Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
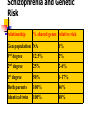
Schizophrenia Overview (part I) Ewa Pilaczyńska-Jodkiewicz What is schizophrenia? A chronic severe brain disorder; often they hear voices, believe media are broadcasting their thoughts to the world or may believe someone is trying to harm them. In men it usually develops in teen years and early 20s; in women it usually develops in 20s and 30s. Schizophrenia is the most severe and debilitating mental illness in psychiatry and is a brain disorder Definition The schizophrenic disorders are characterized in general by fundamental and characteristic distortions of thinking and perception, and affects that are inappropriate or blunted. Clear consciousness and intellectual capacity are usually maintained although certain cognitive deficits may evolve in the course of time. The most important psychopathological phenomena include thought echo thought insertion or withdrawal thought broadcasting delusional perception and delusions of control influence or passivity hallucinatory voices commenting or discussing the patient in the third person thought disorders and negative symptoms. Diagnosis Currently there is no physical or lab test that can absolutely diagnose schizophrenia. A psychiatrist usually comes to the diagnosis based on clinical symptoms. Misdiagnosis This is a common problem since schizophrenia shares a significant number of symptoms with other disorders. Per the Nat’l Depression & Bipolar Support Alliance there is an average of 10 years from onset to correct diagnosis & tx. Schizophrenia Schizophrenia occurs with regular frequency nearly everywhere in the world in 1 % of population and begins mainly in young age (mostly around 16 to 25 years). Schizophrenia is defined by a group of characteristic positive and negative symptoms deterioration in social, occupational, or interpersonal relationships continuous signs of the disturbance for at least 6 months Schizophrenia It has more impact on urban people than rural people It is a disease of the brain Epidemiology M=F (equally man and women) Females age of onset is generally later – better outcome Downward drift social-economically Die younger – 10% suicide History Emil Kraepelin: This illness develops relatively early in life, and its course is likely deteriorating and chronic; deterioration reminded dementia („Dementia praecox“), but was not followed by any organic changes of the brain, detectable at that time. Eugen Bleuler: He renamed Kraepelin’s dementia praecox as schizophrenia (1911); he recognized the cognitive impairment in this illness, which he named as a „splitting“ of mind. Kurt Schneider: He emphasized the role of psychotic symptoms, as hallucinations, delusions and gave them the privilege of „the first rank symptoms” even in the concept of the diagnosis of schizophrenia. Schizophrenia: Historical Perspectives 1 1893 Kraepelin distinguished “dementia praecox” from manic-depressive psychosis Emphasized course and prognosis Early onset Deteriorating course Dementia as the end state An “organic” brain disorder Schizophrenia: Historical Perspectives 2 1911 Bleuler coins “schizophrenia” in reference to the splitting of mental functions Emphasized psychological mechanisms Four fundamental features (“the 4 A’s”) Loosening of Associations Autistic behavior and thought Disturbance in Affect Ambivalence Psychosis = Accessory Symptoms 4 A (Bleuler) Bleuler maintained, that for the diagnosis of schizophrenia are most important the following four fundamental symptoms: affective blunting disturbance of association (fragmented thinking) autism ambivalence (fragmented emotional response) These groups of symptoms, are called „four A’ s” and Bleuler thought, that they are „primary” for this diagnosis. The other known symptoms, hallucinations, delusions, which are appearing in schizophrenia very often also, he used to call as a “secondary symptoms”, because they could be seen in any other psychotic disease, which are caused by quite different factors — from intoxication to infection or other disease entities. Schizophrenia is not caused by: Inadequate parenting Overzealous mothers Poor family relations It is not split personality Schizophrenia is a heterogeneous illness Defined by a constellation of symptoms, including psychosis Multifactorial etiology, variable course Social/occupational dysfunction a required diagnostic criterion Good treatment must address symptoms and social/occupational dysfunction Etiology of schizophrenia Genetic Structural brain changes Functional brain changes Dopamine hypothesis What exactly might be the cause of Schizophrenia? Is there a concrete explanation? The biological, cognitive, and behaviorist approaches all have their different theories to resolve a cure for this disorder. Research is revealing that schizophrenia is indeed a environmental impact