Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
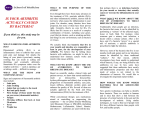
SEPTIC ARTHRITIS ALLISON I. MARTIN, BSN, RN DIAGNOSIS • Septic arthritis is an infection in the joint cavity most often caused by bacteria, but also can be caused by fungi or mycobacteria • Nongonococcal bacteria can lead to irreversible joint damage • Gonococcal bacteria is far less destructive to joints • Acute monoarticular arthritis • Infectious and inflammatory MECHANISM OF INFECTION • Hematogenous spread • Bacteremia • IV drug abuse • Immunocompromised state (Diabetes, HIV) • Direct inoculation • • • • Recent joint surgery Prosthetic joint Steroid injections Trauma • Spread from local infection • • • • Skin infection or ulcer Osteomyelitis Septic bursitis Abscess http://www.physio-pedia.com/Septic_(Infectious)_Arthritis PATHOGENESIS • The synovial fluid within the joint cavity is normally sterile • Synovial tissue has no limiting basement plate so bacteria quickly gain access • Most common causative agents: • Staphylococcus aureus • Streptococcus species • Gram-negative bacilli in immunocompromised and IV drug abusers • Bacteria cause an acute inflammatory cell response in the synovial membrane with purulent effusion into the joint capsule • Following onset, there is a marked hyperplasia of the lining cells in the synovial membrane within 7 days • Inflammatory cells release cytokines and proteases that cause cartilage degradation and inhibit cartilage synthesis leading to rapid destruction of the joint RISK FACTORS • • • • • • • • Advanced age (50% of patients are > 60 years) Diabetes mellitus Rheumatoid arthritis Presence of prosthetic joint Recent joint surgery Skin infection Intravenous drug use, alcoholism Prior intraarticular corticosteroid injection CLINICAL MANIFESTATIONS • History • Presentation • Monoarticular acute joint swelling, pain, erythema, warmth, joint immobility; ROM is significantly restricted and very painful • Infection in the knee is most common (> 50% of cases), but the hip, shoulder, ankle, elbow, and wrist can also be affected • HPI – OLDCARTS • Onset, location, associated symptoms, risk factors, concurrent illness • Ask about injury or trauma, recent infections of skin or urinary tract • Abrupt onset with fever and chills points to infectious cause • History of skin lesions, vaginal or urethral discharge, exposure to gonorrhea, tick bites or exposure to ticks CLINICAL MANIFESTATIONS • ROS: • General: fever and chills (common but are absent in up to 20% of cases), fatigue • HEENT: drainage, mucosal ulcers, petechiae in eyes or mouth • Cardiovascular: chest pain, syncope • Respiratory: cough, shortness of breath, dyspnea • GU: urinary symptoms, hematuria, discharge • GI: bowel changes, N/V • Skin: skin wound, lesion, ulcers, bites, petechiae • Musculoskeletal: swelling, erythema, warmth, joint stiffness and immobility (mono-, oligo- or polyarticular) CLINICAL MANIFESTATIONS • PMH: Diabetes mellitus, rheumatoid arthritis, gout or pseudogout, prosthetic joint, osteoarthritis, prior intraarticular corticosteroid injections, immunosuppression, HIV infection, previous trauma • PSH: Recent joint surgery (within 24 months), dental procedures • Social history: IV drug abuse, alcoholism, sexual history and STDs (gonococcal arthritis) • Medications: Immunosuppressive therapy, steroids, chemotherapy PHYSICAL EXAMINATION • Vitals: Note temperature • Most patients with septic arthritis are febrile with high fever • Patients with gout and rheumatoid arthritis may have low-grade fever • HEENT: Examine eyes for conjunctivitis and iritis, fundi for signs of endocarditis, mouth for mucosal ulcers • Cardiovascular: Auscultate for murmur • Respiratory: Auscultate lungs • Integumentary: Lesions, wounds, ulcers, track marks, tophi • Genitalia: Check for signs of gonococcal urethritis and cervicitis • Musculoskeletal: Examine all joints; assess involved joint for increased warmth, swelling, redness, effusion, and immobility; test active and passive ROM • Differentiate inflammation of the joint space versus periarticular process (tendons, bursa, or skin) which may have preserved ROM despite pain • Check spine ROM, restriction and tenderness can indicate spondylitis DIAGNOSTIC TESTS • Synovial fluid aspiration is the definitive diagnostic test • Gram stain: gram positive bacteria in about 80% of cases • Culture: positive in 90% of cases with nongonococcal arthritis • Leukocyte count with differential: exceeds 50,000/mcL and often > 100,000/mcL • Crystal analysis Blood cultures should be obtained (positive in 50% of patients) CBC: elevated WBCs, common, but not specific C-reactive protein: 92% sensitive, not specific Erythrocyte sedimentation rate: 98% sensitive, not specific Radiographs obtained for baseline image, detect fracture, or underlying inflammatory arthritis • MRI to detect effusions and inflammation in joints that are difficult to examine, including the hip and sacroiliac joints • Ultrasound more sensitive