Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
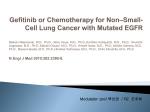
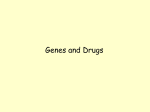
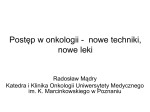
Vol. 10, 4607– 4613, July 15, 2004 Clinical Cancer Research 4607 Perspective Development of the Novel Biologically Targeted Anticancer Agent Gefitinib: Determining the Optimum Dose for Clinical Efficacy Michael Wolf,1 Helen Swaisland,2 and Steven Averbuch1 1 Clinical Research, AstraZeneca Pharmaceuticals, Wilmington, Delaware, and 2AstraZeneca Pharmaceuticals, Macclesfield, Cheshire, United Kingdom ABSTRACT The emergence of novel, biologically targeted anticancer agents such as gefitinib (‘Iressa’, ZD1839) has raised the question of how the dose for later-stage clinical development and clinical use is best determined. For cytotoxic drugs, because toxic effects and antitumor activity often fall within the same dose range and are dose dependent, the clinically used dose will depend on the therapeutic window. Therefore, the maximum tolerated dose identified in Phase I trials is typically used to determine the dose level for Phase II and III trials. However, because biologically targeted agents are expected to provide clinical benefits that are not predicted by surrogate end points of toxicity to normal replicating tissue, new Phase I trials have been designed to determine the optimum biological dose for use in further studies. A large, multifaceted Phase I program was designed to evaluate the pharmacokinetics, safety, efficacy, and targeted biological activity of a once-daily oral dose of gefitinib. The maximum tolerated dose was >700 mg/day, although doses as low as 150 mg/day provided (a) plasma concentrations sufficient for pharmacological activity, (b) evidence of targeted biological effect, and (c) antitumor activity. From these observations, two large Phase II trials (‘Iressa’ Dose Evuluation in Advanced Lung Cancer 1 and 2) evaluated 250- and 500-mg/day doses of gefitinib in patients with advanced non-small cell lung cancer (NSCLC). As predicted from the Phase I trials, doses >250 mg/day provided no additional efficacy benefit, whereas adverse effects increased in a dose-dependent manner. Consequently, the recommended dose of gefitinib in NSCLC is 250 mg/day. The early clinical trial development of gefitinib provides a model for the development of novel, noncytotoxic anticancer agents. Received 1/12/04; revised 4/12/04; accepted 4/19/04. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Note: S. Averbuch is currently at Merck Pharmaceuticals, Wynnewood, PA. ‘Iressa’ is a trademark of the AstraZeneca group of companies. Requests for reprints: Helen Swaisland, AstraZeneca, Alderley Park, Macclesfield, Cheshire, SK10 4TG, United Kingdom. Phone: 44 (0) 1625 510340; Fax: 44 (0) 1625 585626; E-mail: helen.swaisland@ astrazeneca.com. INTRODUCTION In recent years, the search for novel anticancer agents has moved from cytotoxic agents to biologically targeted agents (which are primarily antiproliferative) to avoid the traditional toxic effects of anticancer therapy and to develop more selective and effective agents. Traditionally, Phase I trials of anticancer agents aim to identify toxicities, pharmacokinetic (PK) profiles, and the dose for Phase II trials. For cytotoxic agents, antitumor activity and toxic effects generally occur within a similar dose range, and the dose selected is usually the maximum tolerated dose (MTD; Fig. 1A; Ref. 1). However, for biologically targeted agents that are cytostatic, the maximum biological effect may occur at doses lower than the MTD (Fig. 1B) and alternative end points based on biological and/or clinical activity rather than toxicity might be more appropriate (2). Alternative end points may include changes in tumor markers, prolonged disease stabilization, improvements in disease-related symptoms, pharmacodynamic assessment of the biological activity of the target molecule, and pharmacokinetic studies. One promising biological target is the epidermal growth factor receptor (EGFR), because EGFR activation initiates a signaling cascade that leads to a number of processes involved in tumor progression, including increased proliferation, angiogenesis and invasion, and decreased apoptosis (3). In addition, a variety of tumors express