Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
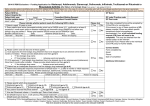
2015/16 PBR Exclusions – Funding Application for Abatacept, Adalimumab, Etanercept, Golimumab, Infliximab, Tocilizumab or Rituximab for Rheumatoid Arthritis after failure of a biologic drug (Final version 2: last updated 01/07/15) Before providing patient identifiable data on this form, please confirm that the patient (or in the case of a minor or vulnerable adult with the parent/legal guardian/carer) has given appropriate explicit consent for sensitive personal information on this form to be passed to the CCG and/or CSU for processing this funding request and validating subsequent invoices. Consent given: Patient NHS No: Patient Hospital No: Patient birth year: Confirm patient status: (yyyy) NHS Private Overseas Trust: GP Name: Consultant Making Request: Consultant Contact Details: GP code /Practice code: GP Post code: Yes (select 1 option) Please indicate whether patient meets the following NICE criteria 1. Patient is aged 18 years or over 2. Does patient have active rheumatoid arthritis which had a DAS28 score >5.1, confirmed on at least 2 occasions 1 month apart while on disease modifying anti-rheumatic drugs (DMARD) but before any biologic drug was started ? Please give baseline DAS28 scores and list DMARDs used. Baseline DAS28 Score 1 Date: Baseline DAS28 Score 2 Date: Start date Stop date DMARD treatment line biologic treatment Start date Stop date DAS28 at start date DAS28 at stop date Stop date Treatment No DAS28 at start date DAS28 at stop date Yes No Only fully completed forms will be accepted by CCGs/CSUs for consideration. If the answer to any of these questions is NO, please consider if there are patient specific exceptional clinical circumstances demonstrated. If so, a full individual funding request (IFR) form will need to be completed. This may be obtained from the named contact at the relevant CCG/CSU/Trust. Please refer to the individual CCG IFR policy for further details. Contact details: Form completed by: Email: Phone: Date of completion: Additional Information: Yes No Adverse event and severity 5. Patient had inadequate response (improvement of DAS28 score < 1.2) after 6 months or initial response and subsequent inadequate response to either Abatacept, Adalimumab, Certolizumab, Etanercept, Golimumab, Infliximab or Tocilizumab. Please provide biologic drug history below: Start date Yes Reason for stopping 3. Please confirm and tick that one of these applies: CCG approved 2nd line biologic drug treatment has to be stopped due to an adverse event within 6 months of initiation. Please provide details below: 1st line biologic drug name: 2nd line biologic drug name: ; Adverse event and severity: (go to 6) Patient was responding to CCG approved 1st line biologic treatment but this had to be stopped due to an adverse event (intolerance) more than 6 months after initiation (go to 4) Patient has an inadequate response to first line biologic drug treatment (go to 5) 4. Was there an improvement in DAS28 score by >1.2 compared to baseline while on 1st line biologic treatment? Please provide details below, then go to 6. 1st Please tick Yes No Yes No Reason for stopping Participating CCGs: Barking&Dagenham; Barnet; Brent; Camden; Central London; City and Hackney; Croydon; Ealing; Enfield; Hammersmith&Fulham; Haringey; Harrow; Havering; Hillingdon; Hounslow; Islington; Kingston; Merton, Newham; Redbridge; Richmond; Sutton; Tower Hamlets; Waltham Forest; Wandsworth; West London. This form should be returned to the named contact at the relevant CCG/CSU Page 1 of 5 6. Please specify which drug is requested? Abatacept sc (go to 12) Abatacept iv (go to 12) Golimumab (go to 11) Rituximab (go to 7) Remsima® (infliximab biosimilar)* Adalimumab (go to 12) Tocilizumab sc (go to 10) Inflectra® (infliximab biosimilar)* *Remsima® is the preferred Infliximab brand for all London Trusts. Please provide valid reason, if not using preferred biosimilar. 7. Has patient received Rituximab before? No (go to 13) Yes (go to 8) Etanercept (go to 12) Tocilizumab iv (go to 10) Remicade® (then go to 12) 8. Was last Rituximab infusion > 6 months ago? Date of last infusion: 9. Did DAS28 improve by ≥1.2 with previous Rituximab treatment? (provide scores) (go to 13) DAS28 score pre-rituximab: DAS28 after 2 Rituximab doses: 10. For Tocilizumab, the manufacturer will provide tocilizumab at the discount agreed by NICE as part of the patient access scheme? (go to 12) Note: Full list price will not be reimbursed 11. For Golimumab , the manufacturer will provide the 100mg dose at the same cost as the 50mg. 12. Patient cannot receive rituximab because of adverse reaction or has a contraindication to Rituximab and/or Methotrexate (please tick): Rituximab. Please give details: OR Methotrexate (NICE supports monotherapy with adalimumab or etanercept only). Please give details: 13. Is Abatacept / Adalimumab/ Etanercept/ Golimumab / Infliximab / Rituximab / Tocilizumab to be used with Methotrexate? 