Review based on brief vigne e and imaging Clinical Vigne e with 2-5 ques ons, Records for collec on (≤3), Case approval +/- UPW MA RD for T3 Tier 4 Expert Review based on Vigne e and Extended Records Tier 5 Expert Review based on Formal Case Summary and Extended Records Clinical Vigne e with 4-7 ques ons, Records for collec on, Case approval & BDRS UPW AP/MA RD Case Summary with 6-12 ques ons, Records for collec on Expert type Case approval & BDRS UPW AP RD Page 6 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Chapter 2: Calling the member Calling the member through the MD Triage model will follow the same scheduling and calendar process as the MD Intake service line (see Module 2). You will receive an invitation and an intake template from the Member Experience Coordinator (MEC). Your call should follow the same script as an MD Intake call and is outlined below. 1. Prepare a. Review the intake that was sent to you by the MEC – what was the primary question? If needed, review relevant background medical information to help you focus your questions. b. Call the member at the scheduled time c. Introduce yourself i. State your name and your role in the case. Let the member know that you have been involved and are familiar with their case and the BD report. 1. “Hi my name is David Harrison and I am a physician at Best Doctors. I am calling to do an intake for your case. Is now a good time to talk?” 2. “I would like to start by introducing myself. My role in your case is that of a Best Doctors Associate Physician. The purpose for this phone call is to discuss the issue or issues that you would like us to address and I will provide you with some information. At the conclusion of the call I will send you a summary of our discussion and some educational materials. We may also determine that additional information and review is necessary and if so we will discuss the next steps at the conclusion of the call.” 3. In addition to my work with Best Doctors, I am a . . . ” 4. “Many times questions come up during this discussion. Most of the time I can answer them but if not, we will make a plan to make sure they are answered. d. Set expectations – the member should understand what type of information you are able to provide and make it clear that you are not providing medical care, just information and education. Also clarify that your comments to not replace the recommendations of their treating doctors. Page 7 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS e. Take a history as you would in clinical practice. Use the Intake Template to document your discussion. Try to focus the member on the 1 or 2 key issues for which the need help. Try to focus on the key questions. f. Summarize the discussion and determine next steps i. “Thank you, this has been a very helpful discussion. I would like to summarize briefly if ok with you. Please let me know if I misstate anything. My understanding is that Your history until now is as follows” ii. Then review their questions. Discuss general information, as you are comfortable. Whenever possible refer to educational materials that can be sent to the member at the conclusion of the call (see Appendix A). iii. Based on this discussion determine the optimal tier for the case. If you believe expert review will be necessary, triage to the most efficient Tier (see Figure 1) that will meet the member’s needs as quickly as possible. g. If necessary based on your selected tier, review records to be collected i. Try to understand what tests (e.g. biopsies, imaging) have been done and where ii. Try to understand which doctors have been involved. Try to understand which specialist if any has been driving the current treatment plan h. At the end, you can ask: “Are there any other questions that we did not cover?” i. Review next steps (as appropriate for your selected tier) and general timelines for communication. i. Sending a call summary and educational materials ii. Record collection iii. Expert review iv. Report discusssion j. Close the call Page 8 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Chapter 3: Deliverables for each Tier Specific deliverables outlined below are covered in subsequent modules (e.g. Case Summary, BDRS). Please make sure to review all modules in the curriculum. If you have any questions contact your lead. For each tier make sure that the number of records and questions matches the guidelines provided in Chapter 1. Tier 1—Real-time Clinical Information o Write a summary of your conversation, include, “questions to ask your doctor” o Select pre-approved education to send to the member o Email the team when the call is completed and be specific about any “next steps” needed (e.g. FBD) Tier 2—Expert Review Without Records o Write a clinical vignette of your conversation (see Module on writing a clinical vignette) o Email the team when the call is completed, identify the case as Tier 2, select the specialty of the expert to review the case Tier 3—Expert Review With Focused Records o Write a clinical vignette of your conversation (see Module on writing a clinical vignette) o Email the team when the