EGFR (4), giving rise to the wide application of EGFR-targeted agents such as gefitinib (‘Iressa,’ ZD1839), an EGFR tyrosine kinase inhibitor. This review will discuss how the strategic aim of defining the optimum biological dose (OBD) of gefitinib in the early clinical trial program was achieved. DESIGNING A CLINICAL TRIAL FOR GEFITINIB Several challenges were present in designing the Phase I clinical trials of gefitinib, because this agent was expected to be cytostatic rather than cytotoxic; hence, objective tumor responses might not be expected. These challenges included a scarcity of precedents, the way in which “biological activity” was defined, the integration of outcomes across multiple tumor types in Phase I trials (because the OBD and clinical activity may not necessarily be the same for all tumor types), the relationship between biological activity and clinical outcome, and unknown PK and pharmacodynamic (PD) relationships. Thus, four large, multicenter, randomized, oncology-like and clinical pharmacology-like Phase I trials were designed. Two conventional oncology-like Phase I trials used dose escalation to identify the MTD and characterize the PK of gefitinib in patients; these trials also ascertained whether there was any evidence of antitumor activity (objective tumor response and stable disease). Two more sophisticated pharmacology-like Phase I trials were split into Part A (dose escalation) and Part B (randomized dose response). Up to four doses from Part A were to be evaluated in Part B, with alternative efficacy Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. 4608 Gefitinib: Determining the Optimum Dose for Efficacy Fig. 1 Idealized curves reflecting molecular target effects, antitumor effects, and toxicity as functions of dose for (A) a typical cytotoxic agent whose toxicity occurs at roughly the same dose as target effects and (B) a hypothetical target-based antiproliferative agent whose target effects occur at lower doses than do toxic effects (1). MTD, maximum tolerated dose; OBD, optimum biological dose. end points used to collate tumor-specific PK/PD data for each patient (tumor measurements, serum tumor markers, baseline and day-28 tumor EGFR levels, and cell proliferation indices from skin and tumor biopsies, where available). Data from these four trials would enable dose levels for the Phase II/III trials to be determined. If a single dose level for Phase II/III trials could not be determined, a blinded-review panel would assess evaluable cases using the collated PK/PD data available from Part B of the two pharmacology-like Phase I trials. The relevance of the data (magnitude of change, reliability, and methodology) would be weighed in a prospective algorithm to assign an overall targeted biological effect (TBE) outcome (yes/no). Regression analysis from dose-response (for the TBE) and exposure-response relationships would be constructed, from which dose selection could be derived. Evidence of TBE would be based on tumor shrinkage, changes in tumor EGFR-specific markers [EGFR expression, phosphorylated EGFR, phospho-p44/42 mitogen-activated protein kinase (pMAPK)], proliferation (Ki67) or apoptosis, and skin EGFR markers and serum tumor markers. PHASE I TRIALS OF GEFITINIB Initial Phase I trials performed in healthy volunteers showed that oral administration of gefitinib given once on day 1 (50, 100, 250 or 500 mg) or daily for 14 days (100 mg/day) was feasible, and that PK parameters that were used to assess exposure to gefitinib increased in proportion to dose (5). Four multicenter Phase I trials then evaluated the safety profile of gefitinib (50 –1000 mg/day) in more than 250 patients with a wide range of solid tumors that were known to express EGFR [e.g., non-small cell lung cancer (NSCLC) and head and neck, breast, colorectal, prostate, and ovarian cancers], although baseline expression levels were not determined (6 –9). All of the patients had histologically confirmed advanced or metastatic tumors that were refractory to conventional chemotherapy or hormone therapy, were aged ⱖ18 years, and had a life expectancy of ⱖ12 weeks and a WHO performance status of 0⫺1. Oncology-like Trials. Two conventional oncology-like Phase I monotherapy trials evaluated the safety of gefitinib (50 –1000 mg/day) given