during the the development of the brain during pregnancy and childhood. Another prediction is that is a result of the interaction of certain variations of genes. These would be the damaged portions of genes. The biological approach closely looks at the interaction between the environment and genetics. Some might say that the biological perspective is too radical, and reductionist, but it seems that genetics due play a major role in the involvement of this disorder. Research nowadays proposes the idea that schizophrenia is caused by a genetic vulnerability which is coupled with the environmental and psychological stressors. This is also known as the diathesisstress model. The idea basically says that whether the person develops the disorder or not, for the most part it is determined by the vulnerability. In overall, as said before…the biological approach closely looks at the genetic factors, and how they apply to the disorder. In this case, if there is a genetic vulnerability, it is more likely for the person to develop Schizophrenia. Etiology of Schizophrenia The etiology and pathogenesis of schizophrenia is not known It is accepted, that schizophrenia is „the group of schizophrenias“ which origin is multifactorial: internal factors – genetic, inborn, biochemical external factors – trauma, infection of CNS, stress Structural Brain Abnormalities in Schizophrenia ~40% increase in 3rd and lateral ventricular volumes Associated with more neuropsychological impairments and negative symptoms More prominent in males 3-4% decrease in whole brain volume Structural changes in brain Increased loss of gray matter in adolescence Structural changes in brain Hippocampus, amygdala, parahippocamp. Smaller in affected twin Disordered hippocampal pyramidal cells Correlation between cell disorder and severity May be due to maternal influenza in 2nd trimester Also in entorhinal, cingulate, parahippocampal cortex Structural changes in brain Larger ventricles Subgroup: inverse correlation between ventricle size and response to drugs Structural Brain Abnormalities in Schizophrenia Hippocampus and Association Cortices Decreased gray matter volume No cell loss Reductions in pre- and post-synaptic markers Structural Brain Abnormalities in Schizophrenia Mediodorsal thalamic nucleus Decreased volume ~30% Decrease in neuronal number Structural Brain Abnormalities in Schizophrenia Convergent lines of evidence indicate that schizophrenia is associated with A reduction in synaptic connections in the hippocampus and cerebral cortex. Fewer neurons in the mediodorsal thalamus. Which neurotransmitter systems are involved in these Schizophrenia as a Genetic Disorder The morbid risk of schizophrenia increases in relation to the percentage of genes shared with an affected individual. Genetics of Schizophrenia Many psychiatric disorders are multifactorial (caused by the interaction of external and genetic factors) and from the genetic point of view very often polygenically determined. Relative risk for schizophrenia is around: 1% for normal population 5.6% for parents 10.1% for siblings 12.8% for children It seems that Identical Twins hold the highest risk percentage to obtain this disorder…might this have a biological connection? Schizophrenia and Genetic Risk relationship % shared genes relative risk Gen population NA 1% 3rd degree 12.5% 2% 2nd degree 25% 2-6% 1st degree 50% 6-17% Both parents 100% 46% Identical twin 100% 48% The familial nature of schizophrenia is NOT due simply to a shared environment The risk of schizophrenia is ~17% for fraternal twins and ~48% for identical twins. The risk for adopted-away biological children of individuals with schizophrenia… is elevated as expected for first-degree relatives. higher than rates of schizophrenia present in their adoptive families. higher than rates of schizophrenia in the adopted-away offspring of unaffected parents. Dopamine hypothesis Amphetamine (very high doses) paranoia, delusions, auditory hallucination Amphetamines worsen schizophrenia symptoms Effects blocked by dopamine antagonist chlorpromazine (Thorazine) Typical antipsychotics block D2 receptors and alleviate positive symptoms. Brain Dopamine Pathways Nigrostriatal degenerates in Parkinson’s disease Mesolimbic positive symptoms of schizophrenia Mesocortical negative symptoms of schizophrenia Tuberoinfundibular Mesolimbic DA Hypothesis Hyperactivity of mesolimbic DA mediates positive symptoms of psychosis Accounts for these psychotic symptoms whether in SZ or other disorders Mesocortical DA Hypothesis Deficit of mesocortical DA mediates negative and cognitive symptoms of psychosis - more controversial - degenerative in some SZ patients - may be primary deficit - may be secondary drug effect Etiology of Schizophrenia Dopamine Hypothesis The most influential and plausible are the hypotheses, based on the supposed disorder of neurotransmission in the brain, derived mainly from 1. 