call is completed, identify the case as Tier 3, select the specialty of the expert to review the case, identify records for collection o The MA involved with provide a report discussion at the end of the case Tier 3R— Expert Review With Focused Records Including Primary Imaging o Write a clinical vignette of your conversation (see Module on writing a clinical vignette) o Email the team when the call is completed, identify the case as Tier 3R, select the type of imaging expert to review the case, identify records for collection Tier 4— Expert Review With Extended Focused Records o Write a clinical vignette of your conversation (see Module on writing a clinical vignette) o Email the team when the call is completed, identify the case as Tier 4, select the type of expert to review the case, identify records for collection o You may be asked to perform a Report Discussion at the conclusion of the case (See Report Discussion Module) Tier 5—Formerly known as InterConsultation (See Module 2 – MD Intake) o Complete the intake template with extensive guidance for record collection o Email the team when the call is completed, identify the case as Tier 5 o Identify the type of expert and work with PSD to select the specific expert o Create a clinical summary o At the end of the case complete the BDRS and UPW (see Report Approval module) o Perform a Report Discussion (see Report Discussion Module) Page 9 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Appendix A: Vignette Guidelines Writing the Vignette Prior to submitting a case to the Lead, a vignette should be written based on a telephone conversation with the member. We ask that the vignette is written in flowing prose and that it is checked for grammar and spelling before submission. Please try to write this vignette as if it were going to be written about and read by a family member without clinical expertise; please use patientfriendly language and avoid medical abbreviations. Please also try to write the vignette as if you were preparing to present the information directly to an expert; non-standard abbreviations, sentence fragments, mis-spellings and punctuation errors should be avoided. When writing vignettes, please note that the member information section should always have the member’s height, weight, and body mass index (BMI) as well as a complete medication list, including dosages. Please make sure to check the spelling and names of medications. Often a patient doesn’t report a medication name accurately, and might say that he is taking “Armor” for his thyroid when the product is called “Armour Thyroid” (please note full and correct spelling of the product). Attention to detail here is appropriate, as this is the only section that the Lead cannot edit after the case is submitted. The chronological description of illness should be a concise summary of the case, 2-3 paragraphs at most (EU vignettes should be limited to 1 page of a Word document). The opening sentence should briefly summarize the case and should tell the reader where the questions are going and what type of physician should address them. For example, starting a vignette with “This is a healthy 56 y/o man who eats well and works out three times a week” is not a helpful opening sentence for a vignette about a member with an elevated PSA who has questions about a prostate biopsy. A better leading sentence might be: “This is a 56 year old gentleman with an elevated PSA who has questions about whether or not he should have a prostate biopsy.” As another example, an opening sentence that reads: “Early 2015 was scheduled for a routine colonoscopy” could be improved grammatically and is not helpful for a case that is about atrial fibrillation. A better leading sentence might be: “This is a 61 year old gentleman with asymptomatic Page 10 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS atrial fibrillation and questions about management options.” Always include the age, and we prefer that the words “gentleman” or “man” or “woman” are used to indicate gender, rather than the generic “member.” Likewise, when referring to the individual, please use the gender-specific pronouns “he” or “she” and please refrain from using the repetitive and impersonal phrases “member says” or “member reports.” For pediatric cases, please write from the perspective of the family (e.g. “the child’s mother reports that...”) In general, race is not necessary unless it is clinically relevant, e.g. a member of Ashkenazi Jewish descent asking about the risk of cystic fibrosis or breast cancer. Lastly, as a tip that may help to distinguish AtEs from other medical histories that are not usually patient-facing, please be careful about (and avoid if possible) the phrase “the member denies.” For those who are not accustomed to reading clinical histories, the term “denies” often has an accusatory and confusing connotation. When writing the vignette, try to focus on one topic in order to facilitate a focused expert selection. For example, if a member calls with questions about a thyroid medication and also about routine mammography, we would need to engage multiple