Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cell encapsulation wikipedia , lookup
Drug discovery wikipedia , lookup
MTOR inhibitors wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Drug design wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Neuropharmacology wikipedia , lookup
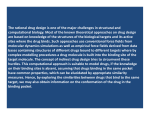
JULS The Development of Novel Small Molecules as Protein Tyrosine Kinase Inhibitors for the Treatment of Cancer Julia X Su Review Article Fourth Year Undergraduate Student in Pharmaceutical Chemistry Specialist, Deparment of Pharmaceutical Science, University of Toronto, Toronto, Canada Abstract Protein Tyrosine Kinases (PTKs) are important regulators of signalling, growth and proliferation of cells. In cancer cells, overexpression or gain-of-function mutations causes PTKs to become constitutively active, causing uncontrolled growth and proliferation. Studies of the common PTKs mutations can lead to potential treatment of cancer through developing novel small molecules which selectively target the mutated PTKs. This review summarizes the diseases associated with four different mutated PTKs, Bcr-Abl, Anaplastic Lymphoma Kinase (ALK), Fms-Like Tyrosine Kinase 3 (FLTK3) and Fibroblast Growth Factor Receptor 3 (FGFR3). This review will also discuss the small molecules developed to specifically inhibit each of these mutated PTKs. Being on different stages of the drug development process, the small molecule inhibitors have so far been shown to be effective at PTK inhibition, demonstrating their potential as therapeutic anti-cancer agents. Though a large numbers of tests and clinical trials are still needed before these molecules can be proven to be safe and efficacious in humans, continuous studies on small molecule inhibitors of PTKs will lead to new understanding of cellular pathways and more effective therapies for the treatment of cancer. . Protein Tyrosine Kinase Protein Tyrosine Kinases (PTKs) play important roles in signalling, growth and proliferation of cells. Upon ligand binding, PTKs catalyze the transfer of the phosphate group of ATP to tyrosine residues of their protein substrates. PTKs consist of two subclasses, the Receptor Tyrosine Kinases (RTKs), a type of cell surface receptor that has intrinsic kinase activity and the non-receptor tyrosine kinases, which can be either cytoplasmic or nuclear proteins. Currently, there are 90 known PTK genes in the human genome, out of which, 58 encoding transmembrane RTK genes, and 32 encoding non-receptor PTKs [1]. Both subclasses of PTKs are involved in critical growth and proliferative pathways in the cell. In tumours with mutated and constitutively active PTKs, the growth and proliferation of cancer cells become highly dependent on the mutated PTKs and their associated signalling pathways [1]. The growth and proliferation of cells can thus become uncontrolled. Because of PTKs’ involvement in cell proliferation in various cancers, they have been identified as excellent therapeutic targets in the rational drug discovery process. Based on the crystal structure of the PTK, various small chemical molecules are designed using computational tools to selectively inhibit the targeted PTK [2]. Currently, in the pharmaceutical industry, larger efforts are devoted to designing these small molecules and testing their efficacy in inhibiting PTKs for the treatment of cancer. This review summarizes the mutations and diseases associated with four different PTKs, their mechanism of actions, and the inhibitory efficacy of several small molecules devel- 2 Journal of Undergraduate Life Sciences oped specifically for mutated PTKs. Bcr-Abl One of the most familiar examples of PTK inhibition for cancer treatment is the targeting of Bcr-Abl, the mutant PTK resulted from a chromosomal translocation. The Philadelphia chromosome (Ph-chromosome), produced by the fusion of portions of chromosome 9 and chromosome 22, is the genetic cause of 95% of chronic myeloid leukemia (CML) and 20% of acute lymphoblastic leukemia (ALL) [3]. The resultant fusion protein, Bcr-Abl PTK becomes constitutively active and transfers the phosphate group of ATP to various substrate proteins, which in turn activates a whole cascade of downstream pathways, resulting in the activation or improper stabilization of some well-known oncoproteins, such as MYC and JAK2 [4]. In 1996, a small molecule STI571 (imatinib) was discovered and developed by Novartis (Basel, Switzerland) to selectively inhibit Bcr-Abl [5]. Imatinib was shown to bind to the ATP binding site on the Abl protein and stabilize the fusion protein in its inactive conformation, thereby inhibiting its kinase activity and preventing the activation of downstream pathways [5]. In clinical studies, imatinib has substantial tumour reduction activity in CML and in Ph-chromosome positive ALL [6]. Imatinib was later introduced to the market under the name Gleevec, as a frontline therapy for CML. However, since the introduction of Gleevec to the market, its secondary resistance in patients is commonly encountered and has attracted enormous research interests. Clinical resistance is primarily caused by point mutations in the kinase The Development of Novel Small Molecules as Protein Tyrosine Kinase Inhibitors for the Treatment of Cancer domain of Bcr-Abl [7]. Since imatinib can only bind to the ATP binding site of Abl when the activation loop is closed, it is believed that the majority of the amino acid substitutions impairs the ability of Abl to adopt its specific closed conformation and prevents imatinib from binding [8]. As a result, a derivative of imatinib that has less rigid binding requirements is needed to overcome the resistance. Another small molecule, BMS-354825 (dasatinib) was discovered in 2004, which is able to bind to Bcr-Abl in both open and closed conformations, thus demonstrating its ability to target most imatinib-resistant Bcr-Abl mutations [9]. Recently, another derivative of imatinib, nilotinib was brought to clinical trials with a more favourable safety profile and reduced side effects when administered at a similar dose [10]. Nilotinib caused less myelosuppression and fewer nonhematologic adverse effects than imatinib. In a clinical trial, 86 patients who were intolerant to imatinib were administered nilotinib, and only 2 out of these 86 patients developed grade 3 or 4 adverse events in the nilotinib treatment (Table 1) [10]. This reduction in side effects can be explained by nilotinib’s higher selectivity for Bcr-Abl. Nilotinib provides an alternative treatment for diseases that have become resistant or intolerant to imatinib. Table 1. Comparison of nonhematologic adverse events observed in imatinib-intolerant patients treated with nilotinib. Grade 3/4 adverse events Rash/skin Liver toxicity Fluid retention Gastrointestinal intolerance Musculoskeletal Other Total Patients with toxicity on imatinib, no. 25 10 17 15 Patients with toxicity on nilotinib, no. 0 1 0 1 9 10 86 0 0 2 86 patients who were intolerant to imatinib were administered nilotinib. [10]. ALK (Anaplastic Lymphoma Kinase) After the success of Gleevec, the efforts in developing mechanism-based therapy for cancer have brought forth many more small molecules to inhibit other mutated PTKs. One example is the inhibition of mutated anaplastic lymphoma kinase (ALK). Mutated ALK is the cause of cancers like anaplastic large-cell lymphoma (ALCL) and neuroblastoma [13]. In ALCL, 50-60% of the cases are associated with the fusion of the nucleophosmin (NPM) gene on chromosome 5 to a portion of the ALK gene on chromosome 2, generating a chimeric NPM-ALK protein that is constitutively active, and leading to tumour formation [14]. In neuroblastoma, the ALK positive tumours do not show the same chromosomal translocation, but acquire point mutations in the ALK gene. These non-synonymous sequence variations in conserved positions of the tyrosine kinase domain, such as F1174L and R1275Q, are associated with constitutive phosphorylation of ALKs and downstream signalling proteins, such as STAT3 and AKT, which are regulators that can induce protein synthesis pathways and promote oncogenesis [15]. Galkin et. al developed a cell proliferation assay using a NPM-ALK transformed murine cell line and were able to identify a small molecule, TAE684, which selectively blocked ALK activity and signal transduction by occupying the ALK’s ATP binding site [16]. The inhibition was shown to be accompanied by a rapid and sustained reduction in ALK autophosphorylation, dose-dependent reduction of phosphorylation of downstream proteins ERK and AKT, and down-regulation of CD30 expression, a marker of ALCL [14]. With the administration of TAE684 in the cell culture, the proliferation and survival of NPM-ALK transformed