Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
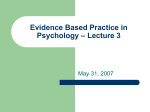
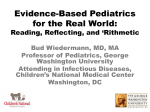
The Journal of Pain, Vol 16, No 2 (February), 2015: pp 116-123 Available online at www.jpain.org and www.sciencedirect.com A Review of the Use of the Number Needed to Treat to Evaluate the Efficacy of Analgesics Nathaniel Katz, Florence C. Paillard, and Richard Van Inwegen Analgesic Solutions, Natick, Massachusetts. Abstract: Standardized measures of efficacy are needed to compare analgesic efficacy across trials. The number needed to treat (NNT) is considered a statistically robust and readily interpretable measure to rank the efficacy of treatments, including analgesics. The NNT has become widely utilized to compare the efficacy of chronic pain treatments, helping physicians make treatment decisions and informing decisions for market access, reimbursement, and treatment guidelines. However, the NNT is associated with specific weaknesses in calculation and interpretation not associated with other methods for integrating trial data. These weaknesses include distortions in calculation as placebo effects approach treatment effects, with the possibility of infinite values; difficulties in estimating the NNT’s confidence interval; and difficulties in interpretation. The NNT also requires selecting cutoffs of the original variable for dichotomization, with the NNT often changing depending on the cutoff. The NNT also suffers from problems common to other placebo-adjusted endpoints, including being sensitive to study-related and external factors (eg, year of publication). Therefore, clinicians and other stakeholders need to be aware of these issues to correctly calculate, use, and interpret the NNT. Nevertheless, efficacy, as measured by any variable, is only one aspect of a treatment to be considered in determining its place in therapy. Perspective: The NNT has become widely utilized to compare the efficacy of chronic pain treatments. This article reviews the uses of the NNT and the potential problems associated with its calculation, use, and interpretation. Clinicians should be aware of these issues when interpreting clinical trial data based on the NNT. ª 2015 by the American Pain Society Key words: Number needed to treat, analgesics, efficacy, clinical trials, chronic pain treatment. T he number needed to treat (NNT) was devised in 1988 by Laupacis et al29 as a single unitary measure of a drug’s efficacy that was meant to provide an intuitive means for evaluating the relative efficacy of different drugs in order to rank them as to their efficacy.33 Like any other method that evaluates the relative efficacy of treatments, the NNT is dependent on comparing data across randomized double-blind controlled trials, the gold standard in clinical research. The efficacy of the drug being studied is measured as incremental benefit above that in the placebo group and is typically quantified by the difference between groups in The authors received a grant from Janssen Pharmaceuticals to support independent writing of this review. The authors declare having no financial relationship to the work. N.K. and R.V.I. are employees and F.C.P. is a contractor of Analgesic Solutions. Address reprint requests to Florence C. Paillard, PhD, Analgesic Solutions, 232 Pond St, Natick, MA 01760. E-mail: [email protected] 1526-5900/$36.00 ª 2015 by the American Pain Society http://dx.doi.org/10.1016/j.jpain.2014.08.005 116 mean value for the primary endpoint. The group mean difference is often difficult to interpret in a clinically intuitive manner. Thus, to allow easier interpretation of clinical data, the NNT defines each patient as either a responder or a nonresponder (based on some predefined definition of response) and compares the proportion of responders in each group. Definition and Methods of Calculation of the NNT The NNT is interpreted as the number of patients one would need to treat in order to get one more responder on the active treatment than one would have gotten had they been treated with control. In technical terms, the NNT is the inverse of the absolute risk difference (ARD): 1 NNT ¼ ARD : ARD is the difference in proportion of patients who manifest a response to a treatment and the proportion of patients who manifest a response to control. It is possible to use placebo, nontreatment, or another active Katz, Paillard, and Van Inwegen treatment as the control to calculate the NNT. The choice of controls has a huge impact on the NNT values and their interpretations. Thus, any comparison of NNT values must use the same controls for calculations; comparing NNT values calculated with different control groups would not be valid. Therefore, the discussions in this review are limited to comparisons to placebo controls, unless otherwise so stated. Most often, the response used to calculate the ARD is an improvement (eg, reduction in pain), in which case ARD is calculated as ‘‘response with drug minus response with placebo.’’ Responders, patients who manifest a response, are defined as patients who meet a predefined criterion of response in an all-or-nothing fashion (ie, death/life). However, for most uses, a nondichotomous endpoint is used (eg, pain intensity score), and a predefined response criterion is created (eg, having a $30% pain reduction or not). The following is an example of calculating the NNT. If half (50%) the patients on active treatment respond (response rate = .5), and one quarter (25%) of the placebo-treated patients respond (response rate = .25), then the ARD is .5.25 = .25. The NNT is 1/.25 = 4. This can be interpreted as 4 patients would have to be treated with the treatment to get 1 more responder than with placebo. In other words, treating 4 patients with treatment would yield 2 responders, whereas treating 4 patients with placebo would yield only 1 responder. The NNT can be also calculated using the odds ratio (OR) or the relative risk reduction (RRR) (reviewed in33). The optimal NNT value is 1, whereby every patient has a positive response to treatment and no patient responds to placebo. When a drug produces an identical effect to placebo, the NNT would have a value of infinity (ARD = 0 and NNT = 1/0). Thus, in theory, the NNT can vary from 1 to infinity. It is also possible for the NNT to have a negative value when the response rate for placebo is greater than that for the drug. In practice, the NNT is usually used to compare effective drugs, so negative and infinity values are not usually reported because the drug is considered ineffective. Thus, the lower (ie, the closer to 1) the NNT, the more efficacious the drug. Uses of the NNT The NNT is usually used to compare the efficacy of different drugs for the same indication to enable physicians to make informed choices in clinical practice. To allow comparison and ranking of the efficacy of different treatments, many systematic reviews and meta-analyses of randomized controlled trials provide average NNT values for various treatments across an indication (the NNT being treatment- and dose-specific).33 For instance, a meta-analysis evaluating the efficacy of analgesics ranked the drugs’ efficacy by NNT value (the lower the NNT, the higher the efficacy) as follows: efficacy of ibuprofen 400 mg (NNT = 2.8) > paracetamol (600/ 650 mg) (NNT = 5.0) > codeine 60 mg (NNT = 18).34 The NNT has become widely utilized for comparing treatment efficacy for chronic pain and other conditions, which informs decisions for market access, reimbursement, and position in treatment guidelines, which affect The Journal of Pain 117 the lives of countless patients. Reliance on the NNT for this purpose is based on presumptions of methodologic robustness and straightforward interpretability. Herein, we conducted a qualitative review of the advantages and limitations of the NNT to assess whether the NNT is suitable for evaluating the comparative efficacy of analgesics for chronic pain. Critiques of the NNT Critiques of NNT have been grouped into 6 major categories (Table 1). A number of these critiques (both positive and negative) were not specifically inherent to the NNT, but could be applied to any comparative measure of efficacy such as the ARD and OR. The fact that the NNT can be impacted by study design (eg, study size, number of arms, type of comparator) and subject’s characteristics (eg, indication, severity, and duration of disease; reviewed in references14,31,32,48,51) is not too surprising as these factors influence the response rate, which forms the basis of the NNT definition. These variables can also influence other comparative measures. Thus, critiques of the NNT were categorized based on whether they are specific to the NNT or nonspecifically applicable to any placebo-adjusted efficacy measure used in meta-analysis. Critiques Specific to the NNT Issues Associated With Calculating the NNT Calculating the Combined NNT From Various Trials Can Be Subject to Bias. Two methods have been proposed and used to calculate the NNT from several clinical trials. One method uses a meta-analytic method wherein each trial is handled separately, and the other treats the data as if arising from a single trial.2,6 The latter method is prone to bias, especially when there is an imbalance in sample size between treatment and placebo arms, a phenomenon called the Simpson’s paradox. The metaanalytic method is not prone to this issue. In metaanalyses, the use of a relative measure such as OR or risk ratio (RR) is advocated because event rates vary considerably from study to study even for the same drug.6 The method used to calculate the combined NNT from various trials should be clearly stated. The NNT Can Have an Infinite Value. Unlike other measures of efficacy (eg, ARD), the NNT is an inversion of a response (ie, 1/ARD) so that a zero difference between active and placebo groups results in an undefined number (ie, 1/0).18,26,43 This could be further complicated if the treatment in one study is less efficacious than placebo, resulting in a negative number. Having an infinite or negative value renders comparing studies and calculating the combined NNT for several trials difficult.2,8,22,30,50 As stated