daily for 14 days in 95 patients, followed by 14 days’ observation (6, 7). Adverse events (AEs) occurred at doses ⱖ50 mg/day, with the most commonly reported AEs being mild-to-moderate (grade 1–2) acne-like rash, diarrhea, nausea, anorexia, vomiting, and asthenia. The frequency of AEs such as skin rash and diarrhea increased with dose, and the MTD was identified as 700 mg/day. Exposure to gefitinib increased with dose; in patients taking 100 –700 mg/ day, Cmax (peak plasma concentrations) and AUC0 –24 (area under the curve from 0 to 24 h) increased from 105 to 2146 ng/ml and 1860 to 36077 ng䡠h/ml, respectively. Despite a 6 – 8fold interpatient variability at each dose level, biologically relevant plasma concentrations [⬎100 ng/ml, equivalent to the in vitro IC90 (inhibitory concentration) for KB oral carcinoma cells (3)] were generally maintained at doses ⬎100 mg/day across the 24-h dosing period. Disease control in these trials was observed across the whole dose range; objective responses in 9 patients with NSCLC were seen at 225 mg/day, 300 mg/day, 400 mg/ day, 525 mg/day, and 700 mg/day; and stable disease in 15 patients (5 with NSCLC) was seen at 50 mg/day, 100 mg/day, 225 mg/day, 400 mg/day, 525 mg/day, and 700 mg/day (6, 7). For those nine patients with objective responses, steady-state trough plasma concentrations ranged between 63 and 1873 ng/ml (10); interestingly, two patients taking 225 and 300 mg/day had steady-state trough plasma concentrations of gefitinib ⬍100 ng/ml, which suggests that plasma levels ⬍100 ng/ml may result in objective responses in patients with NSCLC. Oncology/Pharmacology-like Trials. Two pharmacologylike Phase I trials determined a dose range for gefitinib given orally on a daily basis and further defined the OBD (8, 9). Secondary objectives were to (a) monitor gefitinib exposure; (b) investigate the feasibility and sensitivity of the Functional Assessment of Cancer Therapy (FACT) questionnaire for lung, head and neck, breast, colorectal, prostate and ovarian cancer; (c) assess improvements in NSCLC-related symptoms using the seven-item Lung Cancer Subscale of FACT-Lung (11); and (d) select tumor types for Phase II/III studies. Up to 14 patients Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. Clinical Cancer Research 4609 were enrolled at each planned dose level (150 –1000 mg/day gefitinib). A total of 157 patients received 150-1000 mg/day gefitinib (Table 1), with the MTD identified in one trial as 800 mg/day (8) and not reached in the other (9). The most commonly reported AEs (grade 1–2 diarrhea and skin rash) were dose related across the range studied (150 – 800 mg/day), with dosage interruptions and reductions generally required only at doses ⬎600 mg/day. There was no clear dose-response relationship for disease control, which was observed at all doses (Table 2), with 45 patients receiving gefitinib for ⱖ3 months, 20 patients receiving gefitinib for ⱖ6 months, and 7 patients receiving gefitinib for ⬎1 year (1 with a partial response and 6 with stable disease). Patients with NSCLC who had stable disease for ⱖ6 months also had improvements or stabilization in diseaserelated symptoms, whereas those patients with disease progression had worse Lung Cancer Subscale (LCS) scores (12). Therefore, duration of treatment and the LCS might be useful in determining clinical activity with gefitinib treatment. Because the EGFR is present and important for normal skin homeostasis (13, 14), the biological activity of gefitinib was assessed using markers of PD effects from skin biopsies (e.g., levels of phosphorylated EGFR and activated pMAPK; Ref. 15). These biopsies showed that EGFR phosphorylation was abolished and that activated pMAPK levels were significantly reduced in skin biopsies from patients taking ⱖ150 mg/day gefitinib (Figs. 2A and B, respectively), the lowest dose at which objective tumor responses were noted. These PD analyses indicate that in the skin, gefitinib was exerting maximum biological effect at the lowest dose studied. Table 2 Patients with disease control who received gefitinib for ⱖ6 monthsa,b No. of Time on Gefitinib dose, mg/day patients Response Tumor study, months 150 (n ⫽ 19) 1 1 PRc SD NSCLC NSCLC 17 15 225 (n ⫽ 7) 1 1 1 1 SD SD SD SD SCCHN NSCLC SCCHN HRPC 28⫹d 14 8 7e 300 (n ⫽ 