experts for the AtE (an endocrinologist cannot comment about mammography), which is not ideal. We could send a case like that to an internist to comment on both issues, but this would sacrifice the optimal expertise of the responding expert. As a general strategy, if there are multiple issues, please help the member select the issue of highest priority and process an ATE for that issue; if needed, we can open a subsequent case for a second issue if absolutely necessary. The chronological description of illness should include symptoms and essentially have all of the information for the case, except social, family, and past medical history (unless relevant to a case, e.g. asking about breast cancer screening with multiple close relatives who had breast cancer). If there is a further description of symptoms needed that is not covered in this section, it can go in the symptoms section, though that is usually not necessary. An exception might be fully describing knee pain, e.g. location, exacerbating/alleviating factors, positions that cause problems, radiation of pain, associated symptoms. If you described the symptoms well in chronological description of illness, simply write “as above” in the symptom section. Try to use your clinical knowledge to ask the member additional questions about their symptoms and to go past simply writing down what a member says. Page 11 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Examples include chest pain and sleeping problems. For chest pain, we want to know when it occurs, what triggers it, exacerbating/alleviating factors, whether shortness of breath is associated, whether palpitations are associated, family history of arrhythmias/cholesterol issues/atherosclersosis/myocardial infarctions/strokes, work-up to date, etc. For sleep, we need to know when they go to bed, when they get up, typical amount of sleep at night, daytime sleepiness, restless legs/associated symptoms, whether they nap (and if so, for how long), medications tried in the past, workup to date, etc. The past medical history section should be in prose as well and should start with “The member has a past medical history of… He/she has a past surgical history of…” This is where family history should go, as well as social history (it is better to put in too much information if you are unsure of what to include, as we can always remove extraneous information). For any of the medications that the member lists, make sure you have a corresponding diagnosis listed under the past medical history section. In some cases, the past medical history section will say “none” though the medication list will include an antidepressant, a proton pump inhibitor, and a statin. The lists should correlate. Questions should be limited to 7 questions at most. If you feel that the member is asking more, reach out to the Lead to help trim the list or to offer additional compensation when there is a legitimate need for more than 7 questions. As a tip when writing the question section, we recommend use of the following phrase before the question list: “Please address answers to the member (write “family” or “mother” or “father” if it is a pediatric case) in patient-friendly language.” From there, number the questions and try to not write questions that require prescriptive or definitive answers. For example, instead of asking “Does the member need surgery?” consider writing “What are the indications for surgery for this condition and what are the pros and cons of surgery?” Or, instead of “Does the member have gout?” consider “Given the limited information in the vignette, do you think that gout is a possible diagnosis for this member, and what other diagnoses would you consider in this case?” For the last question for all cases, please ask: “Please provide any additional comments and links to patientfriendly resources that you think this member might find useful (again, write “family” if it is a pediatric case). Do not promise members that a specific member-provided question will definitely be asked as provided - for medical Page 12 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS appropriateness, the Lead may need to edit or exclude a member-provided question from time to time. Appendix A: Case that is not a good choice for a vignette based review This case is sub-optimal for ATE for several reasons. First, there is a significant amount of diagnostic testing performed that is “described” in the vignette. These reports have impact potential and should be directly reviewed for this case. There is also a potential high impact diagnosis here- a bowel obstruction could be due to inflammatory bowel disease or cancer. Hence, a full IC is a good choice here. “Member is a 50 year old male living in the UK reportedly diagnosed with Diverticulitis in March 2015. Early 2015 (before his diagnosis) he had an episode of abdominal pain. The pain was located in the mid-lower quadrant (suprapubic region) and radiated to left hand side; it was a stabbing-like pain and was tender to touch. A full bladder aggravated the pain, “it felt like the pressure of a full bladder was pressing on