14. Does patient have residual disease activity (i.e. DAS28 score≥ 2.6)? Please provide current DAS28 Score: Date: 15. Treatment will be initiated, supervised and treatment response assessed by specialist physicians experienced in the diagnosis and treatment of rheumatoid arthritis? 16. What is the acquisition cost of the drug (including VAT if applicable)? Abatacept, Adalimumab, Etanercept, Golimumab, Infliximab, Tocilizumab: Rituximab: Funding approved for first 6 months Funding reapproved? (12 monthly intervals) Funding approved (max. TWO 1000mg infusions 2 weeks apart). Yes No Yes No Yes No £ Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Patient weight (if used for drug dosing): kg Drug dose + frequency: Please note: CCGs only fund licensed doses. Do not exceed licensed dose or frequency. /month FOR CCG/CSU USE ONLY Funding will only be re-approved if there is an adequate response at 6 months i.e. improvement in DAS28 score of ≥ 1.2 in the absence of severe drug related toxicity. After initial response DAS28 should be monitored at least every 6 months and treatment withdrawn if improvement is not maintained. Complete new application if alternative biologic drug has to be used due to adverse event before initial 6 month efficacy assessment of CCG approved 2nd line biologic drug. Treatment with rituximab plus methotrexate should be continued only if there is an adequate response following initiation of therapy. An adequate response is defined as an improvement in disease activity score (DAS28) ≥ 1.2. Trusts may apply for repeat courses of treatment with rituximab plus methotrexate by completing another application no more frequently than every 6 months. Page 2 of 5 Adalimumab, etanercept, infliximab rituximab and abatacept for the treatment of Rheumatoid Arthritis after the failure of a TNF inhibitor (NICE TA 195: Aug 2010) 1.1 Rituximab in combination with methotrexate is recommended as an option for the treatment of adults with severe active rheumatoid arthritis who have had an inadequate response to, or are intolerant of, other disease-modifying anti-rheumatic drugs (DMARDs), including at least one tumour necrosis factor (TNF) inhibitor. Treatment with rituximab should be given no more frequently than every 6 months. 1.2 Treatment with rituximab in combination with methotrexate should be continued only if there is an adequate response following initiation of therapy and if an adequate response is maintained following retreatment with a dosing interval of at least 6 months. An adequate response is defined as an improvement in disease activity score (DAS28) of 1.2 points or more. 1.3 Adalimumab, etanercept, infliximab and abatacept, each in combination with methotrexate, are recommended as treatment options only for adults with severe active rheumatoid arthritis who have had an inadequate response to, or have an intolerance of, other DMARDs, including at least one TNF inhibitor, and who cannot receive rituximab therapy because they have a contraindication to rituximab, or when rituximab is withdrawn because of an adverse event. 1.4 Adalimumab monotherapy and etanercept monotherapy are recommended as treatment options for adults with severe active rheumatoid arthritis who have had an inadequate response to, or have an intolerance of, other DMARDs, including at least one TNF inhibitor, and who cannot receive rituximab therapy because they have a contraindication to methotrexate, or when methotrexate is withdrawn because of an adverse event. 1.5 Treatment with adalimumab, etanercept, infliximab and abatacept should be continued only if there is an adequate response (as defined in 1.2) 6 months after initiation of therapy. Treatment should be monitored, with assessment of DAS28, at least every 6 months and continued only if an adequate response is maintained. 1.6 When using DAS28, healthcare professionals should take into account any physical, sensory or learning disabilities, communication difficulties, or disease characteristics that could adversely affect patient assessment and make any adjustments they consider appropriate. 