2. the effects of antipsychotic drugs that have in common the ability to inhibit the dopaminergic system by blocking action of dopamine in the brain dopamine-releasing drugs (amphetamine, mescaline, diethyl amide of lysergic acid - LSD) that can induce state closely resembling paranoid schizophrenia Classical dopamine hypothesis of schizophrenia: Psychotic symptoms are related to dopaminergic hyperactivity in the brain. Hyperactivity of dopaminergic systems during schizophrenia is result of increased sensitivity and density of dopamine D2 receptors in the different parts of the brain. Dopamine blockade effects Limbic and frontal cortical regions: antipsychotic effect Basal ganglia: Extrapyramidal side effects (EPS) Hypothalamic-pituitary axis: hyperprolactinemia Deficits in Prefrontal Cortical Dopamine Neurotransmission in Schizophrenia Normal function of the DLPFC depends upon appropriate stimulation of dopamine D1 receptors Individuals with schizophrenia may have Decreased dopamine axons in the DLPFC Increased levels of D1 receptors in the DLPFC Improvement in DLPFC function with dopamine agonists Dopamine Neurotransmission in Schizophrenia The cognitive symptoms of schizophrenia may be associated with a functional deficit of dopamine at D1 receptors in the prefrontal cortex. The psychotic features of schizophrenia may be associated with a functional excess of dopamine at D2 receptors in the striatum (caudate/putamen). But, Schizophrenia Also Appears to be Associated with an Excess of Dopamine Neurotransmission Amphetamines can induce psychotic symptoms. All antipsychotic drugs share antagonism of the dopamine D2 receptor. Subjects with schizophrenia show excess release of dopamine in the striatum. Catechol-O-methyltransferase (COMT) Enzyme involved in the metabolic degradation of dopamine. COMT appears to be the major contributor to the termination of dopamine action in the prefrontal cortex due to low levels of the dopamine transporter. Single guanine to adenine transition (common) changes val to met at codon 108. Val-COMT has 4-fold greater activity than metCOMT, leading to decreased prefrontal dopamine levels. Schizophrenic individuals with val/val COMT show greater impairments on working memory Etiology of Schizophrenia Contemporary Models Dopamine hypothesis revisited: various neurotransmitter systems probably takes place in the etiology of schizophrenia (norepinephric, serotonergic, glutamatergic, some peptidergic systems); based on effects of atypical antipsychotics especially. Contemporary models of schizophrenia conceptualize it as a neurocognitive disorder, with the various signs and symptoms reflecting the downstream effects of a more fundamental cognitive deficit: the symptoms of schizophrenia arise from “cognitive dysmetria” (Nancy C. Andreasen) concept of schizophrenia as a neurodevelopmental disorder (Daniel R. Weinberger) Schizophrenia as an Environmental Disorder A variety of “environmental” events appear to increase the risk for schizophrenia: Pregnancy and labor/delivery complications Late winter/early spring births Urban place of birth and rearing Advanced paternal age However, the predictive value of all of these risk factors is low. Etiology of Schizophrenia Neurodevelopmental Model Neurodevelopmental model supposes in schizophrenia the presence of “silent lesion” in the brain, mostly in the parts, important for the development of integration (frontal, parietal and temporal), which is caused by different factors (genetic, inborn, infection, trauma...) during very early development of the brain in prenatal or early postnatal period of life. It does not interfere too much with the basic brain functioning in early years, but expresses itself in the time, when the subject is stressed by demands of growing needs for integration, during formative years in adolescence and young adulthood. Schizophrenia as a Neurodevelopmental Disorder During childhood and adolescence, individuals who subsequently manifest schizophrenia may exhibit… Motor abnormalities Social abnormalities Impairments in IQ and school performance Schizophrenia as a Neurodevelopmental Disorder Early model: Brain lesion from early in life remains clinically silent until normal developmental processes during adolescence bring the structures affected by the lesion “on line.” Late model: Brain dysfunction arises as a result of altered brain development (e.g., synaptic pruning) during adolescence. “The Behaviourist Approach interprets abnormal behavior as simply maladaptive learning.” From this, the behaviourist approach would then say that Schizophrenia is not regarded at all differently to other forms of abnormal behaviour. In other words, the behaviourist approach would actually see the term Schizophrenia as having no etiological value. Although the behaviourist approach does not believe that there