Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
THE
ANATOMY
CORACOHUMERAL
OF
A SUBSTANTIAL
J. G.
From
Poriya
We dissected
structure
From
the
time
of
Government
60 shoulders
in clinical
Bankart
BUT
EDELSON,
C.
Hospital,
Tiberias,
to demonstrate
problems
LIGAMENT
the
area
of
SchoolofMedicine,
Tel Aviv
of the coracohumeral
ligament.
MATERIALS
Both
The role of this
shoulders
placed
superior
structure
particularly
in problems
AND
of 10 cadavers
METHODS
were
examined
within
24
hours of death.
Another
40 shoulders
were examined
in
bodies
preserved
for dissection
at the Sackler
Medical
School
of Tel Aviv
University,
Israel.
The age range
at
death
varied
from three
to 74 years.
In addition
to gross
anatomical
observations,
sections
of the coracohumera!
ligament,
partner.
strategically
appreciated,
GRISHKAN
greatest
have
recently
emphasised
the intricate
and
relationship
of the
inferior
glenohumeral
to the coracohumeral
ligament,
which
forms
a
substantial
superior
The role ofthis
is becoming
better
STRUCTURE
is discussed.
interest
as regards
problems
of shoulder
stability
has
been the inferior
capsule
and the inferior
g!enohumeral
ligament
(Perkins
1953 ; Moseley
and Overgaard
1962;
Protzman
1980; Turke!
et a! 1981).
However,
Gagey
et
a! (1987)
necessary
ligament
A.
and Sack/er
the anatomy
of the shoulder
(1938)
TAITZ,
NEGLECTED
capsule
nation.
the coraco-acromial
ligament,
were harvested
These
specimens
and
sent
were
and
the shoulder
for histological
fixed
in 10%
examineutral
of inferior
(Basmajian
and Bazant
1959;
Ovesen
and
Nielsen
1985)and
mu!tidirectional
instability
(Nobuhara
and Ikeda
1987; He!mig
et a! 1988), but also in posterior
(Ovesen
and S#{248}jbjerg 1986),
recurrent
anterior
(Rowe
and Zarins
1981) and even
bicipital
instabilities
(Sl#{228}tis
buffered
formalin,
sectioned
in paraffin
and stained
with
haematoxylin-eosin
and Masson’s
trichrome.
Exposure.
The coracohumera!
ligament
is surrounded
and
bursa)
mera!
Aa!to
1979; BjOrkenheim
et a! 1988).
However,
many
orthopaedic
surgeons
sider
the role ofthe
do not
see
coracohumera!
it. As Rowe
and
do
ligament
Zarins
not
con-
because
point
out
they
(1981),
and obscured
by fatty fibrous
tissue
and bursae
(above
is the subacromia!
bursa
and below
is the subcoracoid
which
ligament
ligament
this
area is not easily
visualised
in the standard
approaches
to the shoulder.
Nor does arthroscopic
examination
help,
since the coracohumera!
ligament
is extra-articular.
This paper
aims
to demonstrate
the structure
and
relations
of the coracohumera!
ligament
and to discuss
its clinical
relevance.
gain
; this
exposure.
we teased
is closely
also
was
It was
away or excised.
The coracohuoverlaid
by the coraco-acromia!
removed
then
possible
or partially
detached
in fresh
specimens
demonstrate
the coracohumeral
ligament
by traction
the arm or through
sutures
placed
in the rotator
cuff,
we usually
divided
the acromion
and lateral
clavicle
order
to gain
it
full exposure
(Figs
to
to
on
but
in
1 to 5).
FINDINGS
J. G. Edelson,
MD, FAAOS,
A. Grishkan,
MD, Pathologist
Poriya
Government
Hospital,
C. Taitz,
Department
Medicine,
Tiberias,
Israel.
Tel
of Anatomy
Aviv,
Israel.
should
DN Emek
and
be sent
HaYarden
Anthropology,
to
Dr J.
15130,
1991 British
Editorial
Society
ofBone
030l-620X/91/10l2
$2.00
JBoneJoint
Surg[Br]
1991 ; 73-B:l50-3.
150
Surgery
MSc
Correspondence
Degania
Bet,
©
ChiefofOrthopaedic
Sackler
G. Edelson
Israel.
and
Joint
School
at do
Surgery
Kibbutz
of
The coracohumeral
‘ligament’
is not a true ligament.