above, using a meta-analytic methodology based on the OR or RR is recommended.6 In some systematic reviews, the NNT is considered ‘‘nonsignificant’’ when it is high or infinite,16 which means that the treatment has no therapeutic value. However, the cutoff value for ‘‘high’’ is arbitrary; the 118 Uses and Misuses of NNT to Rank Analgesics The Journal of Pain Table 1. Critiques of the NNT TYPES OF CRITIQUES STUDIES Critiques specific to the NNT Issues associated with calculating the NNT: The NNT can have an infinite value, creating problems for meta-analyses and causing a disproportionate impact of failed versus successful studies The precision of the NNT is difficult to estimate The NNT has a skewed CI The NNT is difficult to interpret Critiques of the NNT applicable to other endpoints used in meta-analyses The NNT is sensitive to the level of efficacy in the placebo group The NNT depends on the endpoint: The NNT is dependent on the selection of outcome measured The NNT is dependent on the cutoff chosen for the dichotomous outcome The NNT is dependent on the time point of outcome The NNT depends on factors internal and external to the study aside from study drug NNT does not reflect effectiveness of treatment in clinical practice Suissa,49 Stang,48 Hutton,22 Hutton,23 Thabane,50 Ebrahim,13 Hutton,24 Lesaffre,30 Newcombe,37 Newcombe,38 Smeeth,47 Altman1,2 Christensen,8 Ebrahim,13 Smeeth47 Moore 33 Suissa,49 Stang,48 Citrome,9 McAlister,32 Moore,35 Christensen,8 Mayne,31 Tramer,51 Wu,53 Ebrahim13 Suissa,49 Stang,48 Citrome,9 McAlister,32 Moore,35 Christensen,8 Mayne,31 Tramer,51 Wu,54 Ebrahim13 Tramer,51 Smeeth,47 Black,4 Dowie10 therapeutic value or lack thereof of a therapy with a high NNT would be dependent on the therapeutic area and availability of successful treatments with lower NNT values. In an indication with limited treatments (eg, visceral pain), a ‘‘high’’ number would be more acceptable than in a pain indication with multiple options. The Precision of the NNT Is Difficult to Estimate. A measure of drug effect size should have a definable precision, such as a 95% confidence interval (CI). When the NNT is very high or infinite, its 95% CI cannot be accurately calculated.1,2,8,22,30,50 For instance, if the ARD is .01 and its 95% CI is [.01 to 1.03], the NNT is 100 (1/.01) but its 95% CI is not [100 to 133.3]. In this example, the 95% CI would be mathematically 2 intervals, one at [N, 100] and another at [133.3, 1N], because the ARD 95% CI contains zero, which is very difficult to interpret.8 Therefore, in such circumstances, it has been recommended that the NNT be given only as a point estimate (ie, 100 in this example) without the 95% CI, which avoids the mathematical problem but does not fulfil the desire for an estimate of precision. The NNT Has a Skewed CI. The NNT is calculated by inverting the ARD and its CI by inverting the ARD’s CI limits. This leads to an uneven distribution of the NNT’s CI, whereby the upper bound of the CI is artificially ‘‘inflated.’’2,50 For instance, if the ARD is .1 times the 95% CI: [.05–.15], the NNT is 10 times the 95% CI: [6.7–20]. Therefore, the NNT value is further from the upper bound of the CI than from the lower bound of the CI.2 To provide a real example, the NNT for 60 mg etoricoxib to produce at least 50% pain relief at 6 weeks compared with placebo was 2.6 [95% CI: 2.0–3.9], showing an ‘‘inflation’’ of the upper bound of the 95% CI.35 However, this anomaly is not unique to the NNT and has been observed with the OR, albeit for different reasons. mean differences, RRR, OR, and absolute risk reduction (ARR).33 However, several studies using a randomized design to survey the understanding of NNT among doctors,21,39 medical students,43 patients,44 and laypersons20,28 have shown that they have difficulty understanding the meaning of the NNT. One survey of first-year medical students showed that treatment benefit was correctly interpreted by $75% of the students when presented as RRR or ARR, but only by 30% of students when presented as the NNT.43 A survey of Norwegian medical doctors showed that many believed that only 1 of NNT patients would benefit from treatment (eg, if the NNT were 4, then 1 of 4 patients would benefit).21 Patients who were presented with clinical data in terms of RRR, ARR, and NNT were best able to interpret the benefits of treatment when it was presented as RRR or ARR.44 A study showed that a large majority of people would accept using the hypothetical treatment presented to them regardless of its NNT, and that those who declined using the medication misinterpreted the NNT.28 In another study, laypersons presented with the benefit of a hypothetical osteoporosis intervention and offered the therapy were sensitive to the magnitude of treatment benefit when it was presented in terms of postponement of hip fracture, but not in terms of NNT.7,20 A search for definitions of the NNT on the Internet shows that the NNT is commonly misinterpreted as the number of patients one needs to treat to get one responder. The NNT Is Difficult to Interpret The NNT Is Sensitive to the Level of ‘‘Efficacy’’ in the Placebo Group Since its inception in 1988, the NNT has quickly become a widely used measure of a drug’s efficacy because it was thought to be a more intuitive measure of a drug’s efficacy than other measures of efficacy such as group Critiques of the NNT Applicable to Other Endpoints Used in Meta-Analyses An important asset of the NNT is that it takes into account the response observed in the placebo group, thereby allowing for the adjustment for nonspecific Katz, Paillard, and Van Inwegen Impact of the Placebo Response on NNT—Theoretical Example No. 1 Table 3. % RESPONDERS IN ACTIVE TREATMENT GROUP % RESPONDERS IN ACTIVE TREATMENT GROUP Table 2. 