Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
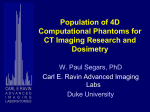
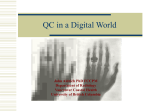
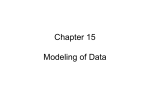
ORIGINAL ARTICLE Perfusion Assessment Using Intravoxel Incoherent Motion-Based Analysis of Diffusion-Weighted Magnetic Resonance Imaging Validation Through Phantom Experiments Ju Hee Lee, MD,* Hyunhee Cheong, BA,† Seung Soo Lee, MD, PhD,† Chang Kyung Lee, PhD,† Yu Sub Sung, PhD,† Jae-Wan Huh, PhD,‡ Jung-A Song, MD, PhD,§ and Han Choe, MD, PhD§ Objectives: The aims of this study were to demonstrate the theoretical meaning of intravoxel incoherent motion (IVIM) parameters and to compare the robustness of 2 biexponential fitting methods through magnetic resonance experiments using IVIM phantoms. Materials and Methods: Intravoxel incoherent motion imaging was performed on a 3 T magnetic resonance imaging scanner using 15 b values (0–800 s/mm2) for 4 phantoms with different area fractions of the flowing water compartment (FWC%), at the infusion flow rates of 0, 1, 2, and 3 mL/min. Images were quantitatively analyzed using monoexponential free biexponential, and segmented biexponential fitting models. Results: There were some inconsistent variations in Dslow with changing flow rates. The perfusion fraction, f, showed a significant positive correlation with the flow rate for both the free and segmented fitting methods (ρ = 0.838 to 0.969; P < 0.001). The fast diffusion coefficient, Dfast, had a significant positive correlation with the flow rate for segmented fitting (ρ = 0.745 to 0.969; P < 0.001), although it showed an inverse correlation with the flow rate for free fitting (ρ = −0.527 to −0.791; P ≤ 0.017). Significant positive correlations with the FWC% of the phantoms were noted for f (P = 0.510 for free fitting and P = 0.545 for segmented fitting, P < 0.001). Conclusions: The IVIM model allows for an approximate segmentation of molecular diffusion and perfusion, with a minor contribution of the perfusion effect on Dslow. The f and Dfast can provide a rough estimation of the flow fraction and flow velocity. Segmented fitting may be a more robust method than free fitting for calculating the IVIM parameters, especially for Dfast. Key Words: intravoxel incoherent motion, perfusion, diffusion-weighted imaging, phantom experiment, fitting algorithm According to the IVIM theory, each IVIM parameter has a specific biologic meaning; in biologic tissue, the slow diffusion coefficient (Dslow) stands for the degree of brownian motion of water molecule or pure molecular diffusion, perfusion fraction (f) for the fraction of water flowing in capillaries, and fast diffusion coefficient (Dfast) for flow velocity.1,2 Although a few phantom and animal experiments suggested the flow dependency of f and Dfast,17–20 these studies did not separately evaluate the effect of the flowing water fraction and flow velocity on the IVIM parameters and thus provided only limited proof regarding the biologic meaning of IVIM parameters. The IVIM-based analysis of DW imaging data has been usually performed using either free, unconstrained, nonlinear, least square fitting (hereafter referred to as free fitting), or segmented, partially constrained fitting (hereafter referred to as segmented fitting).12,21–24 Although previous computer simulation studies claimed the superiority of segmented fitting to that of free fitting in terms of its accuracy and reliability, this result has not been completely proven with actual DW imaging data. For successful clinical application of IVIM imaging, it is crucial to analyze image data using the robust postprocessing method as well as to adequately interpret the results with a correct understanding of the meaning of each IVIM parameter. To this end, we conducted IVIM imaging experiments using the phantoms that consist of static and flowing water compartments, in simulated conditions with various flowing water fractions and flow velocities. The purpose of our phantom experiments was to prove the theoretical meaning of IVIM parameters and to compare the robustness of the free and segmented fitting methods. (Invest Radiol 2016;00: 00–00) I ntravoxel incoherent motion (IVIM) imaging is a method based on diffusion-weighted (DW) imaging with multiple b values. It allows for the separate analysis of 2 components of random water motion in biologic tissue, that is, pure molecular diffusion and perfusion.1–4 The clinical usefulness of IVIM imaging has been widely investigated in the assessment of various disease processes in many anatomical organs.5–16 Received for publication November 25, 2015; and accepted for publication, after revision, January 6, 2016. From the *Department of Radiology, Center for Liver Cancer, National Cancer Center, Goyang; †Department of Radiology and Research Institute of Radiology, Asan Medical Center, Departments of ‡Biochemistry and Molecular Biology, and §Physiology and Biomedical Institute of Technology, University of Ulsan College of Medicine, Seoul, South Korea. Conflicts of interest and sources of funding: Supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT, and future planning (2014R1A2A1A11052085). The authors report no conflicts of interest. Supplemental digital contents are available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's Web site (www.investigativeradiology.com). Correspondence to: Seung Soo Lee, MD, PhD, Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Asanbyeongwon-gil 86, Songpa-Gu, Seoul 138-736, South Korea. E-mail: [email protected]. Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. ISSN: 0020-9996/16/0000–0000 DOI: 10.1097/RLI.0000000000000262 MATERIALS AND METHODS Principles of IVIM Phantoms Based on the IVIM theory that explains the random motion of water in biologic tissue as 2 components, that is, a slower diffusion component and a faster perfusion component, we devised 2 compartment IVIM phantoms that simplistically reflect human tissue composed of diffusion-dominant intracellular and interstitial space and perfusiondominant microvasculature (Fig. 1). The phantoms were produced using vertical glass columns packed with cross-linked dextran gel beads and water. When water is infused into the phantoms, water flows through the spaces between the beads, which serve as the flowing water compartment of the phantom, thus simulating perfusion-dominant microvasculature in biologic tissue. The gel beads contain many pores on their surface, thus allowing water to diffuse in and out of the gel beads similarly to the transcapillary fluid exchange in biologic tissue. Despite this fluid exchange through the pores, the water within the gel beads is relatively static and, therefore, the space within the gel beads serves as a static water compartment, and thus simulating the diffusion-dominant intracellular and interstitial space. To perform magnetic resonance (MR) experiments in simulated conditions with various flowing water fractions and flow velocities, we produced 4 phantoms with different area fraction of flowing water compartments by using the gel beads with different particle size profiles, after which we Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 Lee et al FIGURE 1. Principle of the IVIM phantom. A, A schematic model of biologic tissue modified from that of Le Bihan at al.1 In terms of the random motion of water molecules, biologic tissue can be divided into 2 compartments, that is, diffusion-dominant intracellular and interstitial space and perfusion-dominant microvasculature. In intracellular and interstitial space, molecular diffusion of water within the intracellular space (a) and the interstitial space (b) accounts for the movement of water, whereas blood flow or perfusion within a capillary (f) predominates in microvasculature. The IVIM theory assumes that water exchange through capillary fenestrations (t) is negligible. B, A schematic drawing of the IVIM phantom. The spaces within the gel beads (c) serve as a static water compartment, and thus simulating diffusion-dominant intracellular and interstitial space. After water infusion into the phantom, the spaces between the gel beads (f ) serve as a flowing water compartment, and thus simulating perfusion-dominant microvasculature. Water can move through the pores on the surface of the gel beads (t), similar to that of transcapillary fluid exchange in biologic tissue. performed MR imaging of the phantoms at different infusion flow rate settings. Preparation of IVIM Phantoms for MR Imaging We produced 4 sets of IVIM phantoms using the gel beads (Sephadex G-25; GE Healthcare, Piscataway, NJ) with different particle size profiles, that is, coarse (wet particle diameter, 100–300 μm), medium (wet particle diameter, 50-150 μm), fine (wet particle diameter, 20–80 μm), and superfine (wet particle diameter, 20–50 μm),25 and chromatography columns (XK16/20; GE Healthcare, Piscataway, NJ) with an internal diameter of 1.6 cm. Despite their differences in particle size, all 4 types of gel beads have the same pore size, that is exclusion limit of 5 kd corresponding to the diameter of approximately 1.1 nm for globular protein,26 as this approximates the size of capillary fenestrations in the brain and is smaller than that in skeletal muscle (5 nm) and renal glomerulus (15 nm).27 The gel beads were prepared and were then packed in the chromatography columns according to the manufacturer's instructions.24 The phantoms were then equilibrated with normal saline doped with 0.8 mM/L gadoterate meglumine (Dotarem; Guerbet, Aulnay-Sous-Bois, France) to adjust the T2 relaxation time of the solution to that of the blood at 3.0 T, that is, approximately 190 milliseconds.28 MR Imaging of the Phantoms Magnetic resonance imaging was performed on a 3 T MR imaging scanner (Magnetom Skyra; Siemens, Erlangen, Germany) and using a 16-channel ankle coil. The maximum gradient specifications were 45 mT/min for the amplitude and 200 T/m per seconds for the slew rate. For MR experiments, we constructed a polyoxymethylene fixation device that holds 2 sets of the phantoms stably fitted to the ankle coil system used in our MR experiments. The flow inlet of the phantom was connected to a peristaltic pump (Minipuls 3; GILSON, Villiers, France) using a flow line (Tygon; Saint-Gobain, Akron, OH), for controlled flow infusion through the phantoms. The flow outlet of each phantom was connected to a glass measuring beaker to measure the amount of actual flow through the phantoms (Fig. 2). To maintain constant temperature of the phantom through the MR experiments, the thermostatic jacket of XK tubes were filled with 20°C water before imaging. The phantoms were wrapped with a 0.5-mm-thick tissue equivalent material (ROM Transparent Bolus; Radiation Oncology Material, Seoul, South Korea) to reduce the susceptibility artifacts from air. After completing preparation of the phantoms for MR imaging, structural imaging was performed for guidance of DW imaging using a 3-dimensional, coronal, spoiled gradient echo sequence (echo time [TE], 3.25 milliseconds; repetition time [TR], 2200 milliseconds; flip angle, 8 degrees; field