On
gross examination
it has no superficial
sheen nor the taut
feel of a true bone-to-bone
structure
such as the coracoacromia!
ligament
which
overlies
it. On microscopic
examination
we confirmed
the findings
of Hollinshead
(1982),
that the coracohumeral
ligament
is part of the
capsule
of the shoulder
with the typical
layered
pattern
of sheets
and bundles
of collagenous
tissue
interspersed
with
strands
of loose
connective
tissue
and
vascular
channels
(Fig. 6a). This is characteristic
of the shoulder
THE
JOURNAL
OF BONE
AND
JOINT
SURGERY
THE
CORACOHUMERAL
LIGAMENT
151
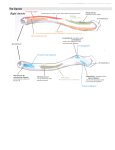
Dissection
superior
to show
and diagram
of anteroviews of the right shoulder
the
rc1ationship
of the
coracohumeral
ligament
to the rotator
cuff.
The
acromion,
distal
clavicle,
coraco-acromial
ligament
and
conjoint
tendon
have
been
removed.
C, coracohumeral
ligament ; c, coracoid
process
; s, supraspinatus;
55, subscapularis;
b, biceps
tendon ; g, glenoid
; o, rotator
interval between
subscapularis
and supraspinatus.
Figure
3 - The left shoulder
of a 40-year-old
man. The acromion
and distal
clavicle
have been osteotomised
and the coraco-acromial
ligament
has
been turned
back.
Figure
4 - The left shoulder
of a 24-year-old
man. This was the least robust
of the coracohumeral
ligaments
found
in our study.
Figure
5 - Same specimen
as Figure
3 with the bicipital
tendon
exposed
by an incision
in the overlying
coracohumeral
ligament.
C, coracohumeral
ligament
; b, biceps
tendon
; ca, coraco-acromial
ligament
; c, coracoid
; s, supraspinatus
; ss, subscapularis.
‘
.
1
.
.j
-
.
..
. ..
-
-
:
...
_UaJ:_f.
!&j
‘
.-.--#{149}
.
‘,
----.
.4
__w-_’
.
;
‘-
..
-.-
-.
:
.-
.-
a
-
-.
.c_
---,-
#{176}.
.;
::
Fig.
Figure
6a
interspersed
of the same
fibroblastic
VOL.
-
6a
Section
of the coracohumeral
with loose connective
tissue
patient.
There
are relatively
cells of true ligaments.
(Both
73-B, No. 1, JANUARY
1991
.i
r\
Fig.
6b
‘ligament’,
showing
the typical
appearance
ofjoint
capsule.
Layered
bundles
of collagenous
and vascular
channels;
note the size and shape
of the nuclei.
Figure
6b - The coraco-acromial
acellular
parallel
bundles
of connective
tissue ; the flattened
and elongated
nuclei
are characteristic
stained
with haematoxylin
and eosin,
x 200.)
tissues
are
ligament
of the
152
J. G. EDELSON,
capsule
Specimens
a quite
(Schwartz
ofthe
et a! 1989)
coraco-acromial
different
pattern
and that
ligament
characteristic
C. TAITZ,
of other
joints.
demonstrated
of a true
ligamen-
A. GRISHKAN
from
trochanter
similar
ligament
to the
bridges
to trochanter
across
the
femur;
this
is
manner
in which
the coracohumeral
the tuberosities
of the humerus.
structure
(Fig. 6b).
The coracohumeral
ligament
is a substantial,
somewhat trapezoidal
structure,
arising
from the lateral
aspect
of the coracoid
process
from its root to about
1 cm from
The i!iofemora!
part
by the reflected
analogous
structure
the biceps.
Indeed,
its tip (Figs
1 and 2). The ligament
then
top of the shoulder,
joining
the capsule,
into the humerus
at the greater
and lesser
either
side of and over the bicipital
groove
The coracohumeral
ligament
begins
the capsule
of the shoulder
at the base
evolution,
the biceps
tendon
is extra-articular
like the
rectus
femoris.
DePalma
(1983)
confirms
this, showing
photographs
of specimens
in which
the biceps
tendon
lies over the capsule,
outside
the joint.
The long head of
tous
but
the
is then lifted
forward-jutting
result,
the
away
from it more
distally
because
of
shape
of the coracoid
process.
As a
ligament
edge (Figs
considerable
passes
over the
and is inserted
tuberosities,
on
(see Fig. 5).
to blend
with
of the coracoid,
forms
a bridge-like
anterior
3 and 4) over the ‘rotator
interval’,
gap
between
the subscapularis
leading
that
and
is, the
the
supraspinatus
parts of the rotator
cuff(see
Fig. 2).