27) 1 1 1 1 SD SD SD SD Ovarian SCCHN NSCLC NSCLC 9f 9 8 6 400 (n ⫽ 27) 1 1 1 1 1 SD SD SD SD SD SCCHN Ovarian CRC CRC NSCLC 14d 7g 6 6 6 600 (n ⫽ 20) 1 1 SD SD NSCLC NSCLC 25⫹d 14d 800 (n ⫽ 20) 1 SD NSCLC 7 1000 (n ⫽ 17) 1 1 SD SD NSCLC HRPC 8d 6h DOSE SELECTION FOR PHASE II AND III CLINICAL TRIALS ⱖ 6 ⫻ 28-day treatment periods. References 8 and 9. PR, partial response; NSCLC, non-small cell lung cancer; SD, stable disease; SCCHN, squamous cell carcinoma of the head and neck; HRPC, hormone-refractory prostate cancer; CRC, colorectal carcinoma. d Includes time spent on extension compassionate-use trial. e Patient had a sustained decrease from baseline prostate-specific antigen ⬎50% over 4 months. f No change in carbohydrate antignen 125 (CA125). g Patient had a 48% reduction in serum CA125. h Worsening in prostate-specific antigen levels observed. The gefitinib Phase I trials were designed and planned for the possibility that results might be unclear, because gefitinib was anticipated to be cytostatic rather than induce tumor regression. However, the blinded-review panel was not required because sufficient patients with objective tumor responses and stable disease were observed across a range of tumors to establish a dose-response curve, supported by PD and PK assessments. The dose:response and dose:toxicity relationships observed are shown in Fig. 3; clinical benefit was not dose related at doses ⱖ150 mg/day, whereas the most common AEs (skin rash and acne) increased with gefitinib dose. These Phase I trial results showed that the OBD for gefitinib is much lower than the MTD, supporting the hypothetical model in Fig. 1B, and they suggested that gefitinib had maximum biological and clinical activity over the dose range 150-1000 mg/day. In addition, PK a b c Table 1 Patients receiving gefitinib by dose and tumor type in two Phase I pharmacology-like dose-escalation trialsa Tumor type b Gefitinib dose, mg/day NSCLC (n ⫽ 61) Ovarian (n ⫽ 25) CRC (n ⫽ 28) HRPC (n ⫽ 17) SCCHN (n ⫽ 26) Total (n ⫽ 157) 150 225 300 400 600 800 1000 13 11 13 8 4 5 7 1 2 4 6 6 2 4 0 4 3 6 3 9 3 0 4 2 2 3 3 3 5 6 5 5 4 1 0 19 27 27 27 20 20 17 a References 8 and 9. NSCLC, non-small cell lung cancer; CRC, colorectal carcinoma; HRPC, hormone-refractory prostate cancer; SCCHN, squamous cell carcinoma of the head and neck. b Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. 4610 Gefitinib: Determining the Optimum Dose for Efficacy dose related, grade 1–2 diarrhea, skin rash, dry skin, pruritus, nausea, acne, vomiting, and elevated liver transaminases. Grade 3– 4 AEs were more frequently observed in patients receiving 500 mg/day than in those given 250 mg/day (Table 3), with the increased incidence accounted for primarily by diarrhea. Furthermore, fewer patients receiving 250 mg/day withdrew (1.5% overall) compared with those given 500 mg/day (4.4%). Consequently, the recommended dose of gefitinib in NSCLC is now 250 mg/day, the dose at which ⬎40% of patients experienced disease control and a favorable tolerability profile was maintained. REACHING THE TARGET: GEFITINIB TISSUE DISTRIBUTION Fig. 2 Graphic display of the immunohistochemical evaluation of paired skin samples taken before (Pre) and during (During) gefitinib therapy. Percentage of keratinocytes with (A) activated epidermal growth factor receptor (EGFR) and (B) phospho-p44/42 mitogen-activated protein kinase (MAPK) levels (15). ⴱ, P ⬍ 0.001. studies indicated that plasma levels of gefitinib over this dose range were sufficient for effective EGFR inhibition. The objective tumor responses observed in patients with NSCLC resulted in two dose levels being selected for Phase II and III NSCLC trials. Although the lowest dose at which objective tumor responses were observed was 150 mg/day, there was potential for individuals receiving this dose to have subtherapeutic exposure as a result of interpatient variability in pharmacokinetics. Accordingly, the slightly higher dose of 250 mg/day was chosen because this dose would ensure adequate gefitinib drug exposure. The second dose chosen was 500 mg/day, which was the highest dose that was well tolerated by most patients on a chronic daily dosing schedule. Both doses were significantly lower than the MTD (approximately onethird and two-thirds of the MTD, respectively), unlike