10 20 30 40 50 60 70 80 119 The Journal of Pain % RESPONDERS IN PLACEBO GROUP DELTA NNT % MORE RESPONDERS IN ACTIVE GROUP* 0 10 20 30 40 50 60 70 10 10 10 10 10 10 10 10 10.0 10.0 10.0 10.0 10.0 10.0 10.0 10.0 100.0 50.0 33.3 25.0 20.0 16.7 14.3 12.5 *Calculated as (% responders in active group) (% responders in placebo group) / % responders in active group. factors that may be associated with non–treatment-specific benefits in a clinical trial, such as nonspecific response, spontaneous improvements/worsening of the disease, natural history, and regression to the mean. To this end, the NNT is intending to serve as a measure of the pharmacologic benefit of a drug over and above nonspecific factors that may be associated with benefits in a clinical trial. Other placebo-adjusted measures such as group mean differences, ORs, and RRs are also commonly used to ‘‘normalize’’ the incremental pharmacologic benefit of a drug in the context of a clinical trial. As with other comparative measures of efficacy that rely upon the difference between drug and placebo, the absolute level of placebo response can have an impact on interpretation. For example, a treatment with a high absolute benefit, but a nearly as high benefit in the placebo group, will appear highly effective in clinical practice but will have an unfavorable NNT. A treatment with a more modest absolute benefit, but a much lower response in the placebo group, will appear less effective in clinical practice despite a more favorable NNT. This is illustrated in the theoretical example illustrated in Table 2, where the NNT of different treatments remains constant, but the likely clinical interpretation and desirability of treatment does not. Another theoretical example to consider is where the response to drug remains constant but the response to placebo varies, as is often observed between similar studies of the same treatment (see examples below and reference12). In Table 3, the drug’s response was held constant at 40% (a typical response rate observed for analgesics) and the placebo response varied from 5% to 40%. This example shows that the NNT dramatically increases with increasing placebo response, reaching infinity when the response in the placebo group is equal to that in the active group (Table 3). Although the NNT for these theoretical examples varied from 2.9 to infinity, the ARD only varied from .35 to 0, illustrating how the NNT appears to be more unstable than the ARD in the face of variable placebo responses. Impact of the Placebo Response on NNT—Theoretical Example No. 2 40 40 40 40 40 % RESPONDERS IN PLACEBO GROUP DELTA NNT ARD 5 10 20 30 40 35 30 20 10 0 2.9 3.3 5 10 N .35 .30 .20 .10 0 The fact that the NNT varies more widely than the ARD is illustrated in examples of clinical trials noted in Table 4. This table shows trials from anticonvulsant analgesics with very different NNTs (presented in order of lowest to highest NNT) and presents the ARD. In these examples, the NNT varied from 1.4 to infinity, whereas the ARD only varied from .704 to 0. This is again a consequence of the difference between the active and placebo groups in the proportion of patients improving. The NNT Depends on the Endpoint To calculate the NNT, continuous data need to be converted into dichotomous data; for instance, pain scores over time need to be converted into change in pain score from baseline to endpoint, and then converted to a response rate using a predefined criterion; for example, proportion of subjects having an X% pain reduction from baseline to endpoint. Therefore, to calculate the NNT of an active drug in a trial, one needs to select 1) the derived outcome measure (eg, % responders); 2) the cutoff for the definition of response (eg, 30% reduction in pain); and 3) the time at which the observation of response/nonresponse is made (time point). Several articles have shown that the NNT is dependent on the outcome measured,11,28 the time point of measurement,6,11,44,45 and the cutoff value of response.31 The NNT Is Dependent on the Selection of Endpoint Measured. Comparison of the NNT for total mortality, mortality, and all cardiovascular events in various statin trials showed that the NNT value was different for each of these outcome measures.11 In an analgesic trial, it seems obvious that the NNT for reduction in pain will not be the same as the NNT for improvement in sleep. Moore’s review36 of pregabalin efficacy presented the NNT for 2 outcomes: the proportion of subjects with $30% or $50% pain reduction (% responders) and the level of improvement in Patient’s Global Impression of Change (Fig 1). The NNT for the level of improvement in Patient’s Global Impression of Change was systematically higher than the NNT for the proportion of responders (regardless of the cutoff), although all 3 sets of NNT values yield the same conclusion.36 The NNT Is Dependent on the Cutoff Chosen for the Dichotomous Outcome. Transformation of continuous data into dichotomous data, a process necessary to calculate the NNT, reduces the statistical estimation of outcomes and results in an important loss of information. 