Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
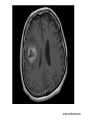
Encephalitis Brain Abscess Reşat Özaras, MD, Prof. Infection Dept. • A 37-year-old male • Headache, stupor, tendency to sleep, fever, unaware to recognise the time and the place... Acute Encephalitis • The inflammation of the parenchyma of the brain especially that of the cerebral cortex The inflammation of the CNS • Encephalitis… the parenchyma...mostly due to viral infections • Meningitis… the meninges... mostly due to bacterial infections Symptoms • Fever • Headache • Mental changes • • • • • • • • Confusion Hallucinations Personality changes Diplopia Fatigue Tremors Rash Loss of consciousness Acute Encephalitis • Mostly due to viral inf. – Herpes simplex virus (HSV) (the most common etiology of acute sporadic encephalitis) – Arboviruses – arthropod-borne virus (outbreaks in summer time…mosquitos and ticks) – Varicella zoster virus (VZV) patients) (immunosuppressed HSV-1 • The most common etiology of acute sporadic encephalitis • HSV-1 – acquired in childhood period, – re-activates after years HSV-1 • Primary infection; • On the mucosa of oropharynx, mostly asymptomatic • fever, pain, dysphagia • 2-3 weeks • Following primary infection, a latent infection in trigeminal ganglion HSV-1 • Inferior and medial temporal lobe • Orbito-frontal lobe • Limbic structures Inflammation necrotizing lesions Hemorrhagic necrosis in herpes encephalitis especially when remains untreated. HSV-1 Widespread edema and subarachnoid hemorrhage areas in medial temporal and orbitofrontal regions HSV-1 • • • • • Fever Unilateral or generalized headache Mental changes Focal seizures Focal neurological deficits • Dysphasia • Hemiparesis VZV • • • • Primary infection… chickenpox Latent infection thereafter The commonest reactivation… herpes labialis Chickenpox, herpes labialis and zona may be complicated with encephalitis Epstein Barr Virus • Causes infectious mononucleosis • May cause encephalitis • Direct invasion of CNS or immune mechanisms • Cortex, brain stem, basal ganglia, temporal lobe CMV • Encephalitis in both immunocompetent and immunosuppressed • Risk is higher – immunosuppressed, – organ transplanted – HIV-infected patients • Organ transplantation, highest risk… CMV (-) donor to CMV (+) recipient HIV • In 10-50% of AIDS patients, HIV infection in CNS • Multinuclear giant cells in gray matter and central white matter are pathognomonic. Rabies • • • • • • Lyssavirus Acute progresive fatal encephalitis. Transmitted with infected saliva of the animal Incubation period: 5 days-6 mo.(20-60 days) III, IV and IXth canial nerve palsies Prodromal period, neurological disease period, paralysis, coma, and death. Mumps • The commonest complication; inflammation in CNS • A pleocytosis in CSF in half of the cases • In 5-30%: headache, vomiting, neck stiffnes Clinical Evaluation • History • PE • Neck stiffness • CBC • Biochemistry • Culture • Imaging • Serology • CSF analysis History • • • • • • • Season Localisation Travel Occupational exposure Exposure to animals Immunization Immune status of the patient Lab • • • • CBC Renal and hepatic tests Coagulation studies Plain chest X-ray • CSF analysis • Cranial imaging Nonspecific Main diagnostic methods Cranial Imaging MRI • Sensitive for early period HSV encephalitis • Edema in orbitofrontal and temporal regions CT • Less sensitive than MRI Herpes simplex encepalitis CT(A) and MRI (B-F) temporal lobe involvement CSF Analysis • Cell count: 10-2000 cells/mm3 • • • • • • • • • Mostly <500 cell/mm3 Lymphocyte predominance Erythrocytes (in 80% of the cases) Normal CSF findings in 10% Glucose (mg/dl): normal or low CSF glucose/serum glucose: normal (>0.6) or low Protein (mg/dl): >50 Gram staining: no microorganisms Culture: none Microbiology • HSV PCR: For the first 24-48 hours, detecting HSV DNA by PCR in CSF: – specific (100%) and – sensitive (75-98%) Herpes simplex encephalitis; Neurons including Cowdry A type intranuclear inclusion bodies. Hematoxylen-Eosin, X400. Treatment • If shock/hypotension exists, crystaloid infusion • If unconscious, provide airway/breathing • Seizure, lorazepam 0.1 mg/kg, IV Treatment • For encephalitis, give acyclovir Treatment • Acyclovir IV, 14 – 21 days – HSV encephalitis – VZV encephalitis Some keys • Atypical lymphocytes on peripheral smear… IMN • High amylase … Mumps Complications Acute period • Seizure • Inappropriate ADH synd. • Intracranial pressure inc. • Resp. arrest • Coma • Death Chronic period • • • • • • • • • • Chronic fatigue Depression Personality changes Gait disorders Memory disorders Speech disorders Visual problems Mental retardation Hemiplegia Seizure Prognosis • The virulence of the virus • Patient’s; – previous health status – immune status (chemotherapy, transplantation, AIDS) – age(<1, and >55 years) – any neurological symptoms Prognosis • Being in coma on prsentation: severe inflammation in the brain, poor prognosis • Treated – Mortality… 20% – Morbidity… 40% • Untreated – Mortality … 50-75% – Morbidity… 100% Brain Abscess • Focal collection in the brain parenchyma due to – Infection – Trauma – Surgery Pathogenesis • Hematogenous: multiple abscess – Chronic pulmonary inf. (lung abscess, empyema…) – Skin inf. – Pelvic inf. – Intraabdominal inf. – Bacterial endocarditis – Cyanotic congenital heart dis. • Direct transmission – Subacute or chronic otitis media, mastoiditis (inferior temporal lobe and cerebellum) – Frontal or ethmoid sinusitis (frontal lobes) – Dental infections (frontal lobes) • Early lesion (first 1-2 weeks): – The borders are not clearly defined, localised edema – Inflammation, no necrosis – “Cerebritis” • After 2-3 weeks, necrosis • A fibrous capsule Etiology • Aerobs+Anaerobs Signs&Symptoms • Headache • Fever • Neck stiffness • Mental changes • Nausea, vomiting Warning • LP is contraindicated! Diagnosis • Imaging –MRI –CT Treatment • Intervention • Antibiotics – Ceftriaxone + metronidazole Mortality 0-30 % www.rochester.edu