of view [FOV], 100 100 mm; matrix, 256 256; slice thickness, 1 mm; and number of slices, 72). T1 and T2 measurement of the phantoms were performed using the Look-Locker sequence (TE = 1.32 milliseconds; TR = 3 milliseconds; number of inversion time [TI], 16; range of TI, 170–4985 milliseconds; ΔTI, 321 milliseconds; flip angle, 8 degrees; parallel imaging factor, 2; FOV, 352 352 mm; matrix, 192 192; slice thickness, 5 mm; intersection gap, 0; and number of slices, 3) and multiecho spin-echo sequence (TE = 26 milliseconds; ΔTE = 26 milliseconds; number of echoes = 15; TR = 5000 milliseconds; FOV, 103 103; matrix 128 128; section thickness, 3 mm; intersection gap, 0.6 mm; and number of slice, 3), respectively. Diffusion-weighted imaging was then performed using a single-shot, echo-planar imaging sequence with the following parameters: TE, 70 milliseconds; TR, 5000 milliseconds; receiver bandwidth, 1500 Hz per pixel; FOV, 288 141 mm; matrix, 196 69; slice thickness, 4 mm; intersection gap, 0.8 mm; and number of slices, 10. Bipolar DW gradients, that is, 15 b values of 0, 10, 20, 30, 40, 50, 75, 100, 150, 200, 300, 400, 500, 600, and 800 s/mm2, were applied in 3 orthogonal directions and were subsequently averaged. A k-space–based parallel imaging technique (generalized autocalibrating partially parallel acquisition, GRAPPA, Siemens Medical Solutions) was used with an acceleration factor of 2. Fat suppression was achieved using a chemical shift-selective fat suppression technique. Diffusion-weighted imaging of the phantoms was performed in a static state without flow infusion and with flow infusion using the peristaltic pump at the flow rates of 1, 2, and 3 mL/min. The same DW imaging was repeated 5 times with increasing or decreasing orders of flow rates alternatively every other repetition. As 2 phantoms could be imaged simultaneously, MR experiments were performed first for the coarse and the medium phantoms and then for the fine and the superfine phantoms. Measurement of Area Fraction of the Flowing Water Compartment of the Phantoms Using Micro-CT After completion of the MR experiments, the fluid within the phantoms was replaced with a 1:1 dilute solution of a blood-pool contrast agent (Fenestra VC; MediLumine Inc, Montreal, Quebec, Canada) in normal saline. Fenestra VC is an iodinated triglyceride nanoemulsion with a particle size of 10 to 300 nm.29 Because of its particle size far larger than the pore size (1.1 nm) of the gel beads, Fenestra VC resides in the area outside of the gel beads. Each phantom was scanned on a micro-CT scanner (SkyScan 1176; Bruker micro-CT, Kontich, Belgium) using the scan parameters of 8.94 μm resolution, 70 kVp, 357 μA, 360-degree rotation, 0.3-degree rotation step, 900 milliseconds exposure time, 5 frames averaging, and a 0.5-mm-thick aluminum filter. The images were reconstructed using NRecon v.1.6.9.18 software Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 IVIM Phantom Experiments FIGURE 2. IVIM phantom and phantom setting for MR experiments. A, A photograph of the 2 IVIM phantoms installed in the polyoxymethylene fixation device for MR imaging. Asterisks indicate the part of the phantoms filled with gel beads and where the MR images were obtained. B, A diagram of the phantom setting for the IVIM imaging experiment. Two phantoms were imaged simultaneously. Each phantom was connected to the peristaltic pump and to a glass beaker using water flow lines. Figure 2 can be viewed online in color at www.investigativeradiology.com. (Bruker micro-CT) with the modified Feldkamp cone-beam reconstruction algorithm, which resulted in 35 35-mm axial images in an 8-bit gray scale format (Fig. 3). On micro-CT images of the coarse phantom, individual gel beads and contrast-filled space outside of the gel beads were clearly differentiated, which allowed for direct quantification of the area fraction of the contrast-filled space. The area fraction of the flowing water compartment (FWC%), that is, percentage of the contrast-filled area to the entire cross-sectional area of the phantom, was quantified by a researcher (H.H.C) using the ImageJ software (v. 1.45i; National Institutes of Health, Bethesda, MD). However, for the remaining phantoms, direct quantification of FWC% was not reliable because of too small particle sizes for image resolution. Therefore, assuming that the relative size of the contrast-filled space was proportional to the Hounsfield unit (HU) of the phantoms, the FWC% of medium, fine, and superfine phantoms was estimated as FWC% of the coarse phantom (HU of the phantom of interest/HU of the coarse phantom). Data Analysis The DW image data were quantitatively analyzed according to monoexponential and biexponential models using 2 fitting methods, that is, free fitting and segmented fitting. The apparent diffusion coefficient (ADC) was calculated by least square monoexponential fitting of all b value data on a pixel-by-pixel basis according to the following equation2: S ¼ S0 e−b ADC ; ½1 where S is the signal intensity at a given b value and S0 is the signal intensity at b = 0 s/mm2. For biexponential IVIM analysis, DW signal decay was fitted to the following equation3: ½2 S ¼ S0 f e−b Dfast þ ð1 − f Þ e−b Dslow ; where f is the perfusion fraction, Dfast is perfusion-related diffusion that indicates the diffusion coefficient of microcirculation, and Dslow is pure molecular diffusion. With the unconstrained, free fitting method, all 3 parameters in the Equation 2 were simultaneously determined to minimize the distance between the fitted curve