120 Uses and Misuses of NNT to Rank Analgesics The Journal of Pain NNT Varies More Widely Than ARD—Examples of Clinical Trials of Anticonvulsants in Neuropathic Pain Table 4. REFERENCE ANALGESIC DRUG NO. (%) OF PATIENTS WHO IMPROVED* WITH ACTIVE TREATMENT NO. (%) OF PATIENTS WHO IMPROVED* WITH PLACEBO NNT ARD Killian27 Zakrzewska55 Gilron19 Simpson45 Simpson46 Otto40 Raskin41 Drewes11 Serpell42 Finnerup17 Carbamazepine Lamotrigine Gabapentin Gabapentin Lamotrigine Valproate Topiramate Valproate Gabapentin Lamotrigine 19/27 (70.4) 7/13 (53.8) 27/44 (61.4) 15/30 (50.0) 86/150 (57.3) 8/31 (25.8) 74/214 (34.6) 6/20 (30.0) 32/153 (20.9) 4/21 (19.0) 0/27 (0.0) 1/14 (7.1) 13/42 (31.0) 7/30 (23.3) 30/77 (39.0) 3/31 (9.7) 23/109 (21.1) 4/20 (20.0) 21/152 (13.8) 4/21 (19.0) 1.4 2.1 3.3 3.8 5.4 6.2 7.4 10.0 14.1 N .704 .467 .304 .267 .183 .161 .135 .10 .072 .0 NOTE. Data are from Finnerup et al.16 *Response was based on 50% pain relief; if 50% pain relief could not be obtained directly from the publication, then the number of patients reporting at least good pain relief or reporting improvement was used to calculate the NNT. Thus, if the NNT was to become the measure of choice in clinical trials, study design may evolve toward the use of dichotomous measures (such as response rate) as primary endpoints, which would reduce studies’ power (or lead to increased sample size).15 Dichotomizing the data requires that the analyst decide on a cutoff, which can be somewhat arbitrary; not all studies use the same definition for the cutoff point to determine the number of responders (most studies use the 30% threshold, but others use a 20% or 50% threshold). Dichotomization separates patients into responders and nonresponders, losing the nuances of partial responders (those close to the threshold). For instance, a subject with a 31% response will have a preferential impact over one that has a 29% response. The example illustrated in Table 5 shows that the NNT is dependent on the cutoff of the outcome: the NNT for the 30% pain reduction cutoff is systematically lower than that for the 50% cutoff. In another example, the NNT seems to increase with increasing cutoffs of percentages of response, especially for the lower doses (Table 5)35; indeed, for the 5-mg dose, the NNT jumps from 4.0 to 5.3 to 12.5 (quadruples), and for the 10-mg dose it jumps from 3.7 to 5.9 to 7.1 (doubles) for the typical cutoffs of 20%, 30%, and 50% of pain relief, respectively (Table 5). Thus, as with any comparative measure, the selection of the cutoff chosen is critical and the same exact cutoff needs to be used for comparing data from different studies. The NNT Is Dependent on the Time Point of Outcome. The NNT depends on when the outcome is measured. First, it is expected that the response to treatment will vary over time: the response rate may be very different at 1 week and at 4 weeks of treatment, and so will the NNT calculated at these 2 time points. This issue renders difficult the comparison of NNT from different studies with various lengths, which is typical in chronic indications.31 The 3 issues mentioned above are not unique to the NNT, and any comparative measure of efficacy is likely to be affected by the type of outcome considered, the time point of the outcome, and the cutoff chosen. However, what is unique to the NNT is the mechanism by which one has to dichotomize the selected endpoint. Some endpoints do not lend themselves easily to simple dichotomization into responder or nonresponder. The NNT Depends on Internal and External Factors Aside From Study Drug Like all other measures of efficacy in clinical trials, the NNT is affected by factors internal to the study (study design and conduct) and factors external to the study (real-world factors). NNT Varies With the Cutoff for the Dichotomous Variable (% Pain Relief) Table 5. ETORICOXIB DOSE (MG) 5 10 30 60 Figure 1. NNT for pregabalin calculated from various outcome measures (data from Moore et al36). NNT FOR 20% PAIN RELIEF NNT FOR 30% PAIN RELIEF NNT FOR 50% PAIN RELIEF 4.0 3.7 3.6 2.3 5.3 5.9 4.0 2.4 12.5 7.1 4.3 2.6 NOTE. Data are from Moore et al.35 Katz, Paillard, and Van Inwegen The Journal of Pain 121 Figure 2. NNT for analgesics by year of publication (data from Finnerup et al16). Left panel: tricyclic antidepressants; right panel: anticonvulsants. Each point of data represents 1 clinical trial. The NNT Depends on