conventional dose selection for chemotherapy agents, which would use the MTD. Evidence to support the extensive tissue distribution of gefitinib has been provided in PK studies involving healthy volunteers and patients with advanced solid tumors, which found that gefitinib (50 –100 mg) had a very high volume of distribution (ⱖ1400 liters; Table 4; Ref. 10). In the Phase I trials, analysis of PD marker levels in the skin also provided evidence that sufficient gefitinib was reaching the skin and inhibiting EGFR signaling (15). Additionally, objective tumor responses observed across a dosage range of 150-1000 mg/day in the Phase I trials indicated that these doses resulted in target inhibition in tumors. These data are supported by preclinical xenograft (LoVo) data showing that, 8 h after the administration of radiolabeled [14C]gefitinib, the tumor:plasma gefitinib ratio was 11:1 (19); radioactivity levels in skin and tumor samples were similar and considerably higher than those in the plasma. Thus, gefitinib targets tumors effectively. DISCUSSION Although the primary objective of a Phase I trial is to assess the safety profile of an anticancer agent, some evidence PHASE II DOSE-EVALUATION TRIALS IN NSCLC Two large, dose-randomized, double-blind, parallel-group, multicenter Phase II trials (‘Iressa’ Dose Evaluation in Advanced Lung Cancer 1 and 2) independently evaluated the activity of 250 and 500 mg/day gefitinib in 425 patients with advanced NSCLC (16, 17). These trials allowed a more detailed evaluation of the doses selected from the Phase I trials and included symptom improvement as an additional end point. There was no difference between the doses for any of the efficacy end points such as objective tumor response rate, disease control rate, time to progression, overall survival, and symptom improvement. Symptom improvement occurred rapidly in both trials (8 –10 days) and was associated with conventional efficacy end points such as objective tumor response rates and overall survival (18). However, fewer and less severe AEs were observed with 250 mg/day than with 500 mg/day in both trials. The most common AEs were manageable, noncumulative, Fig. 3 Dose relationship of disease control (partial response plus stable disease) and skin rash/acne in patients from the Phase I and II (IDEAL) trials (31). Œ, Phase I rash/acne; 䉬, Phase I disease control; large open triangle, Phase II rash/acne; large open diamond, Phase II disease control. Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. Clinical Cancer Research 4611 Table 3 IDEAL 1 and 2 drug-related grade 3– 4 adverse events, disease control, symptom improvement, and survivala IDEAL 1 Drug-related grade 3–4 adverse events (%) Response rate (%) Disease control rate (%) Overall survival (mo) Symptom improvementd (%) Patients with partial response experiencing symptom improvement (%) Improved quality of lifee (%) IDEAL 2 250 mg/day (n ⫽ 103) 500 mg/day (n ⫽ 106) 250 mg/day (n ⫽ 102) 500 mg/day (n ⫽ 114) 8.7b 18.4 54.4 7.6 40.3 69.2 30.2b 19.0 51.4 7.9 37.0 85.7 6.9 11.8 42.2c 7 43 100 17.5 8.8 36.0c 6 35 90 23.9 21.9 34.3f 22.8f a References 16 and 17. Reference 28. c Reference 29. d Assessed using the seven-item Lung Cancer Subscale (LCS) of Functional Assessment of Cancer Therapy-Lung (FACT-L). e Assessed using FACT-L. f Reference 30. b of antitumor activity is required to justify progression to Phase II trials. For the evaluation of biologically targeted agents, conventional clinical end points should be supplemented with surrogate markers of clinical activity, because these agents might not be expected to cause tumor regression or normal tissue toxicity at maximally effective doses. This review has used the example of gefitinib to show that early clinical trials of biologically targeted agents should aim to identify the OBD using clinical end points and one or more PD parameters. NSCLC objective tumor response data from the Phase I and II trials, in which objective responses were observed across a wide dose range (150 –1000 mg/day; Fig. 3), indicate that these doses of gefitinib were sufficient to inhibit EGFR signaling. However, in the absence of an objective response, how do we know that relevant levels of biologically targeted agents are reaching their target tissue? Evidence