and the measured signal intensities. With the segmented fitting method, the IVIM parameters were sequentially determined as described in previous studies.13,21,30,31 First, under the assumption of the negligible contribution of the perfusion component at the range of high b values, Dslow was determined from monoexponential data fitting of b ≥ 200 s/mm2 data according to the following equation: S ¼ Sint e−b Dslow ; ½3 where Sint is the b = 0 intercept of the monoexponential fit of high b value data. Because the optimal b values separating perfusion and diffusion effects vary depending on the tissue type,32 the threshold b value of 200 s/mm2 in our study was determined by the b value where perfusion effect is negligible for most human organs based on previous studies.12,13,24,33 Then f can be estimated according to the following equation: f ¼ ðS 0 − Sint Þ = S0 ½4 with the Dslow and f, Dfast being calculated using a partially constrained, nonlinear regression of all data sets according to the Equation 2. For all fitting methods, the normalized root mean square error (RMSE), that is, RMSE/S0, was calculated as a parameter indicating the fitting accuracy. The product f·Dfast was calculated by multiplying f and Dfast to represent the overall amount of flow through the phantom.34 All fitting algorithms were written on ImageJ software as plug-in functions. One radiologist (J.H.L) measured the parameter values using 1.5-cm circular regions-of-interest located in the center of the phantoms. The average measurement on 3 consecutive DW images covering the midportion of the phantom was used as the representative parametric value. Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Lee et al Investigative Radiology • Volume 00, Number 00, Month 2016 FIGURE 3. Confocal microscopic images and micro-CT images of gel beads. A–D, Confocal microscopic images (100 magnification) of G-25 coarse (A), G-25 medium (B), G-25 fine (C), and G-25 superfine (D) gel beads, which have different particle size profiles. E–H, Micro-CT images of the coarse (E), medium (F), fine (G), and superfine (H) phantoms after an infusion of a blood-pool contrast agent. The individual gel beads are depicted as low-attenuating spheres on the images of the coarse phantom (E), although they are not clearly delineated on the images of and the medium (F), fine (G), and superfine (H) phantoms due to the limited spatial resolution of the CT images. Figure 3 can be viewed online in color at www.investigativeradiology.com. Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 ADC Measurement of the Ice Water Phantom To confirm the performance of our MR system in the acquisition of DW imaging, the ADC of the ice water phantom was measured 5 times using the same DW imaging sequence for the IVIM phantoms. The ice water phantom was prepared by immersing a sealed 15 mL tube of tap water into a 0.6-L plastic container filled with ice cubes according to the protocol reported previously.35 The mean ± standard deviation ADC value of the ice water phantom was 1.978 ± 0.005 10−3 mm2/s, which closely approximated the known diffusion coefficient of water at 0°C (1.1 10−3 mm2/s),36 indicating the adequacy of our MR system for DW imaging. Statistical Analysis The Spearman correlation coefficient was used to evaluate the correlation of the ADC and IVIM parameters with flow rates for each phantom and to analyze the correlation of the ADC and IVIM parametric values obtained at a flow rate of 1 to 3 mL/min with FWC% of the phantoms. The normalized RMSE values for monoexponential, free biexponential, and segmented biexponential fitting methods were summarized as the mean and standard deviation at each flow rate and were compared among the 3 fitting methods using the Friedman test and the post hoc Dunn multiple comparisons test. The measurement repeatability of the ADC or IVIM parameters across 5 repeated scans was evaluated using the within-subject coefficient of variation (CV) for the 3 fitting methods. A P value less than 0.05 was considered to indicate a statistically significant difference. Statistical analyses were performed using commercial software (IBM SPSS statistics version 21 software; IBM, Armonk, NY, and GraphPad InStat version 3.0; GraphPad Software, San Diego, CA). RESULTS Phantom Characteristics The T1 and T2 of the gadoterate meglumine solution were 192.8 milliseconds and 191.1 milliseconds, respectively; the T2 of the gadoterate meglumine solution was nearly the same as that of whole blood (ie, 190 milliseconds). The T1 and T2 of the phantoms were as follows: T1 = 182.3 milliseconds, T2 = 102.3 milliseconds for the coarse phantom; T1 = 181.1 milliseconds, T2 = 77.1 milliseconds for the medium phantom; T1 = 180.9 milliseconds, T2 = 73.4 milliseconds for the fine phantom; and T1 = 180.1 milliseconds, T2 = 62.7 milliseconds for the superfine phantom. The estimated FWC% were 31.4% for the coarse phantom, 27.8% for the medium phantom, 24.7% for the fine phantom, and 24.3% for the superfine phantom. IVIM Phantom Experiments ADC and IVIM Parameters of the Phantoms at Various Flow Rates Figure 4 shows examples of the signal decay curve of the coarse phantom seen on DW images; at no flow, the logarithm of the phantom signal decays linearly as a function of the b value, and thus indicating monoexponential decay. However, at a flow rate of 3 mL/min, the phantom signal curve shows an obvious biexponential decay, with a steeper slope at a range of lower b values than that at a range of higher b values. The ADC and IVIM parametric values of the phantoms