1.7 A team experienced in the diagnosis and treatment of rheumatoid arthritis and working under the supervision of a rheumatologist should initiate, supervise and assess response to treatment with rituximab, adalimumab, etanercept, infliximab or abatacept. Disease severity 2.10 …”A DAS28 score greater than 5.1 indicates high disease activity, between 3.2 and 5.1 moderate disease activity, and less than 3.2 low disease activity. A score less than 2.6 indicates disease remission. An improvement in DAS28 score of 0.6 or less is considered a poor response, and improvements greater than 1.2 points indicate a good response. The European League Against Rheumatism (EULAR) response criteria are based on the DAS measure. …”. Golimumab for the treatment of rheumatoid arthritis after the failure of previous disease-modifying anti-rheumatic drugs (NICE TA 225: June 2011) 1.1 Golimumab in combination with methotrexate is recommended as an option for the treatment of rheumatoid arthritis in adults whose rheumatoid arthritis has responded inadequately to conventional disease-modifying anti-rheumatic drugs (DMARDs) only, including methotrexate, if: it is used as described for other tumour necrosis factor (TNF) inhibitor treatments in ‘Adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis’ (NICE technology appraisal guidance 130), and the manufacturer provides the 100 mg dose of golimumab at the same cost as the 50 mg dose, agreed as part of the patient access scheme. 1.2 Golimumab in combination with methotrexate is recommended as an option for the treatment of rheumatoid arthritis in adults whose rheumatoid arthritis has responded inadequately to other DMARDs, including a TNF inhibitor, if: it is used as described for other TNF inhibitor treatments in ‘Adalimumab, etanercept, infliximab, rituximab and abatacept for the treatment of rheumatoid arthritis after the failure of a TNF inhibitor’ (NICE technology appraisal guidance 195), and the manufacturer provides the 100 mg dose of golimumab at the same cost as the 50 mg dose, agreed as part of the patient access scheme. 1.3 When using the disease activity score (DAS28), healthcare professionals should take into account any physical, sensory or learning disabilities, communication difficulties, or disease characteristics that could adversely affect patient assessment and make any adjustments they consider appropriate. Page 3 of 5 Tocilizumab for the treatment of rheumatoid arthritis (NICE TA 247: Feb 2012; this replaces NICE TA 198) 1.1 Tocilizumab in combination with methotrexate is recommended as an option for the treatment of rheumatoid arthritis in adults if: the disease has responded inadequately to disease-modifying anti-rheumatic drugs (DMARDs) and it is used as described for tumour necrosis factor (TNF) inhibitor treatments in Adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis (NICE technology appraisal guidance 130), specifically the recommendations on disease activity and choice of treatment or the disease has responded inadequately to DMARDs and a TNF inhibitor and the person cannot receive rituximab because of a contraindication to rituximab, or because rituximab is withdrawn because of an adverse event, and tocilizumab is used as described for TNF inhibitor treatments in Adalimumab, Etanercept, infliximab, rituximab and abatacept for the treatment of rheumatoid arthritis after the failure of a TNF inhibitor (NICE technology appraisal guidance 195), specifically the recommendations on disease activity or the disease has responded inadequately to one or more TNF inhibitor treatments and to rituximab and the manufacturer provides tocilizumab with the discount agreed as part of the patient access scheme. 1.2 People currently receiving tocilizumab for the treatment of rheumatoid arthritis who do not meet the criteria in 1.1 should have the option to continue treatment until they and their clinicians consider it appropriate to stop. Summary of Product Characteristics- Rituximab (Mabthera ®) (ref: http://www.medicines.org.uk, accessed 05/03/2015, last updated on the eMC: 06/06/2014) A course of MabThera consists of two 1000 mg intravenous infusions. The recommended dosage of MabThera is 1000 mg by intravenous infusion followed by a second 1000 mg intravenous infusion two weeks later. The need for further courses should be evaluated 24 weeks following the previous course. Retreatment should be given at that time if residual disease activity remains, otherwise retreatment should be delayed until disease activity returns. Available data suggest that clinical response is usually achieved within 16 - 24 weeks of an initial treatment course. Continued therapy should be carefully reconsidered in patients who show no evidence of therapeutic benefit within this time period. Page 4 of 5 NICE Rheumatoid arthritis commissioning algorithm (August 2013) (Ref: http://www.nice.org.uk/proxy/?sourceUrl=http%3a%2f%2fwww.nice.org.uk%2fmedia%2f730%2f6B%2fRheumatoidArthritisCommissioningAlgorithm.pdf) Page 5 of 5