that gefitinib reaches target tissues and tumors has been supported by the high tumor: plasma ratio observed in xenograft models and by the high volume of distribution of gefitinib (10, 19). Furthermore, PD analyses of biomarker expression have shown that gefitinib at 250 mg/day and 500 mg/day inhibits EGFR-mediated signaling in clinical breast and gastric cancer tumor biopsies (20, 21). The use of surrogate markers has previously been shown to be feasible in selecting the dose for cetuximab (IMC-C225), a humanized anti-EGFR monoclonal antibody; 200 mg/m2 was the lowest dose that saturated the antibody systemic clearance rate and was significantly lower than the MTD (22). In the gefitinib example, when conventional clinical end points were used, doses above a certain threshold did not give better objective tumor responses, whereas AEs were dose-related (Fig. 3). Surrogate markers (including inhibition of EGFR signaling in skin biopsies, duration of treatment, and improvements in disease-related symptoms) were also shown to be feasible for Phase II dose selection. Indeed, the rapid onset of symptom improvement in the Phase II trials along with an observed correlation between symptom improvement and objective tumor response, suggests that symptom improvement may be a rapid surrogate marker of objective tumor response, although additional placebo-controlled studies are needed to clarify this. Although the gefitinib Phase I trials aimed to explore the OBD in an optimal fashion, there were a number of complications that may also apply in early trials of other novel targeted agents. These included the fact that the patient population was heterogeneous, with a variety of EGFR-expressing tumor types. In addition, there is no certainty that each tumor type will be equally sensitive to gefitinib or that the OBD will be identical in all tumors. Such uncertainties meant that two doses (250 and 500 mg/day) were chosen for Phase II/III trials. Finally, much of the PD data came from skin biopsies rather than tumor biopsies, and, because biopsies are not easy to obtain for many tumor types, this is a significant challenge for any approach relying on tumor PD assessments. Furhter refinements in the design of Phase I trials for biologically targeted agents could also be made. One of the complexities of using a blinded-review panel is in the evaluation of TBE based on the relevance of each type of data, because patients will be differently evaluable for specific data of antitumor effects. As such, trials could benefit from cross-validation between experts to obtain a consensus, with focused discussion on discordant cases. If all patients are evaluable for at least one PD parameter (rather than depending on serial biopsies), evidence of TBE could be measured consistently and more Table 4 Intravenous pharmacokinetics of gefitiniba Volume of distribution, liter Mean Range Plasma clearanceb rate, ml/min Mean Range Elimination half-life, h Mean Range a b Healthy volunteers 50–100 mg i.v. (n ⫽ 8) Patients 50 mg i.v. (n ⫽ 19) 1610 1230–2540 1400 830–2710 840 471–1250 514 194–1460 34 23–73 48 10–136 Reference 10. Geometric mean. Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. 4612 Gefitinib: Determining the Optimum Dose for Efficacy accurately; and, if there were more than one PD parameter per patient, the relative merit of that parameter could be prospectively specified (a weighting factor). Potentially, if evidence of a dose response for TBE is further explored in relation to specific tumors (e.g., by increasing patient numbers across the dose range to focus on the most reliable PD measures), a better dose decision for subsequent trials could be determined. One major challenge in designing clinical trials for biologically targeted agents and optimizing their use is how to identify a patient population that is likely to benefit from treatment. In the case of some novel targeted agents, such as trastuzumab, high expression of the target itself is used to select the patients to be treated (23, 24). However, the situation with gefitinib is not so straightforward. Although clinical trials have recruited patients with tumor types known to express EGFR, subsequent retrospective gene expression and immunohistochemical analysis of EGFR expression have shown that