are summarized in Table 1 and are displayed according to the various flow rates in Figure 5. The ADC values gradually increased as increasing flow rates and with statistically significant positive correlations (ρ = 0.659 to 0.969; P ≤ 0.002). There were some variations in Dslow with changing flow rates, although the correlation between the Dslow and the flow rates was not consistent across different phantoms and fitting methods. Interestingly, there was a tendency toward the highest Dslow value noted at the flow rate of 1 mL/min among the various flow rates. The f values consistently showed significant positive correlations with the flow rates in all of the phantoms for both free fitting (ρ = 0.838 to 0.969; P < 0.001) and segmented fitting (ρ = 0.938 to 0.969; P < 0.001). However, conflicting results were noted for Dfast between the 2 biexponential fitting methods. The Dfast values obtained with segmented fitting have a significantly positive correlation with the flow rate in all of the phantoms (ρ = 0.745 to 0.969; P < 0.001), whereas those obtained with free fitting showed opposite results, that is, a significantly inverse correlation with the flow rate (ρ = −0.527 to −0.791; P ≤ 0.017). Of note, high Dfast values (60.554 to 142.013 10−3 mm2/s) with large variations were obtained with free fitting at no flow state. As a result, the product f·Dfast for segmented fitting also had a strong positive correlation with the flow rates in all of the phantoms (ρ = 0.931 to 0.969; P < 0.001), while inconsistent results were noted for the flow rates for free fitting across different phantoms. When the parametric values obtained at a flow rate of 1 to 3 mL/min were compared with FWC% of the phantoms, statistically significant positive correlations with FWC% were noted for ADC (P = 0.695; P < 0.001), f for both free fitting (ρ = 0.510; P < 0.001) and segmented fitting (ρ = 0.545; P < 0.001), and f·Dfast for both free fitting (ρ = 0.481; P < 0.001) and segmented fitting (ρ = 0.532; P < 0.001). For ADC and all IVIM parameters for the coarse and medium phantoms, a large standard deviation of the parameter values was noted at the flow rate of 1 mL/min. When the biexponential fitting curves and the fitted parametric values for each repeated scan of 4 IVIM phantoms at the flow rate of 1 mL/min (Supplementary Figure 1, Supplemental Digital Content 1, http://links.lww.com/RLI/A255 and Supplementary Table 1, Supplemental Digital Content 2, http://links.lww.com/RLI/A256) were reviewed, in contrast to the fine and superfine phantoms, signal FIGURE 4. Diffusion-weighted, signal decay curves of the G-25 coarse phantom at no flow (A) and at a flow rate of 3 mL/min (B). Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 Lee et al TABLE 1. Summary of the ADC and the IVIM Parameters Monoexponential Phantoms Coarse Medium Fine Superfine Free Biexponential Segmented Biexponential Flow rate ADC Dslow f (%) Dfast Dslow f (%) Dfast 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 1.670 ± 0.103 2.018 ± 0.266 2.317 ± 0.039 2.439 ± 0.019 1.491 ± 0.013 1.771 ± 0.187 1.801 ± 0.010 1.777 ± 0.005 1.499 ± 0.010 1.732 ± 0.009 1.879 ± 0.005 1.905 ± 0.003 1.429 ± 0.012 1.607 ± 0.088 1.809 ± 0.048 1.885 ± 0.034 1.632 ± 0.098 1.841 ± 0.216 1.313 ± 0.012 1.323 ± 0.006 1.464 ± 0.011 1.629 ± 0.112 1.402 ± 0.013 1.302 ± 0.009 1.476 ± 0.011 1.630 ± 0.010 1.543 ± 0.003 1.396 ± 0.003 1.435 ± 0.010 1.565 ± 0.059 1.537 ± 0.029 1.409 ± 0.023 2.0 ± 0.3 8.2 ± 2.0 40.6 ± 0.8 40.1 ± 0.3 1.6 ± 0.1 7.0 ± 3.3 19.5 ± 0.3 22.4 ± 0.4 1.5 ± 0.1 5.3 ± 0.1 16.1 ± 0.1 23.4 ± 0.2 1.2 ± 0.2 3.1 ± 0.9 13.4 ± 1.6 22.2 ± 0.3 75.960 ± 22.654 16.462 ± 16.082 6.713 ± 0.059 9.895 ± 0.074 60.554 ± 29.561 13.560 ± 11.249 7.018 ± 0.061 8.157 ± 0.111 86.053 ± 59.923 13.155 ± 9.277 7.715 ± 0.017 7.785 ± 0.039 142.013 ± 121.750 59.461 ± 43.242 7.706 ± 0.121 7.774 ± 0.129 1.618 ± 0.094 1.804 ± 0.208 1.635 ± 0.021 1.478 ± 0.005 1.458 ± 0.011 1.622 ± 0.123 1.498 ± 0.009 1.407 ± 0.005 1.467 ± 0.011 1.617 ± 0.008 1.591 ± 0.003 1.516 ± 0.003 1.432 ± 0.014 1.556 ± 0.059 1.577 ± 0.024 1.521 ± 0.022 2.2 ± 0.4 8.5 ± 2.2 25.0 ± 0.4 33.4 ± 0.4 1.5 ± 0.1 6.3 ± 2.7 13.1 ± 0.1 16.5 ± 0.1 1.4 ± 0.1 5.1 ± 0.1 12.3 ± 0.1 16.8 ± 0.1 0.9 ± 0.1 2.5 ± 0.9 10.2 ± 1.2 15.7 ± 0.4 8.073 ± 0.540 8.623 ± 1.062 10.153 ± 0.048 12.014 ± 0.043 8.382 ± 0.487 8.665 ± 1.773 9.435 ± 0.036 10.801 ± 0.084 7.353 ± 0.183 8.043 ± 0.097 9.237 ± 0.054 10.556 ± 0.038 7.162 ± 0.848 7.641 ± 0.432 9.307 ± 0.090 10.561 ± 0.077 Data are presented as mean ± standard deviation. ADC indicates apparent diffusion coefficient; IVIM, intravoxel incoherent motion; Dslow, slow diffusion coefficient; f, perfusion fraction; Dfast, fast diffusion coefficient. fitting curves of the coarse and the medium phantoms revealed the fitting results, which deemed to be outlier. When these results were excluded, the standard deviation of the parametric values decreased, especially for the medium phantom. However, the overall trend in parametric values including the tendency toward the highest Dslow value at the flow rate of 1 mL/min did not change after excluding the outlier results. Fitting Error and Measurement Repeatability of the Fitting Algorithms Figure 6 displays normalized RMSE representing the fitting error for the 3 fitting methods at various flow rates. The normalized RMSE was least for free fitting, followed by segmented fitting and monoexponential fitting, and with a statistically significant difference among the 3 fitting methods at all of the flow rates (P < 0.001). This indicates that the model curves obtained