seems to be an etiology for this disorder, it does have a number of different treatments for it, such as token economy. Schizophrenia affects multiple complex brain systems as evidenced by the range of clinical features Positive symptoms: Delusions, hallucinations, thought disorder Negative symptoms: Decreased motivation, diminished emotional expression Cognitive deficits: Impairments in attention, executive function, certain types of memory Sensory abnormalities: “Gating” disturbances Sensorimotor abnormalities: Eye tracking disturbances Motor abnormalities: Posturing, impaired coordination Features of Schizophrenia Negative symptoms Positive symptoms Functional Impairments Work Interpersonal relationships Self-care Cognitive deficits Mood symptoms Disorganizatio n Positive Symptoms (Psychosis) Disturbance of Perception (Hallucinations) Disturbance of Thought Content (Delusions) Features of Schizophrenia Positive symptoms Delusions Hallucinations Functional Impairments Work/school Interpersonal relationships Self-care Cognitive deficits Attention Memory Verbal fluency Executive function (eg, abstraction) Disorganization Speech Behavior Negative symptoms Anhedonia Affective flattening Avolition Social withdrawal Alogia Mood symptoms Depression/Anxiety Aggression/Hostility Suicidality Positive Symptoms Disturbance of Perception may effect any sensory modality Positive Symptoms: Hallucinations Auditory Hallucinations •involve voices or sounds •single or multiple •familiar or unfamiliar •may make insulting remarks or be pleasant •may comment on behavior •may command person to perform acts Positive Symptoms: Hallucinations Other Sensory Modalities • Tactile: may involve electrical, tingling, or burning sensations • Visual • Gustatory • Olfactory Positive Symptoms: Delusions Delusions •fixed false beliefs •examples: - persecutory delusions - delusions of reference - delusions of being controlled - thought broadcasting/insertion/withdrawal - grandiose - religious - nihilistic - somatic Features of Schizophrenia Positive symptoms - Hallucinations - Delusions Negative symptoms Functional Impairments Work Interpersonal relationships Self-care Cognitive deficits Mood symptoms Disorganization Negative Symptoms Negative symptoms include: decreased expression of feelings diminished emotional range poverty of speech decreased interests diminished sense of purpose diminished social drive Differential Diagnosis of Negative Symptoms Negative Symptoms primary to schizophrenia: The “Deficit Syndrome”: primary and enduring negative symptoms in individuals with schizophrenia The Deficit Syndrome occurs in about 20% of treated patients Differential Diagnosis of Negative Symptoms Negative Symptoms may be secondary to: antipsychotic EPS side effects - decreased emotional expression and apathy may be due to Parkinsonian side effects - lack of initiation of activity may be due to bradykinesia psychosis depression or anxiety Positive Symptoms: Disorganization • Disorganization of Speech – tangential or circumstantial speech – looseness of associations • Disorganization of Behavior – odd mannerisms – catatonic stupor Features of Schizophrenia Positive symptoms - Delusions - Hallucinations - Disorganization Functional Impairments Work Interpersonal relationships Self-care Cognitive deficits Negative symptoms - emotional range - expression of emotion - motivation/drive - interests - social drive - poverty of speech Mood symptoms Disorganization Cognitive Domains: Severe Impairment in Schizophrenia Severe Impairments – Serial learning – Executive functioning – Vigilance – Motor speed – Verbal Fluency Moderate Impairment – Delayed recall – Distractibility – Immediate memory span – Visuomotor skills – Working memory Cognitive Deficits in Schizophrenia: Core Features of the Illness Present in individuals at high risk Premorbid and prodromal phase marker Persistent (progressive?) during illness Predictor of long-term outcome Diagnosis of Schizophrenia A. Characteristic symptoms -Delusions -Hallucinations -Disorganized speech -Grossly disorganized or catatonic behavior -Negative symptoms B. Social/occupational dysfunction C. Overall duration > 6 months D. Exclude mood disorders, drugs, pervasive developmental disorders Positive Symptoms Additions to normal function Delusions Hallucinations Distorted language/communication Disorganised speech / behaviour Catatonic behaviour Agitation Negative Symptoms Losses of normal function -Affective flattening -Alogia -Avolition -Anhedonia -Attentional impairment Blunted affect, emotional withdrawal, poor rapport, passivity, apathetic, social withdrawal Cognitive Symptoms Thought disorder Odd use of language incoherence, loose associations, neologisms Impaired attention / cognition reduced verbal fluency learning/memory executive functions Subtypes of schizophrenia Paranoid Disorganized Catatonic Undifferentiated