his bowel”. The GP prescribed an antibiotic (name unknown) and after 2 to 3 days the pain completely resolved. He was referred to a specialist and underwent a flexi-sigmoidoscopy. This test confirmed the presence of diverticula although the doctor was unable to pass the camera through the entire colon because of a “blockage”. The specialist had said he will need to have a CT scan in order to see the rest of the bowel but that there were no other issues or abnormalities found. After the endoscopy procedure he suffered a similar episode of abdominal pain; this time “more intense”. Again the GP prescribed an antibiotic (name unknown) and after 2 to 3 days the pain completely resolved. He also took a 30 day course of the anti-spasmodic drugs Audmonal. He has regular bowel movements that occur once or twice a day. He denies any problems with passing urine and his urine is clear. He has a past medical history of Asthma controlled by Flixotide and Serevent daily. His surgical history is: circumcision (1995) and gallbladder removal (2003). He is a non-smoker. He exercises doing cardiovascular training 1 ½ hours per week. He works as a construction manager and has admitted to being under unusual amounts of stress between January and March of this year. He stress levels are better now. He is current height is 5’9 ½ and weighs 295 lbs. BMI: 42.9. He says he is allergic to “XRay dye”; when they removed his gallbladder he developed “nausea and sweats” after the injection of contrast medium. He follows a regular diet but since his diagnosis he has stop eating certain foods (bread and fruit) and stop drinking alcohol. “I’m currently managing it with the aid of anti-spasmodic drugs Audmonal (60 mg) three times a day and have no real Page 13 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS symptoms. In the past 8 weeks I have had a reaction to eating fruit whereby I have very bad diarrhea after eating fruit”. He has contacted Best Doctors with general question regarding his condition. Questions (please address answers to the member, in patient-friendly language) 1. Please provide an overview of Diverticulitis in layman’s terms, including how it is treated. 2. How would you further evaluate this member and do you feel that any testing is indicated at this time? 3. What are possible causes of a blockage during a flexi-sigmoidoscopy? 4. What is a CT scan, what does it entail? 5. What type a diet is recommended for a person with Diverticulitis? Are there certain foods that should be avoided? Can I continue eating fruit? 6. Please provide any further comments that you feel would be helpful for this member. “ Appendix B: Case that is a good fit for a vignette based case This case is a better choice for ATE (though it is not written the way we would like an ATE to be written – the point of this Appendix B is the content choice for the ATE). There is a single, focused issue at hand. While there was diagnostic testing, it was interpreted as normal as would be expected in the clinical scenario. Symptoms are well described and the proposed plan from the treatment team is clear. Questions are focused and easily addressed by the expert based on available data. “This is a 34 year old man living in Australia. The patient has had acid reflux on and off for a period of 8 years. About 4 years ago he had it constantly for about a year. He took a supplement called Liv 52 liver support and the condition eased. In the last month he has been regularly getting reflux again with acid refluxing into his mouth, along with stomach cramps and a ‘churning’ sensation in his abdomen as if he needs to open his bowels. He has had blood tests, CT scan, and a breath test for helicobacter pylori which have not shown any abnormalities. His GP has suggested it may due to something he is eating and he is avoiding spicy foods and drinking warm water. His GP has suggested that the next step would be to have endoscopy examinations attended. Page 14 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS The member has not had endoscopy attended in the past and is anxious about undergoing this type of procedure. MEDS: Nil medications PMH/PSH renal stones Wt 82 kg Ht 178 cm BMI 25.9 ALLERGIES-Nil Known This member wishes to ask… 1/What is the risk of cross infection from a previous patient undergoing endoscopy with the same instrument. How is the instrument sterilized? 2/Please explain what I am to expect for an upper endoscopy and a lower endoscopy-what will happen to me? What are the risks/side effects associated with endoscopy. 