Factors Internal to the Study. A few articles have reviewed the study factors that can impact the NNT12,14,25,26,31,32,48,51 and we refer the reader to these articles for further explanations. Briefly, these factors include 1. The study population, as the type of pain indication and severity of condition at baseline influence the response to active treatment12 2. The study design, for example, number of sites12 3. The comparator: controls used as comparators have huge impact on numbers generated and interpretations; possible controls include a true placebo, an active placebo, no treatment, or another active treatment3,53 4. The time period (as discussed in the previous section) 5. The type of outcome (as discussed in the previous section) The heterogeneity of trials’ data makes pooling NNT data across studies clinically irrelevant.14 Thus, if the NNT is to be used to compare treatments, the therapies must have been tested in similar populations with the same condition at the same stage, using the same comparator, time period, and outcomes.28 Therefore, comparisons of analgesics using the NNT that fail to follow these guidelines may not be valid. Approaches to calculation of the NNT that adjust for such confounders have been described; using an NNT model to account for differences in study design and conduct allows for more meaningful comparisons.5 The NNT Depends on Factors External to the Study. External factors have been cited as potential influencers of observed net treatment effects. The year of publication is one such factor that may stand as a proxy for multiple other influences (eg, availability of other treatments, approval status of the treatment, expectation of treatment benefit, and shifts in sources of patients). A valid measure of treatment effects should be robust to factors other than the treatment itself. The NNT for antidepressant analgesics as well as for anticonvulsant analgesics has steadily increased (the efficacy had gotten worse) over time (Fig 2; reference18). This could be attributed to the fact that in antidepressant trials, placebo response increased more over time (year of publication) than the response to active treatment.52 Increasing placebo response over time relative to the drug will distort any measure of efficacy, including the group mean differences. However, this phenomenon results in more distortion of the NNT over time compared to alternative measures of efficacy (as discussed earlier). Another, perhaps more obvious, reason for the increase in NNT over time is that the experimental conditions (study design and patient population) have evolved over time, rendering the comparison of older and recent studies inappropriate. Indeed, more recent trials, for reasons that are not entirely clear, have greatly increased placebo responses compared to older trials.10 Use of the NNT in Clinical Practice The NNT has been used as a yardstick to compare the efficacy of various drugs, to help clinicians choose between active treatments, inform treatment guidelines, determine market access and reimbursement, and support risk-benefit analyses. But as placebo is not given in clinical practice, placeboadjusted metrics like the NNT have limited usefulness in clinical practice and can be irrelevant to real-world efficacy3 and misleading.43 For example, in the clinic, a physician facing the choice between 1) Treatment A with an NNT of 10 that produces a response in 80% of patients (but a response in 70% of placebo patients) or 2) Treatment B with an NNT of 2.9 that yields a response in 40% of active-treated patients (but 5% in the placebo group) would likely choose Treatment A because it shows greater efficacy in a large proportion of patients—which is what the clinician is looking for—even though it has a higher NNT. Thus, if one wants to measure efficacy in a clinical trial (as defined by the incremental benefit of the drug’s pharmacology over the nonspecific effects of being in the trial), one needs a placebo-adjusted robust measure like the NNT. However, to measure efficacy in the real world, the absolute response rate and similar unadjusted measures may provide a more relevant perspective. Moreover, the NNT taken alone does not summarize all necessary information for the clinician to make informed decisions regarding treatment.10,51 Indeed, a physician not only considers the efficacy of the drug but also takes into account the rate and seriousness of adverse effects of each treatment, the patient’s preference, cost, and clinical experience (if any) with the treatments. Efforts are underway to create quantitative metrics that integrate these factors. Thus, decisions for use in the real world need to be based on multiple pieces of information, not just a solitary measure of efficacy compared to placebo. 