Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
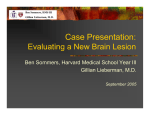
Rebecca Aspden, HMS III Gillian Lieberman, MD Achilles Tendon Rupture Rebecca Aspden, Harvard Medical School Year III Gillian Lieberman, MD November 15, 2004 1 Rebecca Aspden, HMS III Gillian Lieberman, MD Achilles tendon: •Largest tendon in body. •Formed from conjoined tendons of gastrocnemius and soleus muscles. •Inserts on calcaneus. •Contributes to plantar flexion of foot. www.medicalmultimediagroup.com 2 Rebecca Aspden, HMS III Gillian Lieberman, MD Types of Achilles Tendon Injury z Peritendinosis (peritendinitis) – Edema and scarring of paratenon (fatty areolar tissue around tendon). – Acute pain and swelling. – Seen in runners who increase their training or run on uneven surfaces. z Tendinosis – Intrasubstance degeneration of tendon itself. z Tears (partial or complete) – Vulnerable zone of avascularity 2-6 cm above calcaneal insertion. 3 Rebecca Aspden, HMS III Gillian Lieberman, MD Who gets tears? Average age 35-40. • Sports act is often triggering factor. • • “Weekend Warrior” In elderly underlying systemic disease or long-term corticosteroid medication may contribute. • Chronic degeneration of tendon (tendinosis) may be predisposing factor. • 4 Rebecca Aspden, HMS III Gillian Lieberman, MD Our patient Mr. S is a 37 year-old man who was playing basketball at the local YMCA on Saturday afternoon. Even though Mr. S was a serious athlete in college, in the years since graduation he only makes it to the gym once a week for a pick-up game with his buddies from the office. As he was starting to chase after the ball, Mr. S felt a sudden pain in his left calf and heard a snap. He thought he had been shot! He could not walk and immediately limped to the sideline. 5 Rebecca Aspden, HMS III Gillian Lieberman, MD Diagnosis Diagnosis of Achilles Tendon rupture can almost always be made clinically. • Look for: – Palpable gap in tendon – Positive Thompson test – Difficulty standing on toes – Tenderness UpToDate 6 Rebecca Aspden, HMS III Gillian Lieberman, MD Imaging Options z z z Plain films are not very helpful. In questionable cases ultrasound can provide definitive diagnosis (particularly good in differentiating partial from complete rupture). MRI helpful in planning surgery and in identifying intratendon abnormalities such as tears, tendinosis, and retrocalcaneal bursitis. – Helps surgeon decide whether to approximate tendon ends or use allograft. 7 Rebecca Aspden, HMS III Gillian Lieberman, MD Plain film of torn Achilles PACS, BIDMC 8 Rebecca Aspden, HMS III Gillian Lieberman, MD Longitudinal sonogram showing partial-thickness tear Hartgerink et al. Tendon is markedly thickened and hypoechoic. 9 Rebecca Aspden, HMS III Gillian Lieberman, MD Longitudinal sonogram showing full-thickness tear Hartgerink et al. This ultrasound shows posterior shadowing (due to sound beam refraction at frayed tendon ends) and 9 mm of retraction with tendon debris between calipers. Another sign of tear on ultrasound is fat herniation. 10 Rebecca Aspden, HMS III Gillian Lieberman, MD Tendons on MRI Proton Density T2 Normal DARK DARK Degenerated (tendinosis) Torn BRIGHT DARK BRIGHT BRIGHT 11 Rebecca Aspden, HMS III Gillian Lieberman, MD NORMAL - axial Proton density T2 PACS, BIDMC PACS, BIDMC Achilles tendon 12 Rebecca Aspden, HMS III Gillian Lieberman, MD NORMAL - sagittal Proton density T2 PACS, BIDMC Achilles tendon PACS, BIDMC 13 Rebecca Aspden, HMS III Gillian Lieberman, MD Tendons on MRI Normal Proton Density DARK T2 DARK Degenerated BRIGHT DARK BRIGHT BRIGHT (tendinosis) Torn 14 Rebecca Aspden, HMS III Gillian Lieberman, MD DEGENERATED - axial Proton density PACS, BIDMC T2 PACS, BIDMC slightly increased signal 15 Rebecca Aspden, HMS III Gillian Lieberman, MD DEGENERATED - sagittal Proton density T2 PACS, BIDMC PACS, BIDMC thickened tendon 16 Rebecca Aspden, HMS III Gillian Lieberman, MD Tendons on MRI Normal Degenerated (tendinosis) Torn Proton Density DARK T2 DARK BRIGHT DARK BRIGHT BRIGHT 17 Rebecca Aspden, HMS III Gillian Lieberman, MD TEAR - axial Proton density T2 tear PACS, BIDMC intact plantaris tendon PACS, BIDMC 18 Rebecca Aspden, HMS III Gillian Lieberman, MD TEAR - sagittal Proton density PACS, BIDMC avulsed piece of bone T2 PACS, BIDMC 19 Rebecca Aspden, HMS III Gillian Lieberman, MD Torn Summary - sagittal Degenerated PACS, BIDMC Normal PACS PACS, BIDMC Proton Density Images 20 PACS, BIDMC Rebecca Aspden, HMS III Torn Gillian Lieberman, MD Summary - axial Degenerated PACS, BIDMC Normal PACS, BIDMC Proton Density Images 21 PACS, BIDMC Rebecca Aspden, HMS III Gillian Lieberman, MD Treatment for Achilles tendon rupture z Surgery followed by early mobilization has had better results than just immobilizing tendon with cast for 8 weeks. z Active rehabilitation phase after surgery is 6 months long. z Most patients can return to pre-injury activity including sports. 22 Rebecca Aspden, HMS III Gillian Lieberman, MD Conclusion •Achilles tendon rupture is often seen in middle-aged men who exercise infrequently. •Diagnosis is usually made without imaging but US can be used in questionable cases. •MRI is used in surgical planning. www.home.zonnet.nl 23 Rebecca Aspden, HMS III Gillian Lieberman, MD References Anderson, J., J.W. Read, and J. Steinweg. Atlas of Imaging in Sports Medicine. Sydney: McGraw-Hill Australia, 1998. Andrews, J.R., B. Zarins, and K.E. Wilk, ed. Injuries in Baseball. New York: Lippincott-Raven Publishers, 1998. Halpern, B., S.A. Herring, D. Alcheck, and R. Herzog. Imaging in Musculoskeletal and Sports Medicine. Malden, MA: Blackwell Science, 1997. Hartgerink. P. et al. Full- versus Partial-Thickness Achilles Tendon Tears: Sonographic Accuracy and Characterization in 26 Cases with Surgical Correlation. Radiology 220: 406-412, 2001. Kerr, Roger. Magnetic Resonance Imaging of the Foot and Ankle. Seminars in Roentgenology 35(3): 306-318, 2000. Kjaer, M. et al, ed. Textbook of Sports Medicine. Malden, MA: Blackwell Science, 2003. Moore, K.L. and A.F. Dalley. Clinically Oriented Anatomy. New York: Lippincott Williams & Wilkins, 1999. Southmayd, William and Marshall Hoffman. Sports Health. New York: Quick Fox, 1981. 24 Rebecca Aspden, HMS III Gillian Lieberman, MD Acknowledgements Thanks to Larry Barbaras, Gillian Lieberman, Pamela Lepkowski, Alice Fisher, and Mary Hochman. Without their encouragement, inspiration, and technical help, this presentation would not have been possible. 25