3/ What information can a doctor obtain from performing endoscopy? Is there an alternative to endoscopy that will give you the same information? Appendix C: Example of a case before and after editing This version needing editing! Member reports that just prior to June 13, 2015 Member woke having blurry vision to right eye that cleared throughout the day. June 13, 2015 Member reports waking up to binocular double vision, Member states that if she were to cover one eye the double vision would be eliminated. She also complained of confusion and fogginess, insomnia, rapid heart rate, chest pain and diarrhea. Member reports head tingling with facial pressure to right upper quadrant of her face. Member states she has a long history of sinus issues; thinking this is sinus related she started on antibiotics (Augmentin) in which she had at home and a decongestant (Sudafed). Member states condition was not resolving and she called her PCP for an appointment for evaluation; PCP office directed to ER for evaluation and treatement. ER performed a CT scan which Member states was unremarkable. Member sent home to continue on Augmentin. Member evaluated by an Optometrist who stated that 2 of the nerves were not working and that she required a referral to a neurologist or a neuro-opthamologist. Member then evaluated by an ENT who repeated the CT scan which again presented unremarkable. ENT did a nasal scope which Member reports was normal. ENT referred Member to an ENT surgeon who evaluated the Member on July 10, 2015 who states that the sinuses are within normal limits but she did have a deviated septum, and cobblestoning secondary to GERD. Member reports that the surgeon did not feel the Page 15 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS surgery for the deviated septum would be beneficial and to have the MRI with and without contrast on July 23, 2015 and consult with Neurologist and or neuro ophthalmologist. Member reports seeing neuroophthalmology on Sept 18, 2015 and on a wait list for Neurology. Member reports speaking to a personal friend who is a RN who had similar symptoms and was Vitamin B12 deficient; Member states she started taking Vitamin B12 7/17/15. On 7/18/15 Member reports symptoms greatly improved over the course of the weekend; increased energy, fogginess resolved, insomnia improved, rapid heart rate and chest pain resolved. Member also stopped Zantac on 7/16/15 and denies further diarrhea. Member reports that the double vision has improved but remains at about 20%. Member states she had a headache to the right side of her head last evening 7/19/15. Edited version (Please note the complexity of this case. Depending on the questions that the member has, a follow-up IC may be recommended for detailed records review and personalized recommendations) This is a 53 year old woman with a long history of sinus problems who awoke in early June with blurry vision in the right eye that cleared throughout the day. On June 13, 2015, she had double vision. If she were to cover one eye the double vision would be eliminated. She also complained of confusion and “fogginess”, insomnia, rapid heart rate, chest pain and diarrhea. She reported head tingling with facial pressure to the right upper quadrant of her face. Because of her sinus history, she started antibiotics (Augmentin) that she had at home and a decongestant (Sudafed). Her symptoms did not resolve. She was directed by her PCP to the ER, where a CT scan (presumably of the head) was unremarkable. She was sent home to continue on Augmentin. She was evaluated by an Optometrist who stated that "2 of the nerves were not working" and who suggested a referral to a neurologist or a neuro-ophthalmologist. She was evaluated by an ENT who repeated the CT scan which again was unremarkable. Nasal endoscopy was normal. An ENT surgeon evaluated her on July 10, 2015 and told her the sinuses were within normal limits but that she did have a deviated septum, and cobblestoning secondary to GERD. The ENT surgeon did not feel that surgery for the deviated septum would help her symptoms. The surgeon did suggest an MRI with and without contrast (presumably of the brain) and a consult with a neurologist and/or neuroophthalmologist. A friend told her she had similar symptoms and was found to be Vitamin B12 deficient, so the patient started taking Vitamin B12 recently. A few days later, her symptoms greatly improved, with increased energy, improvement in her mental fogginess and insomnia, and resolution of her rapid heart rate and chest pain. She reports that the double vision has improved but remains at "about 20%." Appendix D: Example of a case before and after editing Version Needing Improvement Member states since about April she has been going through with some stressful situations. Member states she was experiencing chest pain and SOB. Member states all cardiac concerns were ruled out and it was thought to be acid reflux related. Member states stressful situations arose again in July and August, with symptoms. In August member noticed that she was frequently clearing her throat Page 16 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS Member states she has been taking gas X, alka seltzer chews and pepcid ac "at least one medicine daily, sometimes to relieve the symptoms and other times to prevent the symptoms from coming on" Member mentioned it to her endocrinologist who referred member to ENT. ENT - "inflammed voice box d/t acid reflux" Member states she was prescribed Pantoprazole 40mg BID for an 8 week course. Member states she is concerned about the high dose of the medication and is worried she will be stuck taking the medication long term to control her symtpoms. Member has