with free fitting best represent the actual data. Of note, the fitting error for monoexponential fitting increases with an increasing flow rate, and thus indicating the inaccuracy of the monoexponential model for explaining the actual biexponential signal decay in the presence of flow within the phantoms. The CV values representing measurement repeatability over 5 repeated scans are summarized in Table 2. The CV values for ADC and Dslow with free and segmented fittings were similar to each other. Overall, the CV values for the flow-related parameters, that is, f, Dfast, and f·Dfast, were larger than those for ADC and Dslow. The CV values for Dfast and f·Dfast for free fitting were obviously larger than those for segmented fitting, and thus indicating poorer measurement repeatability for those parameters with free fitting that those with segmented fitting. DISCUSSION Through the MR experiment using IVIM phantoms with various fractions of flowing water compartments at various flow rates, we evaluated the flow effects on the ADC and IVIM parameters. As expected, the ADC increased in proportional to the flow rates, which reconfirmed that the ADC reflects both the diffusion and the perfusion components. Unlike the theoretic definition of Dslow, which is the coefficient of brownian motion and is not related with microvascular flow,1,2 our results showed some variations in Dslow with changing flow rates, and thus indicating the existence of flow effects on the diffusion signal intensity even at higher b values (200 ≤ b ≤ 800 s/mm2). Of note, there was a tendency toward a higher Dslow at the lowest infusion flow rate (1 mL/min) compared with the Dslow values at no flow and at higher infusion flow rates (2 and 3 mL/min). One possible explanation for these observations would be the contribution of slowflow velocities to the signal decay at higher b values. After infusion of the solution into the phantoms, a wide range of flow velocities may have been generated within the phantoms, and with slow velocities being more dominant at a slower infusion flow rate. As the IVIM model separates 2 components of water motion, that is, diffusion versus perfusion, based on the magnitude of movement at a given time, a very sluggish flow may have resulted in signal decay at higher b values, and thus leading to alteration in Dslow. A previous phantom experiment using sponge phantoms also reported a variation of Dslow with change in flow rates.17 As the fast diffusion coefficient, that is, Dfast, is defined by blood velocity and the mean capillary segment length according to the IVIM theory,1 this parameter was expected to be correlated with the flow rates in our phantom experiments. The findings obtained with segmented fitting were consistent with our expectations and confirmed that Dfast reflects flow velocity. However, the results of Dfast obtained with free fitting were completely opposite to those obtained with segmented fitting. We hypothesized that these unexpected findings may have resulted from the mathematical instability of the free fitting method. Because of the high degree of freedom, simultaneous fit for all 3 parameters in the biexponential model may lead to inaccurate and unreliable fitting results. This hypothesis is further supported by our finding showing a poorer measurement repeatability of Dfast with free fitting than with segmented fitting. The perfusion fraction, that is, f, is defined as the fraction of flowing water.1,2 Our results demonstrating a positive correlation between the FWC% of the phantoms and f proved the dependency of f on the fraction of flowing water. However, our results also demonstrated a correlation between f and the flow rate, and thus suggesting Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 IVIM Phantom Experiments FIGURE 5. The ADC and IVIM parameters of the phantoms according to the various flow rates. The graphs display the ADC values (A), Dslow values obtained with free fitting (B), Dslow values obtained with segmented fitting (C), f values obtained with free fitting (D), f values obtained with segmented fitting (E), Dfast values obtained with free fitting (F), Dfast values obtained with segmented fitting (G), f·Dfast values obtained with free fitting (H), and f·Dfast values obtained with segmented fitting (I) for the coarse, medium, fine, and superfine phantoms at various flow rates. Data are the mean parameter values, and the error bars indicate the range of 1.96 standard deviation. For some data points, error bars were not expressed in graphs due to the very small standard deviations of those data points. Figure 5 can be viewed online in color at www.investigativeradiology.com. the influence of flow velocities on f in our phantoms. Though not yet fully understood, there may be a few possible explanations for this finding. First, IVIM-based analysis of DW imaging may not allow for complete separation of the 2 components of perfusion, that is, the fraction of flowing water and the flow velocity. As a result, both of these components of perfusion may have influence on f. Another possible explanation may be the contribution of fluid exchange between the static and flowing water compartments to f. Similarly to transcapillary fluid exchange through capillary fenestrations in biologic tissue, water may have moved across the surface pores of gel beads in our phantoms, and this water movement may be more facilitated at a higher flow infusion rate. As transcapillary fluid exchange is not modeled as a specific parameter in the IVIM theory, this intercompartmental fluid movement may have been incorporated into f. The product f·Dfast is a parameter reflecting the overall amount of water flow or blood flow in biologic tissue.34 As expected, f·Dfast obtained with segmented fitting was proportional to the flow rate. However, f·Dfast obtained with free fitting showed inconsistent results across different phantoms, which is considered as a consequence of the aforementioned inaccurate estimation of Dfast using free fitting. Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 Lee et al Regarding the 2 fitting methods for IVIM analysis, despite the higher fitting accuracy, that is, smaller normalized RMSE value, of free fitting compared with that of segmented fitting, segmented fitting may be a stronger fitting method for IVIM analysis than free fitting in terms of the accuracy and reliability, especially for estimating Dfast. Our findings repeated the results of previous computer simulation studies, which also demonstrated the higher accuracy and reliability of the measurement of IVIM parameters using the segmented fitting method than with the free fitting method.21,37,38 Our study does have some limitations. First, our 2-compartment IVIM phantoms simplistically simulate biologic tissue, although they do not completely account for the structural complexity of normal or pathologic tissue. Therefore, our study did not evaluate other factors such as cellularity,39,40 interstitial fluid pressure,34 and the various size of capillary fenestration that potentially affect the ADC and IVIM parameters in biologic tissue. Unlike the gadoterate meglumine solution that was used in our study to simulate blood perfusion, blood contains blood cells and macromolecules such as albumin that may influence water diffusion. Thus, our study results do not reflect the influence of these blood contents on IVIM parameters. Second, considering the fact that molecular diffusion is highly dependent on temperature,36 the difference in the temperature between our phantoms and human body may have been a source of bias in our results. Finally, the results of our phantom experiment, which was performed in the ideal experimental condition, do not address the various sources of measurement error in in vivo human imaging. Despite these limitations, our results obtained from the phantom experiments of controllable perfusion-related factors can validate the IVIM theory and provide valuable information for the interpretation of each IVIM parameter. In conclusion, the IVIM model allows for an approximate segmentation of molecular diffusion and perfusion, and with a minor contribution of the perfusion effect on Dslow. Perfusion parameters, that is, f and Dfast, can provide a rough estimation of the flowing water fraction FIGURE 6. A graph displaying the normalized root mean squared error (RMSE) for monoexponential fitting, free biexponential fitting, and segmented biexponential fitting at various flow rates. Data points represent the mean normalized RMSE values, and the error bar indicates the range of 1.96 standard deviation of normalized RMSE. For some data points, error bars were not expressed in graphs due to the very small standard deviations of those data points. Figure 6 can be viewed online in color at www.investigativeradiology.com. TABLE 2. CV Values Representing the Measurement Repeatability of the ADC and the IVIM Parameters Over 5 Repeated Scans Free Fitting ADC Dslow f Dfast f·Dfast Segmented Fitting 4.97% 4.57% 7.78% 112.31% 40.92% 4.36% 8.99% 6.59% 11.68% CV indicates coefficient of variation; ADC, apparent diffusion coefficient; IVIM, intravoxel incoherent motion; Dslow, slow diffusion coefficient; f, perfusion fraction; Dfast, fast diffusion coefficient; f·Dfast, product of f and Dfast. and flow velocity. For IVIM-based analysis of DW images, segmented fitting may be a stronger method than free fitting. REFERENCES 1. Le Bihan D, Breton E, Lallemand D, et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology. 1988;168:497–505. 2. Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology. 1986;161:401–407. 3. Le Bihan D, Turner R, MacFall JR. Effects of intravoxel incoherent motions (IVIM) in steady-state free precession (SSFP) imaging: application to molecular diffusion imaging. Magn Reson Med. 1989;10:324–337. 4. Lemke A, Laun FB, Simon D, et al. An in vivo verification of the intravoxel incoherent motion effect in diffusion-weighted imaging of the abdomen. Magn Reson Med. 2010;64:1580–1585. 5. Chandarana H, Kang SK, Wong S, et al. Diffusion-weighted intravoxel incoherent motion imaging of renal tumors with histopathologic correlation. Invest Radiol. 2012;47:688–696. 6. Chow AM, Gao DS, Fan SJ, et al. Liver fibrosis: an intravoxel incoherent motion (IVIM) study. J Magn Reson Imaging. 2012;36:159–167. 7. Joo I, Lee JM, Han JK, et al. Intravoxel incoherent motion diffusion-weighted MR imaging for monitoring the therapeutic efficacy of the vascular disrupting agent CKD-516 in rabbit VX2 liver tumors. Radiology. 2014;272:417–426. 8. Klauss M, Lemke A, Grunberg K, et al. Intravoxel incoherent motion MRI for the differentiation between mass forming chronic pancreatitis and pancreatic carcinoma. Invest Radiol. 2011;46:57–63. 9. Lee SS, Byun JH, Park BJ, et al. Quantitative analysis of diffusion‐weighted magnetic resonance imaging of the pancreas: usefulness in characterizing solid pancreatic masses. J Magn Reson Imaging. 2008;28:928–936. 10. Lemke A, Laun FB, Klauss M, et al. Differentiation of pancreas carcinoma from healthy pancreatic tissue using multiple b-values: comparison of apparent diffusion coefficient and intravoxel incoherent motion derived parameters. Invest Radiol. 