Residual Course of Illness Course of schizophrenia: continuous without temporary improvement episodic with progressive or stable deficit episodic with complete or incomplete remission Typical stages of schizophrenia: prodromal phase active phase residual phase Clinical Picture Diagnostic manuals: lCD-10 („International Classification of Disease“, WHO) DSM-IV („Diagnostic and Statistical Manual“, APA) Clinical picture of schizophrenia is according to lCD-10, defined from the point of view of the presence and expression of primary and/or secondary symptoms (at present covered by the terms negative and positive symptoms): the negative symptoms are represented by cognitive disorders, having its origin probably in the disorders of associations of thoughts, combined with emotional blunting and small or missing production of hallucinations and delusions the positive symptom are characterized by the presence of hallucinations and delusions the division is not quite strict and lesser or greater mixture of symptoms from these two groups are possible Positive and Negative Symptoms Negative Alogia Affective flattening Avolition-apathy Anhedonia-asociality Positive Hallucinations Delusions Bizarre behaviour Positive formal thought disorder Attentional impairment Andreasen N.C., Roy M.-A., Flaum M.: Positive and negative symptoms. In: Schizophrenia, Hirsch S.R. and Weinberger D.R., eds., Blackwell Science, pp. 28-45, 1995 The Criteria of Diagnosis For the diagnosis of schizophrenia is necessary presence of one very clear symptom - from point a) to d) or the presence of the symptoms from at least two groups - from point e) to h) for one month or more: a) the hearing of own thoughts, the feelings of thought withdrawal, thought insertion, or thought broadcasting b) the delusions of control, outside manipulation and influence, or the feelings of passivity, which are connected with the movements of the body or extremities, specific thoughts, acting or feelings, delusional perception c) hallucinated voices, which are commenting permanently the behavior of the patient or they talk about him between themselves, or the other types of hallucinatory voices, coming from different parts of body d) permanent delusions of different kind, which are inappropriate and unacceptable in given culture The Criteria of Diagnosis e) the lasting hallucination of every form f) blocks or intrusion of thoughts into the flow of thinking and resulting incoherence and irrelevance of speach, or neologisms g) catatonic behavior h) „the negative symptoms”, for instance the expressed apathy, poor speech, blunting and inappropriatness of emotional reactions i) expressed and conspicuous qualitative changes in patient’s behavior, the loss of interests, hobbies, aimlesness, inactivity, the loss of relations to others and social withdrawal Diagnosis of acute schizophorm disorder (F23.2) – if the conditions for diagnosis of schizophrenia are fulfilled, but lasting less than one month Diagnosis of schizoaffective disorder (F25) - if the schizophrenic and affective symptoms are developing together at the same time DSM-IV Schizophrenia 2 or more of the following for most of 1 month: Delusions Hallucinations Disorganized speech Grossly disorganized or catatonic behavior Negative symptoms Social/occupational dysfunction Duration of at least 6 months Not schizoaffective disorder or a mood disorder with psychotic features Not due to substance abuse or a general medical disorder F20-F29 Schizophrenia, Schizotypal and Delusional Disorders F20 F20.0 F20.1 F20.2 F20.3 F20.4 F20.5 F20.6 F20.8 F20.9 Schizophrenia Paranoid schizophrenia Hebephrenic schizophrenia Catatonic schizophrenia Undifferentiated schizophrenia Post-schizophrenic depression Residual schizophrenia Simple schizophrenia Other schizophrenia Schizophrenia, unspecified F20-F29 Schizophrenia, Schizotypal and Delusional Disorders F21 Schizotypal disorder F22 F22.0 F22.8 F22.9 Persistent delusional disorders Delusional disorder Other persistent delusional disorders Persistent delusional disorder, unspecified F23 F23.1 Acute and transient psychotic disorders Acute polymorphic psychotic disorder with symptoms of schizophrenia Acute schizophrenia-like psychotic disorder Other acute predominantly delusional psychotic disorders Other acute and transient psychotic disorders Acute and transient psychotic disorder, unspecified F23.2 F23.3 F23.8 F23.9 F20-F29 Schizophrenia, Schizotypal and Delusional Disorders F24 Induced delusional disorder F25 F25.0 F25.1 F25.2 F25.8 F25.9 Schizoaffective disorders Schizoaffective disorder, manic type Schizoaffective disorder, depressive type Schizoaffective disorder, mixed type Other schizoaffective disorders Schizoaffective disorder, unspecified F28 Other nonorganic psychotic disorders F29 Unspecified nonorganic psychosis Symptoms Positive symptoms: common schizophrenia behaviors Delusions: false