tumor EGFR expression levels do not correlate with response to gefitinib (25), although it remains possible that phosphorylated EGFR may be more important (26). Thus, sensitivity to gefitinib is likely to be much more complex and dependent on a number of factors, of which the EGFR may be but one (27). Some studies have investigated genes associated with resistance to gefitinib, and one retrospective analysis found that increased expression of gefitinib resistant gene 1 (GRG1) correlated with a decreased probability of responding to gefitinib (25). Such analyses of molecular factors are being explored in a wide-ranging clinical trial program to explore more fully the potential to identify those patients who will benefit from gefitinib treatment. The clinical trials of gefitinib presented in this review have shown that efficacy and surrogate end points (duration of treatment, improvements in disease-related symptoms, and PD effects) have identified 250 mg/day as the OBD in NSCLC, because higher doses of gefitinib do not give better responses and cause increased toxicity. This recommended dose is onethird of the MTD and results in a favorable benefit:risk ratio. REFERENCES 1. Rowinsky EK. The pursuit of optimal outcomes in cancer therapy in a new age of rationally designed target-based anticancer agents. Drugs 2000;60(Suppl 1):1–14. 2. Fox E, Curt GA, Balis FM. Clinical trial design for target-based therapy. Oncologist 2002;7:401–9. 3. Woodburn JR. The epidermal growth factor receptor and its inhibition in cancer therapy. Pharmacol Ther 1999;82:241–50. 4. Rusch V, Baselga J, Cordon-Cardo C, et al. Differential expression of the epidermal growth factor receptor and its ligands in primary non-small cell lung cancers and adjacent benign lung. Cancer Res 1993;53:2379 – 85. 5. Swaisland H, Laight A, Stafford L, et al. Pharmacokinetics and tolerability of the orally active selective epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 in healthy volunteers. Clin Pharmacokinet 2001;40:297–306. 6. Nakagawa K, Tamura T, Negoro S, et al. Phase I pharmacokinetic trial of the selective oral epidermal growth factor receptor tyrosine kinase inhibitor gefitinib (‘Iressa’, ZD1839) in Japanese patients with solid malignant tumours. Ann Oncol 2003;14:922–30. 7. Ranson M, Hammond LA, Ferry D, et al. ZD1839, a selective oral epidermal growth factor receptor-tyrosine kinase inhibitor, is well tolerated and active in patients with solid, malignant tumors: results of a phase I trial. J Clin Oncol 2002;20:2240 –50. 8. Herbst RS, Maddox AM, Rothenberg ML, et al. Selective oral epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 is generally well-tolerated and has activity in non-small-cell lung cancer and other solid tumors: results of a phase I trial. J Clin Oncol 2002;20: 3815–25. 9. Baselga J, Rischin D, Ranson M, et al. Phase I safety, pharmacokinetic, and pharmacodynamic trial of ZD1839, a selective oral epidermal growth factor receptor tyrosine kinase inhibitor, in patients with five selected solid tumor types. J Clin Oncol 2002;20:4292–302. 10. AstraZeneca, Macclesfield, UK. Data on file. Unpublished data, 2004. 11. Cella DF, Bonomi AE, Lloyd SR, Tulsky DS, Kaplan E, Bonomi P. Reliability and validity of the Functional Assessment of Cancer Therapy-Lung (FACT-L) quality of life instrument. Lung Cancer 1995;12: 199 –220. 12. LoRusso PM, Herbst RS, Rischin D, et al. Improvements in quality of life and disease-related symptoms in phase I trials of the selective oral epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 in non-small cell lung cancer and other solid tumors. Clin Cancer Res 2003;9:2040 – 8. 13. Threadgill DW, Dlugosz AA, Hansen LA, et al. Targeted disruption of mouse EGF receptor: effect of genetic background on mutant phenotype Science (Wash DC) 1995;269:230 – 4. 14. Miettinen PJ, Berger JE, Meneses J, et al. Epithelial immaturity and multiorgan failure in mice lacking epidermal growth factor receptor. Nature (Lond) 1995;376:337– 41. 15. Albanell J, Rojo F, Averbuch S, et al. Pharmacodynamic studies of the epidermal growth factor receptor inhibitor ZD1839 in skin from cancer patients: histopathologic and molecular consequences of receptor inhibition. J Clin Oncol 2002;20:110 –24. 