In agreement
with Hollinshead
(1982) we found
the coracohumera!
ligament
is “the most important
most
constant
thickening
shoulder”.
It was present
there
was
individual
of the
fibrous
capsule
that
and
of the
in a!! specimens
at a!! ages,
variation
in its breadth
but
and
thickness.
The least robust
of the ligaments
in relation
to
the other
structures
of the shoulder
was found
in a 24year-old
accident
victim
(Fig. 4), but even in this case
the
ligament
was
a substantial
and
clearly
defined
structure.
There
was no great
variation
between
the left
and
right sides in individual
When
the 20 fresh
through
a
ligament
also in the
the body.
cadavers.
shoulder
specimens
were
put
clinical
range ofmovement,
the coracohumeral
was taut in flexion
and external
rotation,
and
anatomical
‘suspended’
position
at the side of
Similarly,
the ligament
tightened
with attempts
the biceps
tendon
the coracohumeral
before
its
ligament
is overlaid
in its Y-shaped
head
of the rectus
femoris.
The
in the shoulder
is the long head
of
Testut
(1932)
points
out that,
in its
seems to have ‘dropped
ligament
to become
attachment
to the
sometimes
stand.
Similarly,
of the shoulder.
rotator
though
meral
interval
when
they do not
ligament
(Neer
The
coracohumeral
and
the
inferior
mobility
et a! 1989) or
1985). However,
DISCUSSION
this
glenohumeral
ligament,
hara
and
Ikeda
(1987)
report
101 cases
of shoulder
instability
in which
good results
were obtained
by closing
the ‘rotator
interval’
and reinforcing
this repair
with the
coracohumera!
ligament.
Other
surgeons
have
also
reported
closing
any areas
of capsular
weakness
in the
repairing
shoulder
instability,
even
specifically
mention
the coracohuand Foster
1980; Rowe
and Zarins
to regain
abduction
the coracohumeral
by virtue
of its strength
and its strategic
position,
is a
central
element
in the suspension
of the humerus.
Although
not
fully
appreciated
at present
and
difficult
to approach,
the coracohumera!
ligament
may
well become
relevant
to clinical
practice.
Indeed,
Nobu-
rotation
coronal
whereas
humeral
ligament.
It is accepted
that
the iliofemora!
ligament
is “one of the strongest
in the body”
(Hollinshead 1982);
it is the passive
stabiliser
against
which
we
1981 ; Cofield,
Kavanagh
The coracohumeral!igament
in pure
glenoid,
the reflected
head ofthe
rectus
femoris
remains
extracapsular in its course
to the superior
rim of the acetabulum.
Such parallels
are not exact,
but are useful in drawing
attention
to the strength
and importance
of the coraco-
at anterior
or posterior
translation
of the humera!
head
in the sagittal
plane.
It tended
to become
slack in media!
and
superior
down’
through
intra-capsular
and
Frassica
may
in reconstructive
in recalcitrant
it is possible
key suspensory
ligament
1985).
need to be released
operations
(F!atow
frozen
shoulders
that too vigorous
might
lead
(Leffert
release
of
to instability.
liga-
ments
have been compared
to the cruciate
ligaments
of
the knee in regard
to the intricate
and co-ordinated
way
in which
they guide and stabilise
movements
of the joint
(Gagey
et a! 1987). We suggest
that a more appropriate
analogy
is with the capsular
ligaments
of the hip and that
the coracohumera!
ligament
corresponds
to the iliofemoral
ligament.
Like
the coracohumeral
ligament,
the
iliofemora!
ligament
is not a typical
ligament
but rather
No benefits
commercial
article.
a strong
superficial
layer of the capsule
deeper
layer of capsular
fibres which
are
orientation
(Hollinshead
1982). Like the
ligament
the iliofemoral
ligament
has
shape.
It arises
from
the inferior
iliac
analogous
in the pelvis
to the coracoid
The i!iofemoral
ligament
passes
down
Basmajlan
running
over a
more circular
in
coracohumeral
a trapezoidal
spine,
which
is
in the shoulder.
to its insertion
in any
party
form have been
related
directly
received
or will be received
or indirectly
to the subject
from a
of this
REFERENCES
Bankart
ASB.
Pathology
shoulder-joint.
BrJSurg
and
treatment
1938; 26:23-9.
of
recurrent
dislocation
of
JV, Bazant
FJ. Factors
preventing
downward
dislocation
of
the adducted
shoulder
joint : an electromyographic
and morphological
study.
J Bone Joint Surg [Am]
1959; 41-A :1182-6.