cancer cells decreased dramatically (Figure 1) [16]. In addition, TAE684 was shown efficacious in tumours involving both a translocation and point mutations of the ALK gene in a mouse model [16]. Currently, TAE684 is still under investigation for optimization and testing. There are currently no clinical trial data regarding the use of TAE684 in humans. It will be intriguing to know if TAE684 demonstrates safety and the same level of efficacy in humans as it has in cell cultures and animal models. FLT3 (Fms-Like Tyrosine Kinase 3) Fms-like tyrosine kinase (FLT3), a member of the receptor PTKs, plays an important role in the proliferation, differentiation and survival of hematopoietic stem cells and progenitor cells [17]. Thirty percent of acute myeloid leukemia (AML) patients show FLT3 positive tumours [18]. The mutations involve either an internal tandem duplication of amino acids in the juxtamembrane (JM) domain of the receptor, or a point mutation in the activating loop which changes the conformation of this domain and causes the receptor to adopt an active conformation [18]. Both types of FLT3 mutations result Journal of Undergraduate Life Sciences Volume 4 • No. 1 • Spring 2010 Another advantage of nilotinib over imatinib comes from its differential susceptibility to drug efflux pumps, which are highly expressed in hematopoietic stem cells [9]. These drug efflux pumps actively transport substrates such as anti-cancer drug molecules out of the cell, resulting in a decreased concentration of drugs at the target sites, and therefore a decreased drug efficacy. Imatinib is a substrate of P-glycoprotein, a multidrug resistance protein, while nilotinib is able to inhibit these efflux pumps, such as the human multidrug resistance protein [11]. Therefore, nilotinb can achieve higher therapeutic concentration at target sites and longer duration of action than imatinib, improving its effectiveness in the human body [11]. Furthermore, there are benefits to explore combinatorial therapy for the treatment of CML. The possibility of developing a cocktail of kinase inhibitors with activity against all drug resistant Bcr-Abl mutations is presently being investigated [9]. Studies have also showed that combining Bcr-Abl targeted small molecules with other current standard treatments for CML, which include stem cell transplantation, interferonalpha-containing regimens, cytosine arabinoside and daunorubicin showed additive or synergistic effects [12]. 3 in FLT3s that are active in the absence of the endogenous FLT3 ligand, a growth factor, leading to tumour formation [17]. Figure 1. TAE684 inhibits cell proliferation of Karpas-299 and Su-DHL-1 cell lines, which are established human ALCL cell lines expressing NPM-ALK [16]. In 2002, Weisberg discovered that small molecule PKC412 (N-benzoyl staurosporine) had the ability to directly inhibit both mutant and wild-type FLT3 [19]. PKC412 is a synthetic derivative of the naturally occurring alkaloid staurosporine and was developed originally as an inhibitor for tyrosine kinases such as c-kit and the vascular endothelial growth factor receptor [19]. In cell culture studies, PKC412 inhibits the autophosphorylation of mutant FLT3 receptors and reduces proliferation of FLT3 positive tumour cells by inducing apoptosis and cell cycle arrest [19]. PKC412 also proves to be efficacious in an animal model of leukemia, using mice transplanted with marrow cells infected by FLT3 mutant allele retrovirus [19]. In clinical studies, PK412 was also shown to be effective and well tolerated by cancer patients with FLT3 mutations, and no significant side effects were found when it was administered at its therapeutic level [18]. However, the serum level of free PKC412 was generally low due to a large extent of plasma protein binding, leading to decreased concentration of free active drug at the target site, which has a negative impact on its efficacy [18]. Because only the free unbound drug in the blood will enter cells, it may be useful to alter the structure of PKC412 in a way that decreases its binding affinity to albumin in the blood, and increase the drug efficacy. FGFR3 (Fibroblast Growth Factor Receptor 3) In an oncogenic form of fibroblast growth factor receptor 3 (FGFR3), the immunoglobulin heavy chain (IgH) locus on chromosome 14 can recombine with the locus on chromosome 4, giving rise to the aberrant expression