16. Fukuoka M, Yano S, Giaccone G, et al. Multi-institutional randomized phase II trial of gefitinib for previously treated patients with advanced non-small-cell lung cancer. J Clin Oncol 2003;21: 2237– 46. 17. Kris MG, Natale RB, Herbst RS, et al. Efficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer. A randomized trial. JAMA 2003;290:2149 –58. 18. Fukuoka M, Kris M, Giaccone G, et al. Phase II trials of gefitinib (‘Iressa’, ZD1839): rapid and durable objective responses in patients with advanced non-small-cell lung cancer (IDEAL 1 and IDEAL 2). Lung Cancer 2003;41(Suppl 2):S247– 8. 19. McKillop D, Stephens TC, Partridge EA, et al. The distribution of gefitinib (‘Iressa’, ZD1839) into mouse xenograft tumours. Poster A100 presented at the AACR-NCI-EORTC, Boston, MA, USA, November 17–21, 2003. Clin Cancer Res 2003;9(Suppl):6093S 20. Baselga J, Albanell J, Ruiz A, et al. Phase II and tumor pharmacodynamic study of gefitinib (ZD1839) in patients with advanced breast cancer. Proc Am Soc Clin Oncol 2003;22:7. 21. Rojo F, Tabernero J, Van Cutsem E, et al. Pharmacodynamic studies of tumor biopsy specimens from patients with advanced gastric carcinoma undergoing treatment with gefitinib (ZD1839). Proc Am Soc Clin Oncol 2003;22:191. 22. Baselga J, Pfister D, Cooper MR, et al. Phase I studies of antiepidermal growth factor receptor chimeric antibody C225 alone and in combination with cisplatin. J Clin Oncol 2000;18:904 –14. 23. Birner P, Oberhuber G, Stani J, et al. Evaluation of the United States Food and Drug Administration-approved scoring and test system of HER-2 protein expression in breast cancer. Clin Cancer Res 2001;7: 1669 –75. 24. Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2overexpressing metastatic breast cancer. J Clin Oncol 2002;20: 719 –26. Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. Clinical Cancer Research 4613 25. Natale RB, Shak S, Aronson N, et al. Quantitative gene expression in non-small cell lung cancer from paraffin-embedded tissue specimens: predicting response to gefitinib, an EGFR kinase inhibitor. Proc Am Soc Clin Oncol 2003;22:190. 26. Bailey LR, Kris M, Wolf M, et al. Tumor EGFR membrane staining is not clinically relevant for predicting response in patients receiving gefitinib (‘Iressa’, ZD1839) monotherapy for pretreated advanced nonsmall-cell lung cancer: IDEAL 1 and 2. Proc Am Assoc Cancer Res 2003;44(Ed 2):1362. 27. Ciardiello F, Tortora G. Epidermal growth factor receptor (EGFR) as a target in cancer therapy: understanding the role of receptor expression and other molecular determinants that could influence the response to anti-EGFR drugs. Eur J Cancer 2003;39:1348 –54. 28. Forsythe B, Faulkner K. Safety and tolerability of gefitinib (’Iressa’, ZD1839) in advanced NSCLC: overview of clinical experience. Poster P327 presented at the ERS, Vienna, Austria, September 27-October 1, 2003. Eur Respir J 2003;22(Suppl 45):32s. 29. Fukuoka M, Kris M, Giaccone G, et al. Phase II trials of gefitinib (’Iressa’, ZD1839): rapid and durable objective responses in patients with advanced non-small-cell lung cancer (IDEAL 1 and IDEAL 2). Poster presented at the WCLC, Vancouver, Canada, August 10 –14, 2003. Lung Cancer 2003;41(Suppl 2):S247. 30. Natale R, Skarin A, Maddox A, et al. Improvement in symptoms and quality of life for advanced non-small-cell lung cancer patients receiving ZD1839 (’Iressa’) in IDEAL 2. Poster 1167 presented at the ASCO, Orlando, FL, May 18 –21, 2002. Proc Am Soc Clin Oncol 2002;21:292a. 31. Herbst R. Targeting the epidermal growth factor receptor: prognostic and clinical implications. Eur J Cancer Suppl 2003; 1:9 –15. Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research. Development of the Novel Biologically Targeted Anticancer Agent Gefitinib: Determining the Optimum Dose for Clinical Efficacy Michael Wolf, Helen Swaisland and Steven Averbuch Clin Cancer Res 2004;10:4607-4613. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://clincancerres.aacrjournals.org/content/10/14/4607 This article cites 25 articles, 13 of which you can access for free at: http://clincancerres.aacrjournals.org/content/10/14/4607.full.html#ref-list-1 This article has been cited by 16 HighWire-hosted articles. Access the articles at: /content/10/14/4607.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 2004 American Association for Cancer Research.