not started to take the medication Symptoms: Symptoms are better or worse depending on the stressful situations that she is dealing with. Chest pain would be present after eating meals and at night the chest pain would also be present or more pronounced". Currently member states she is careful about what she eats and doesn't eat late at night to help relieve the symptoms. Member took out coffee, tea, wine, spicy foods, and sour foods for her diet. "Cut back on fruits and vegetables; eating more eggs, fish and rice" Will take anti-acid chews and a gax-X at night to prevent acid buildup over night. Need to Clear throat. Worse first thing in the morning, and during the day after taking for long periods of time" Member states MD wants her to take the Pantoprazole to reduce the inflammation on her voice box. Past Medical History Osteopenia Hypothyroidism Seasonal allergies Questions What is the recommended dose for Pantoprazole? When would it be necessary to prescribe the medication Pantoprazole 40mg BID? Do you think that Pantoprazole 40mg Once daily would be effective for member's symtpoms and should be trialed before doing BID? if so, when would you recommend increasing to 40mg BID? After the 8 weeks of Pantoprazole will member's body become dependent on the medication? What can member expect after taking the drug for the 8 weeks time? If it proves to be helpful will her boby then need the medicaiton to further prevent symptoms. If it helps reduce the inflammtion on the voice box will the inflammation then come back once the drug is stopped? Is there a concern with taking the other 3 medications long term? Gas X, Pepcid ac and alka seltzer on a daily basis as long as it is taken as recommended? Are there any negative side effects associated with Pantoprazole and osteopenia? Page 17 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS What complications might arise from taking Pantoprazole 40mg BID for 8 weeks, if any? Edited version This is a 57 year old woman with chest pain and shortness of breath who has been diagnosed with gastroesophageal reflux and prescribed pantoprazole. Since April, the member has been experiencing “stressful situations.” She has had chest pain and says that cardiac concerns were ruled-out and that the pain was thought to be related to acid reflux. She experienced additional stress in July/August, again causing symptoms. In August she also noticed that she was frequently clearing her throat. The member has been taking Gas-X, Alka Seltzer chews, and Pepcid AC "at least one medicine daily, sometimes to relieve the symptoms and other times to prevent the symptoms from coming on." The member saw her endocrinologist (she has a history of hypothyroidism and osteopenia) and mentioned her symptoms, at which point she was referred to ENT. She says the otolaryngologist told her that she had an "inflamed voice box due to acid reflux". She was prescribed an 8 week course of pantoprazole 40mg twice daily. The member is concerned about the high dose of the medication and is worried that she will have to take it long-term to control her symptoms. She has not started to take it. Symptoms The member's symptoms vary depending on how much stress she is under. She can have chest pain present after meals and at night as well. Currently she is taking care with what she eats and does not eat late at night to help her symptoms. She has eliminated coffee, tea, wine, spicy foods, and sour foods from her diet and also cut back on fruits and vegetables and eats more eggs, fish, and rice. She takes anti-acid chews and a Gax-X at night to prevent acid buildup overnight. The member also feels a need to clear her throat, worse first thing in the morning and during the day after talking for long periods of time. Past Medical History The member has a past medical history of osteopenia, hypothyroidism, and seasonal allergies. Questions Please address answers to the member in patient-friendly language. 1. What is the standard dose of pantoprazole for the treatment of gastroesophageal reflux? When would it be necessary to prescribe 40mg twice daily? Could a lower dose be tried before increasing to twice daily, and if so, how long would you wait to see if the symptoms were relieved before increasing the dose? Page 18 of 19 Best Doctors MD TRAINING MANUAL – MODULE 1B CASE TRIAGE AND TIERS 2. In general, do patients become “dependent” on pantoprazole after taking it for eight weeks? 3. What can the member expect after taking the drug for the 8 weeks? If it proves to be helpful, would you anticipate that she will continue to need the medication to further prevent symptoms and/or to reduce inflammation in the voice box? 4 Is there a concern with taking Gas-X, Pepcid AC and Alka Seltzer long term on a daily basis if taken as directed by the packaging? 5. Has pantoprazole been shown to cause bone loss or worsen osteopenia? What other complications/side effects might occur from taking pantoprazole 40mg twice daily for 8 weeks, if any? 6. Please provide any additional comments and links to patient-friendly resources that may be helpful for this member. Page 19 of 19