beliefs kept despite contrary evidence. (believing you are the Virgin Mary) Hallucinations: false perceptions (usually hearing voices) mental disturbance: illogical thought, incoherent speech, word usage shifts. Negative Symptoms: absence of expected behavior Physical immobility No emotional expression Little speech Withdrawal from social world Schizophrenia: the affected person may: Talk to himself Gesture to himself Dress in layers in any weather Fail to bathe and get a haircut Gain an odd interest in ordinary things (like religion) Schizophrenia: the affected person may: May even believe he is God See things Feel people are out to get them Believe in all sorts of conspiracies Have ideas that no amount of evidence to the contrary can dislodge Schizophrenia: the affected person may: Be unable to work Stop talking or greatly reduce conversation Appear lazy, unmotivated and uninterested May look like he has dementia Lose the ability to get and keep friends Be tense Positive Symptoms Delusions. Those where the patient thinks he is being followed or watched are common; also the belief that people on TV, radio are directing special messages to him/her. Positive Symptoms Hallucinations. Distortions or exaggerations of perception in any of the senses. Often they hear voices within their own thoughts followed by visual hallucinations. Positive Symptoms Disorganized thinking/speech. loose associations; speech is tangential, loosely associated or incoherent enough to impair communication. Positive Symptom Grossly disorganized behavior. Difficulty in goal directed behavior (ADLs), unpredictable agitation or silliness, social disinhibition, or bizarre behavior. There is a purposelessness to behavior. Positive Symptom Catatonic behavior. Marked decrease in reaction to immediate environment, sometimes just unaware of surroundings, rigid or bizarre postures, aimless motor activity. Other Positive Symptoms Inappropriate response to stimuli Unusual motor behavior (pacing, rocking) Depersonalization Derealization Somatic preoccupations Summary of Positive Symptoms Delusions Hallucinations Disorganized thinking Disorganized behavior Catatonic behavior Inappropriate responses Positive Symptoms Positive symptoms are those that have a positive reaction from some treatment. In other words, positive symptoms respond to treatment. Negative Symptoms Those that appear to reflect a diminution or loss of normal functions. May be difficult to evaluate because they are not as grossly abnormal as positive symptoms. Negative Symptoms Affective flattening. Reduction in the range and intensity of emotional expression, including facial expression, voice tone, eye contact and body language. Negative Symptom Alogia (poverty of speech) Lessening of speech fluency and productivity, thought to reflect slowing or blocked thoughts; often manifested as short, empty replies to questions. Negative Symptom Avolition The reduction, difficulty or inability to initiate and persist in goal-directed behavior. Often mistaken for apparent disinterest. Examples of Avolition No longer interested in going out with friends No longer interested in activities that the person used to show enthusiasm No longer interested in anything Sitting in the house for hours or days doing nothing Disorganized Symptoms This one is somewhat new and may not be considered valid. It is thought disorder, confusion, disorientation and memory problems. Summary of Negative Symptoms Lack of emotion Low energy Lack of interest in life Affective flattening Alogia Inappropriate social skills Inability to make friends Social isolation Cognitive Symptoms Difficulties in concentration and memory: Disorganized thinking Slow thinking Difficulty understanding Poor concentration Poor memory Difficulty expressing thoughts Difficulty integrating thoughts, feelings, behaviors Negative Symptoms Currently there is no treatment that has a consistent impact on negative symptoms. What are the symptons associated with the different types of schizophrenia? Paranoid Schizophrenia Delusions, hallucinations, misinterpretation of facts Violent, suicidal behavior - high risk Ex: patient images that he is someone else or someone is trying to harm him. Imaginary voices F20.0 Paranoid Schizophrenia Paranoid schizophrenia is characterized mainly by delusions of persecution, feelings of passive or active control, feelings of intrusion, and often by megalomanic tendencies also. The delusions are not usually systemized too much, without tight logical connections and are often combined with hallucinations of different senses, mostly with hearing voices. Disturbances of affect, volition and speech, and catatonic symptoms, are either absent or relatively inconspicuous. Paranoid Schizophrenia Persons are very suspicious of others and often have grand schemes of persecution at the root of their behavior. During this phase they may have