122 The Journal of Pain Conclusions Standardized measures of efficacy are needed to compare analgesic efficacy across trials. The NNT was developed to be a statistically robust and readily interpretable measure to rank the efficacy of treatments, including analgesics. However, the NNT is associated with specific weaknesses in calculation and interpretation that are not associated with other methods for integrating data from multiple trials. These weaknesses include distortions in its calculation as placebo effects approach treatment effects, with the possibility of infinite values; difficulties in estimating the precision of the NNT particularly for CI calculation; and, contrary to the original intent, difficulties in interpretation. The NNT requires manipulation of the original variable by References 1. Altman DG: Confidence intervals for the number needed to treat. Br Med J 317:1309-1312, 1998 2. Altman DG, Deeks JJ: Meta-analysis, Simpson’s paradox, and the number needed to treat. BMC Med Res Methodol 2:3, 2002 3. Backonja M, Wallace MS, Blonsky ER, Cutler BJ, Malan P Jr, Rauck R, Tobias J: NGX-4010 C116 Study Group: NGX-4010, a high-concentration capsaicin patch, for the treatment of postherpetic neuralgia: a randomised, double-blind study. Lancet Neurol 7:1106-1112, 2008 Uses and Misuses of NNT to Rank Analgesics selecting cutoff points for dichotomization, with the NNT often changing depending on the cutoff. The NNT suffers from problems common to other placeboadjusted endpoints, including being sensitive to studyrelated and external factors (eg, year of publication) that, when not considered, undermine the validity of the NNT as a tool for comparing different treatments in different studies. Approaches to improving the validity of the NNT (and other summary measures) by adjusting for such factors deserve further exploration. Finally, efficacy alone, as measured by any measure, is only one part of the profile of a treatment to be considered in determining its place in therapy. Therefore, clinicians and other stakeholders need to be aware of these issues to correctly calculate, use, and interpret the NNT. Hertz S, Jay GW, Junor R, Kerns RD, Kerwin R, Kopecky EA, Lissin D, Malamut R, Markman JD, McDermott MP, Munera C, Porter L, Rauschkolb C, Rice AS, Sampaio C, Skljarevski V, Sommerville K, Stacey BR, Steigerwald I, Tobias J, Trentacosti AM, Wasan AD, Wells GA, Williams J, Witter J, Ziegler D: Considerations for improving assay sensitivity in chronic pain clinical trials: IMMPACT recommendations. Pain 153:1148-1158, 2012 13. Ebrahim S: The use of numbers needed to treat derived from systematic reviews and meta-analysis. Caveats and pitfalls. Eval Health Prof 24:152-164, 2001 14. Edelsberg J, Oster G: Summary measures of number needed to treat: How much clinical guidance do they provide in neuropathic pain? Eur J Pain 13:11-16, 2009 4. Black HR, Crocitto MT: Number needed to treat: Solid science or a path to pernicious rationing? Am J Hypertens 11:128S-134S, 1998. discussion 135S-137S 15. Fedorov V, Mannino F, Zhang R: Consequences of dichotomization. Pharm Stat 8:50-61, 2009 5. Caro JJ, Ishak KJ, Caro I, Migliaccio-Walle K, Klittich WS: Comparing medications in a therapeutic area using an NNT model. Value Health 7:585-594, 2004 16. Finnerup NB, Otto M, McQuay HJ, Jensen TS, Sindrup SH: Algorithm for neuropathic pain treatment: An evidence based proposal. Pain 118:289-305, 2005 6. Cates CJ: Simpson’s paradox and calculation of number needed to treat from meta-analysis. BMC Med Res Methodol 2:1, 2002 17. Finnerup NB, Sindrup SH, Bach FW, Johannesen IL, Jensen TS: Lamotrigine in spinal cord injury pain: A randomized controlled trial. Pain 96:375-383, 2002 7. Christensen PM, Brøsen K, Brixen K, Andersen M, Kristiansen IS: A randomized trial of laypersons’ perception of benefit of osteoporosis therapy: Number needed to treat versus postponement of hip fracture. Clin Ther 25: 2575-2585, 2003 18. Finnerup NB, Sindrup SH, Jensen TS: The evidence for pharmacological treatment of neuropathic pain. Pain 150: 573-581, 2010 8. Christensen PM, Kristiansen IS: Number-needed-to-treat (NNT)—Needs treatment with care. Basic Clin Pharmacol Toxicol 99:12-16, 2006 9. Citrome L: Compelling or irrelevant? Using number needed to treat can help decide. Acta Psychiatr Scand 117: 412-419, 2008 10. Dowie J: The ‘‘number needed to treat’’ and the ‘‘adjusted NNT’’ in health care decision-making. J Health Serv Res Policy 3:44-49, 1998 11. Drewes AM, Andreasen A, Poulsen LH: Valproate for treatment of chronic central pain after spinal cord injury. A double-blind cross-over study. Paraplegia 32:565-569, 1994 12. Dworkin RH, Turk DC, Peirce-Sandner S, Burke LB, Farrar JT, Gilron I, Jensen MP, Katz NP, Raja SN, Rappaport BA, Rowbotham MC, Backonja MM, Baron R, Bellamy N, Bhagwagar Z, Costello A, Cowan P, Fang WC, 19. Gilron I, Bailey JM, Tu D, Holden RR, Weaver DF, Houlden RL: Morphine, gabapentin, or their combination for neuropathic pain. N Engl J Med 352:1324-1334, 2005 20. Halvorsen PA, Kristiansen IS: Decisions on drug therapies by numbers needed to treat: A randomized trial. Arch Intern Med 165:1140-1146, 2005 21. Halvorsen PA, Kristiansen IS, Aasland OG, Førde OH: Medical doctors’ perception of the ‘‘number needed to treat’’ (NNT). Scand J Prim Health Care 21:162-166, 2003 22. Hutton JL: Misleading statistics: The problems surrounding number needed to treat and