2009;44:769–775. 11. Lewin M, Fartoux L, Vignaud A, et al. The diffusion-weighted imaging perfusion fraction f is a potential marker of sorafenib treatment in advanced hepatocellular carcinoma: a pilot study. Eur Radiol. 2011;21:281–290. 12. Luciani A, Vignaud A, Cavet M, et al. Liver cirrhosis: intravoxel incoherent motion MR imaging—pilot study 1. Radiology. 2008;249:891–899. 13. Patel J, Sigmund EE, Rusinek H, et al. Diagnosis of cirrhosis with intravoxel incoherent motion diffusion MRI and dynamic contrast-enhanced MRI alone and in combination: preliminary experience. J Magn Reson Imaging. 2010;31:589–600. 14. Suh CH, Kim HS, Lee SS, et al. Atypical imaging features of primary central nervous system lymphoma that mimics glioblastoma: utility of intravoxel incoherent motion MR imaging. Radiology. 2014;272:504–513. 15. Thoeny HC, Binser T, Roth B, et al. Noninvasive assessment of acute ureteral obstruction with diffusion-weighted MR imaging: a prospective study. Radiology. 2009;252:721–728. 16. Thoeny HC, Zumstein D, Simon-Zoula S, et al. Functional evaluation of transplanted kidneys with diffusion-weighted and BOLD MR imaging: initial experience. Radiology. 2006;241:812–821. 17. Cho GY, Kim S, Jensen JH, et al. A versatile flow phantom for intravoxel incoherent motion MRI. Magn Reson Med. 2012;67:1710–1720. 18. Henkelman RM, Neil JJ, Xiang QS. A quantitative interpretation of IVIM measurements of vascular perfusion in the rat brain. Magn Reson Med. 1994;32: 464–469. Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes. Investigative Radiology • Volume 00, Number 00, Month 2016 19. Lorenz CH, Pickens DR, Puffer DB, et al. Magnetic resonance diffusion/perfusion phantom experiments. Magn Reson Med. 1991;19:254–260. 20. Turner R, Le Bihan D, Maier J, et al. Echo-planar imaging of intravoxel incoherent motion. Radiology. 1990;177:407–414. 21. Cho GY, Moy L, Zhang JL, et al. Comparison of fitting methods and b-value sampling strategies for intravoxel incoherent motion in breast cancer. Magn Reson Med. 2015;74:1077–1085. 22. Chung SR, Lee SS, Kim N, et al. Intravoxel incoherent motion MRI for liver fibrosis assessment: a pilot study. Acta Radiol. 2015;56:1428–1436. 23. Lee Y, Lee SS, Kim N, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology. 2014;274:405–415. 24. Sigmund EE, Vivier PH, Sui D, et al. Intravoxel incoherent motion and diffusiontensor imaging in renal tissue under hydration and furosemide flow challenges. Radiology. 2012;263:758–769. 25. Biosciences A. Gel filtration: Principles and methods. Uppsala, Sweden: Amersham Biosciences AB; 2002. 26. Erickson HP. Size and shape of protein molecules at the nanometer level determined by sedimentation, gel filtration, and electron microscopy. Biol Proced Online. 2009;11:32–51. 27. Sarin H. Physiologic upper limits of pore size of different blood capillary types and another perspective on the dual pore theory of microvascular permeability. J Angiogenes Res. 2010;2:14. 28. Chen JJ, Pike GB. Human whole blood T2 relaxometry at 3 Tesla. Magn Reson Med. 2009;61:249–254. 29. Hallouard F, Anton N, Choquet P, et al. Iodinated blood pool contrast media for preclinical x-ray imaging applications—a review. Biomaterials. 2010;31:6249–6268. 30. Callot V, Bennett E, Decking UK, et al. In vivo study of microcirculation in canine myocardium using the IVIM method. Magn Reson Med. 2003;50:531–540. IVIM Phantom Experiments 31. Wirestam R, Borg M, Brockstedt S, et al. Perfusion-related parameters in intravoxel incoherent motion MR imaging compared with CBV and CBF measured by dynamic susceptibility-contrast MR technique. Acta Radiol. 2001;42: 123–128. 32. Wurnig MC, Donati OF, Ulbrich E, et al. Systematic analysis of the intravoxel incoherent motion threshold separating perfusion and diffusion effects: Proposal of a standardized algorithm. Magn Reson Med. 2015;74:1414–1422. 33. Iima M, Yano K, Kataoka M, et al. Quantitative non-Gaussian diffusion and intravoxel incoherent motion magnetic resonance imaging: differentiation of malignant and benign breast lesions. Invest Radiol. 2015;50:205–211. 34. Kim S, Decarlo L, Cho GY, et al. Interstitial fluid pressure correlates with intravoxel incoherent motion imaging metrics in a mouse mammary carcinoma model. NMR Biomed. 2012;25:787–794. 35. Malyarenko D, Galban CJ, Londy FJ, et al. Multi-system repeatability and reproducibility of apparent diffusion coefficient measurement using an ice-water phantom. J Magn Reson Imaging. 2013;37:1238–1246. 36. Simpson J, Carr H. Diffusion and nuclear spin relaxation in water. Phys Rev. 1958; 111:1201–1202. 37. Pekar J, Moonen CT, van Zijl P. On the precision of diffusion/perfusion imaging by gradient sensitization. Magn Reson Med. 1992;23:122–129. 38. Lemke A, Stieltjes B, Schad LR, et al. Toward an optimal distribution of b values for intravoxel incoherent motion imaging. Magn Reson Imaging. 2011; 29:766–776. 39. Gauvain KM, McKinstry RC, Mukherjee P, et al. Evaluating pediatric brain tumor cellularity with diffusion-tensor imaging. AJR Am J Roentgenol. 2001;177: 449–454. 40. Matsumoto Y, Kuroda M, Matsuya R, et al. In vitro experimental study of the relationship between the apparent diffusion coefficient and changes in cellularity and cell morphology. Oncol Rep. 2009;22:641–648. Copyright © 2016 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. This paper can be cited using the date of access and the unique DOI number which can be found in the footnotes.