hallucinations and frequent delusions. F20.1 Hebephrenic Schizophrenia Hebephrenic schizophrenia is characterized by disorganized thinking with blunted and inappropriate emotions. It begins mostly in adolescent age, the behavior is often bizarre. There could appear mannerisms, grimacing, inappropriate laugh and joking, pseudophilosophical brooding and sudden impulsive reactions without external stimulation. There is a tendency to social isolation. Usually the prognosis is poor because of the rapid development of "negative" symptoms, particularly flattening of affect and loss of volition. Hebephrenia should normally be diagnosed only in adolescents or young adults. Denoted also as disorganized schizophrenia Hebephrenic Schizophrenia Disorganized schizophrenia; characterized by emotionless, incongruous, or silly behavior, intellectual deterioration, frequently beginning insidiously during adolescence. May be verbally incoherent and may have moods and emotions that are not appropriate to the situation. Hallucinations not usually present. Catatonic Schizophrenia Negative Symptoms Abnormal posture/movements Repeated motions Motionlessness Inactivity/Excitement periods Impulsiveness F20.2 Catatonic Schizophrenia Catatonic schizophrenia is characterized mainly by motoric activity, which might be strongly increased (hypekinesis) or decreased (stupor), or automatic obedience and negativism. We recognize two forms: productive form — which shows catatonic excitement, extreme and often aggressive activity. Treatment by neuroleptics or by electroconvulsive therapy. stuporose form — characterized by general inhibition of patient’s behavior or at least by retardation and slowness, followed often by mutism, negativism, fexibilitas cerea or by stupor. The consciousness is not absent. Catatonic Schizophrenia Person is extremely withdrawn, negative and isolated. May have marked psychomotor disturbances. F20.5 Residual Schizophrenia A chronic stage in the development of schizophrenia with clear succession from the initial stage with one or more episodes characterized by general criteria of schizophrenia to the late stage with longlasting negative symptoms and deterioration (not necessarily irreversible). Residual Schizophrenia Lacks motivation and interest in day-today living. Person is not usually having delusions, hallucinations or disorganized speech. F20.4 Postschizophrenic Depression A depressive episode, which may be prolonged, arising in the aftermath of a schizophrenic illness. Some schizophrenic symptoms, either „positive“ or „negative“, must still be present but they no longer dominate the clinical picture. These depressive states are associated with an increased risk of suicide. F20.6 Simple Schizophrenia Simple schizophrenia is characterized by early and slowly developing initial stage with growing social isolation, withdrawal, small activity, passivity, avolition and dependence on the others. The patients are indifferent, without any initiative and volition. There is not expressed the presence of hallucinations and delusions. Schizoaffective Disorder There will be symptoms of schizophrenia as well as mood disorder (depression, bipolar, mixed mania). Undifferentiated Schizophrenia Conditions meeting the general diagnostic criteria for schizophrenia but not conforming to any of the previous types. Exhibits more than one of the previous types without a clear dominance of one. Summary Before a diagnosis the psychiatrist must make a thorough evaluation including a physical/medical exam, a mental status exam, appropriate labs, and a full history. History includes changes in thinking, behavior, movement, mood, etc. as seen by the family. Increased Mortality Rates for Medical Disorders in schizophrenia 50% increased risk of death from medical causes in schizophrenia, and 20% shorter lifespan (Harris et al. Br J Psychiatry 1998;173:11) 123 Medical Comorbidity With Schizophrenia Is Very Common Physical Disease With Increased Frequency in Schizophrenia Tuberculosis HIV++ Hepatitis B/C Osteoporosis/decreased bone mineral density Poor dental status Impaired lung function Sexual dysfunction Extrapyramidal side effects of antipsychotic drugs; motor signs in antipsychotic-naive patients Obstetric complications++ Hyperprolactinemia-related side effects of antipsychotics (eg, irregular menses, galactorrhea) Cardiovascular problems++ Hyperpigmentation (side effect of chlorpromazine) Obesity++, diabetes, hyperlipidemia, metabolic syndrome Thyroid dysfunction (++) very good evidence for increased risk (eg, population-based studies). 124 Conclusions Morbidity in terms of rates of a number of physical illnesses is clearly increased in schizophrenia. The amount and quality of epidemiolgical studies found in some areas – especially some hot topics – could be better (e.g. obesity where more work is underway) Surprising medical particularities such 125