Bj#{246}rkenhelm JM, Paavolainen
P, Ahovuo
J,
the rotator
cuff and surrounding
tissues.
results.
C/in Orthop
1988; 236:148-53.
Cofield
RH, Kavanagh
BF,
In : Instructiona/
Course
Co. 1985; 34 :210-27.
THE
Frassica
Lectures,
JOURNAL
Sl#{228}tis
P. Surgical
Factors
repair of
influencing
the
FJ. Anterior
shoulder
instability.
AAOS.
St. Louis,
etc : CV Mosby
OF BONE
AND
JOINT
SURGERY
THE
DePahna
AF.
Lippincott
Flatow
Cagey
E,
Surgery
of the shou/der.
Company,
1983.
Neer
C
der and Elbow
Surgeons,
C, Dalsey
R.
release
: 5th meeting
Las Vegas,
1989.
Philadelphia,
On
etc : JB
the value
of American
of the
Shoul-
RD.
AAOS.
HF,
recurrent
Anatomyfor
Harper
surgeons,
vo/ 3, the back
& Row, 1982; 270 :647-8.
The
frozen
shoulder.
In : Instructiona/
Course
St. Louis,
etc: CV Mosby
Co, 1985; 34:199-203.
Overgaard
anterior
clinical
studies
the gleno-humeral
B :91 3-27.
B.
The
dislocation
with
CS H, Foster
CR.
and
multidirectional
report.
J Bone Joint
special
ligaments.
anterior
reference
J Bone
Inferior
capsular
instability
of
Surg [Am]
1980;
73-B, No. 1, JANUARY
1991
capsular
of the shoulder
Nobuhara
44-50.
3rd ed.
mechanism
to the glenoid
labrum
Joint
Surg
[Br]
1962;
in
and
and
44-
shift for involuntary
inferior
the shoulder:
a preliminary
62-A :897-908.
H.
Rotator
interval
lesion.
J, Nielsen
S. Experimental
meraljoint.
Arch Orthop
Trauma
Ovesen
J, S#{248}jbjerg JO. Posterior
shoulder
capsular
lesions
in cadaver
experiments.
57:535-6.
C.
Rest
and
movement.
distal
Surg
J Bone
C/in
Orthop
1987;
subluxation
in the
1985 ; l04(2):78-91.
Joint
Surg
223:
glenohu-
dislocation
: muscle
Acta Orthop
Scand
[Am]
and
1986;
1953;
35-
B :521-39.
Protzman
RR.
[Am]
Rowe
CR,
Anterior
instability
of the
shoulder.
J Bone
subluxation
of the
Zarins
B. Recurrent
BoneJointSurg[Am]
Sl#{228}tis
P, Aalto
biceps
Testut
Joint
Surg
1980; 62-A :909-18.
transient
1981 ; 63-A
K. Medial
brachii.
Acta
shoulder.
J
:863-72.
Schwartz
RE, O’Brien
SJ, Warren
RF,
Torzilli
histology
ofthe
inferiorglenohumeralligament
Orthop
Soc for Sports
Medicine
meeting,
Las
Lectures,
: morphological
K, Ikeda
Ovesen
Perkins
and/imbs,
153
LIGAMENT
basis of
position
P, Sajbjerg
JO,
Andersen
PK, Nielsen
S. Ovesen
J. Distal
instability
of the shoulder
joint
after
severance
of capsule
and
ligaments
: an experimental
study.
Acta
Orthop
Scand
1988;
59(5):Suppl.
227 ; 74-5.
Moseley
VOL.
ed.
0, Bonfait
H, Gillot
C, Hureau
J, Mazas
F. Anatomic
ligamentous
control
ofelevation
ofthe
shoulder
(reference
ofthe
shoulderjoint).
Surg Radio/Anat
1987 ; 9:19-26.
Hoilinshead
WH.
Philadelphia:
Neer
Satterlee
ligament
Helmig
Leffert
II,
coracohumeral
3rd
CORACOHUMERAL
PA.
Anatomy
and
complex
: American
Vegas,
1989.
dislocation
of the tendon
of the
Orthop
Scand
1979; 50 :73-7.
L. Tratado
de antomia
humana.
Vol. 1, ed. and
Barcelona
: Salvat
Editores,
1932:1047-51.
rev.
TurkelSJ,
Panio MW, Marshall
JL,Gurgis
FG. Stabilizing
preventing
anterior
dislocation
of the glenohumeral
Joint Surg [Am]
1981 ; 63-A :1208-17.
long
head
of
by A. Latarjet.
mechanisms
joint.
J Bone