number needed to harm. Pharm Med 24:145-149, 2010 23. Hutton JL: Number needed to treat and number needed to harm are not the best way to report and assess the results of randomised clinical trials. Br J Haematol 146:27-30, 2009 24. Hutton JL: Number needed to treat: Properties and problems. J R Statist Soc A 163:403-419, 2000 Katz, Paillard, and Van Inwegen 25. Katz N: Methodological issues in clinical trials of opioids for chronic pain. Neurology 65:S32-49, 2005 26. Katz J, Finnerup NB, Dworkin RH: Clinical trial outcome in neuropathic pain: Relationship to study characteristics. Neurology 70:263-272, 2008 27. Killian JM, Fromm GH: Carbamazepine in the treatment of neuralgia. Use of side effects. Arch Neurol 19:129-136, 1968 28. Kristiansen IS, Gyrd-Hansen D, Nexø J, Nielsen JB: Number needed to treat: Easily understood and intuitively meaningful? Theoretical considerations and a randomised trial. J Clin Epidemiol 55:888-892, 2002 29. Laupacis A, Sackett DL, Roberts RS: An assessment of clinically useful measures of the consequences of treatment. N Engl J Med 318:1728-1733, 1988 30. Lesaffre E, Pledger G: A note on the number needed to treat. Control Clin Trials 20:439-447, 1999 31. Mayne TJ, Whalen E, Vu A: Annualized was found better than absolute risk reduction in the calculation of number needed to treat in chronic conditions. J Clin Epidemiol 59: 217-223, 2006 32. McAlister FA: The ‘‘number needed to treat’’ turns 20— and continues to be used and misused. CMAJ 179:549-553, 2008 33. Moore RA: What Is an NNT? In ‘‘What Is. Series.’’ April 2009. Available at: http://www.whatisseries.co.uk/whatis/ pdfs/What_is_an_NNT.pdf The Journal of Pain 123 41. Raskin P, Donofrio PD, Rosenthal NR, Hewitt DJ, Jordan DM, Xiang J, Vinik AI: Topiramate vs placebo in painful diabetic neuropathy: Analgesic and metabolic effects. Neurology 63:865-873, 2004 42. Serpell MG: Gabapentin in neuropathic pain syndromes: A randomised, double-blind, placebo-controlled trial. Pain 99:557-566, 2002 43. Sheridan SL, Pignone MP: Numeracy and the medical student’s ability to interpret data. Eff Clin Pract 5:35-40, 2002 44. Sheridan SL, Pignone MP, Lewis CL: A randomized comparison of patient’s understanding of number needed to treat and other risk reduction formats. J Gen Intern Med 18:884-892, 2003 45. Simpson DA: Gabapentin and venlafaxine for the treatment of painful diabetic neuropathy. J Clin Neuromuscul Dis 3:53-62, 2001 46. Simpson DM, McArthur JC, Olney R, Clifford D, So Y, Ross D, Baird BJ, Barrett P, Hammer AE: Lamotrigine for HIV-associated painful sensory neuropathies: A placebocontrolled trial. Neurology 60:1508-1514, 2003 47. Smeeth L, Haines A, Ebrahim S: Numbers needed to treat derived from meta-analyses sometimes informative, usually misleading. BMJ 318:1548-1551, 1999 48. Stang A, Poole C, Bender R: Common problems related to the use of number needed to treat. J Clin Epidemiol 63: 820-825, 2010 34. Moore RA: Pain and systematic reviews. Acta Anaesthesiol Scand 45:1136-1139, 2001 49. Suissa D, Brassard P, Smiechowski B, Suissa S: Number needed to treat is incorrect without proper time-related considerations. J Clin Epidemiol 65:42-46, 2012 35. Moore RA, Moore OA, Derry S, McQuay HJ: Numbers needed to treat calculated from responder rates give a better indication of efficacy in osteoarthritis trials than mean pain scores. Arthritis Res Ther 10:R39, 2008 50. Thabane L: A closer look at the distribution of number needed to treat (NNT): a Bayesian approach. Biostatistics 4: 365-370, 2003 36. Moore RA, Straube S, Wiffen PJ, Derry S, McQuay HJ: Pregabalin for acute and chronic pain in adults. Cochrane Database Syst Rev 3:CD007076, 2009 37. Newcombe RG: Know your limitations: Not just for clinicians: Estimation of confidence intervals is not straightforward. J Public Health Med 21:481-482, 1999 38. Newcombe RG: Confidence intervals for the number needed to treat. Absolute risk reduction is less likely to be misunderstood. BMJ 318:1765-1767, 1999 39. Nexø J, Gyrd-Hansen D, Kragstrup J, Kristiansen IS, Nielsen JB: Danish GPs’ perception of disease risk and benefit of prevention. Fam Pract 19:3-6, 2002 40. Otto M, Bach FW, Jensen TS, Sindrup SH: Valproic acid has no effect on pain in polyneuropathy: A randomized controlled trial. Neurology 62:285-288, 2004 r MR, Walder B: Number needed to treat (or 51. Trame harm). World J Surg 29:576-581, 2005 52. Walsh BT, Seidman SN, Sysko R, Gould M: Placebo response in studies of major depression: Variable, substantial, and growing. JAMA 287:1840-1847, 2002 53. Webster LR, Malan TP, Tuchman MM, Mollen MD, Tobias JK, Vanhove GF: A multicenter, randomized, double-blind, controlled dose finding study of NGX-4010, a high-concentration capsaicin patch, for the treatment of postherpetic neuralgia. J Pain 11:972-982, 2010 54. Wu LA, Kottke TE: Number needed to treat: Caveat emptor. J Clin Epidemiol 54:111-116, 2001 55. Zakrzewska JM, Chaudhry Z, Nurmikko TJ, Patton DW, Mullens EL: Lamotrigine (Lamictal) in refractory trigeminal neuralgia: Results from a double-blind placebo controlled crossover trial. Pain 73:223-230, 1997