for effusions of the hip • • • • • CATEGORIES OF SYNOVIAL FLUID BASED UPON CLINICAL AND LAB FINDINGS Measure Normal Noninflammatory Inflammatory Septic Volume, mL (knee) < 3.5 Often > 3.5 Often > 3.5 Often > 3.5 Clarity Transparent Translucent Translucentopaque Opaque Color Clear Yellow Yellow to opalescent Yellow to green, frank pus Viscosity High High Low Variable WBC, per mm3 < 200 0 to 2000 2000 to 100,000 15,000 to > 100,000 PMNs (%) < 25 < 25 >= 50 >= 75 Culture Negative Negative Negative Positive Adapted from https://www.uptodate.com/contents/septic-arthritis-in-adults DIFFERENTIAL DIAGNOSIS • Inflammatory • Crystal-induced arthritis: • Gout: uric acid crystals • Pseudogout: calcium pyrophosphate crystals • Rheumatoid arthritis • Reactive arthritis • Infectious • Lyme disease • Disseminated Gonorrhea • Non-inflammatory • Hemarthrosis • Red flags • Septic arthritis • Emergency • Immediate hospital admission required • Significant joint destruction and other complications, including amputation, sepsis, and death • Osteomyelitis • Avascular necrosis TREATMENT • Treatment includes immediate hospitalization for antibiotics and joint drainage • Early consult with orthopedics, rheumatology, and infectious disease • Synovial fluid aspiration analysis, start empirical antibiotics according to gram stain, then tailor antibiotics to culture results • Antibiotic therapy • Gram positive cocci: • Vancomycin (also 1st line for MRSA) • Daptomycin, linezolid, and clindamycin are alternatives • Gram negative bacilli: third-generation cephalosporin • Ceftriaxone, cefotaxime, ceftazidime • Pseudomonas aeruginosa (IV drug abusers) • Ceftazidime and gentamicin • Cephalosporin-allergic patients • Ciprofloxacin and aminoglycoside TREATMENT • Duration of therapy • Parenteral antibiotics for at least 14 days followed by oral therapy for an additional 14 days • Parenteral antibiotics for 4-7 days followed by 14-21 days of oral therapy • Three to four weeks of IV therapy may be needed for arthritis caused by P. aeruginosa, Enterobacter spp., S. aureus, or in the setting of bacteremia • Joint drainage • Needle aspiration (arthrocentesis) • Arthroscopic drainage • Arthrotomy (open surgical drainage) • Immobilization, elevation, ice packs • Postpone anti-inflammatory medications for 12-24 hours; can use analgesics without anti-inflammatories if pain is severe • Early active range of motion as tolerated will speed recovery TREATMENT • Needle aspiration • Knee, perform until culture negative • If not adequate for joint decompression after 3-5 days, then surgical drainage is required • Arthroscopy • Provides easy irrigation and better visualization • Knee, shoulder, wrist • Surgical drainage • Hips, shoulders, and prosthetic joint infections • Any joint not improving after serial needle aspiration or if needle drainage is inadequate http://jama.jamanetwork.com/article.aspx?articleid=206414 OUTCOMES • Prognosis dependent on prior health of the patient, the causative organism, and promptness of treatment • S. aureus is associated with poor functional outcome in 46-50% of cases • Overall mortality rates range from 10 -15% • Mortality rate increases to 30% for patients with polyarticular sepsis • Morality is 50% if infection due to S. aureus or occurs in the presence of RA • Morbidity occurs in one-third of patients with bacterial arthritis • Amputation, arthrodesis, prosthetic surgery, severe functional deterioration • Failure to initiate appropriate antibiotic therapy within 24 to 48 hours of onset can cause subchondral bone loss and permanent irreversible joint damage and dysfunction • Prompt identification and referral for treatment are imperative SUMMARY https://www.uptodate.com/contents/septic-arthritis-in-adults REFERENCES Evaluation of acute monoarticular arthritis (2014). In A. H. Goroll & A. G. Mulley (Ed.), Primary care medicine: Office evaluation and management of the adult patient (7th ed.). Philadelphia: Lippincott Williams & Wilkins. Goldenberg, D. L., & Sexton, D. J. (2016). Septic arthritis in adults. In Calderwood, S. B. (Ed.), UpToDate. Retrieved from https://www.uptodate.com/contents/septic-arthritis-in-adults Hellman, D. B., & Imboden, J. B. (2015). Nongocococcal acute bacterial (septic) arthritis. In M. A. Papadakis, S. J. McPhee, & M. W. Rabow (Eds.). Current medical diagnosis & treatment (54th ed., pp. 849-851). New York: McGraw-Hill Horowitz, D. L., Katzap, E., Horowitz, S., & Barilla-LaBarca, M. (2011). Approach to septic arthritis. American Family Physician. 84(6), 653-660. Retrieved from http://www.aafp.org/afp/2011/0915/p653.html Omar, M., Ettinger, M., Reichling, M., Petri, M., Lichtinghagen, R., Guenther, D.,…Krettek, C. (2014). Preliminary results of a new test for rapid diagnosis of septic arthritis with use of leukocyte esterase and glucose reagent strips. The Journal of Bone and Joint Surgery. American Volume, 96(24), 2032-2037. doi:10.2106/JBJS.N.00173 QUESTIONS? http://www.aafp.org/afp/2011/0915/p653.html