and dysregulation of FGFR3 [20]. This reciprocal chromosomal translocation occurs in 15% of patients with multiple myeloma (MM), a B cell neoplasm characterized by clonal expansion of plasma cells in the bone marrow [21]. MM patients with this specific translocation show a significantly worse prognosis, with minimal benefit from receiving a stem cell transplant [21]. A novel treatment approach is therefore necessary for these patients, 4 Journal of Undergraduate Life Sciences and the development of a small molecule to inhibit mutant FGFR3 would be highly beneficial. CHIR258, a novel benzimidazole-quinolinone is a small molecule that inhibits several classes of PTKs, including FGFR3, platelet-derived growth factor receptor (PDGFR) and C-kit [21]. In cell culture studies, CHIR258 has been shown to inhibit FGFR3 autophosphorylation and therefore cell proliferation in human myeloma cell lines expressing wild type or activated mutant FGFR3 [21]. CHIR258 administration also resulted in a reduction of the phosphorylation of a downstream signalling molecule, FRS2, which directly interacted with FGFR3 [22]. Trudel et al. demonstrated the therapeutic efficacy of CHIR258 in a xenograft mouse model of FGFR3 MM [21]. In an orthotopic MM model in mice, Xin et al. demonstrated that CHIR258’s efficacy exceeded the proteosome inhibitor Velcade, the current standard therapy approved for treatment of MM in humans, providing strong support for starting clinical trials of CHIR258 in FGFR3 positive MM patients [22]. Because CHIR258 is known to inhibit other PTKs, such as the PDGFR, it is likely that the off-target inhibition of PDGFR contributes to the efficacy of CHIR258 in the orthotopic model of MM [22]. More studies need to be conducted for a detailed understanding of the contribution of PDGFR to MM and the molecular interaction of CHIR258 with PDGFR. Conclusion Cancer is becoming more prevalent in today’s society. According to the Canadian Cancer Society, almost 40% of Canadian women and 45% of Canadian men will develop cancer during their lifetimes [23]. Standard chemotherapy for cancer is associated with toxicity and may be ineffective for some patients. Highly efficacious and targeted small molecules are promising alternative treatments. The success of the oncoprotein-directed compound Gleevec has led to a breakthrough in the treatment of cancer. Gleevec demonstrates the power of rational drug discovery, presenting PTKs as suitable molecular targets. Small molecules can be developed to selectively inhibit the mutant PTKs, turn off the downstream signalling pathways and induce apoptosis or growth arrest of cancer cells. Though proteins downstream of a mutant PTK receptor in proliferative or survival pathways can also serve as therapeutic targets, directly targeting the activated kinase itself is often the better choice, because many signal transduction pathways have a high degree of redundancy [18]. In this review, four different receptor tyrosine kinases and their small molecule inhibitors are investigated and characterized (Table 2). The four PTKs summarized are associated with different genetic mutations that lead to various cancers. The Development of Novel Small Molecules as Protein Tyrosine Kinase Inhibitors for the Treatment of Cancer Table 2. Summary of the Protein Tyrosine kinases reviewed in this paper, the causes of their defects and the small molecule inhibitors targeting each Protein Tyrosine Kinase Disease Associated Genetic Mutation Small Molecule Inhibitor Bcr-Abl chronic myeloid leukemia (CML) Translocation between chromosome 9 and 22 Imatinib (Gleevec); acute lymphoblastic leukemia (ALL) Dasatinib; Nilotinib NPM-ALK Nucleophosmin- Anaplastic Lymphoma Kinase ALK anaplastic large-cell lymphomas (ALCL) Translocation between chromosome 2 and 5 neuroblastoma Point mutation in Tyrosine kinase domain acute myeloid leukemia (AML) internal tandem duplication of amino acids in the juxtamembrane (JM) domain Anaplastic Lymphoma Kinase FLT3 Fms-Like Tyrosine Kinase 3 TAE684 PKC412 or a point mutation in the activating loop FGFR3 multiple myeloma (MM) Fibroblast Growth Factor Receptor 3 Translocation between chromosome 4 and 14 CHIR258 The small molecules developed against each of the four PTKs are in different stages of the drug development process. They have been shown to be effective at PTK inhibition in several assays, bringing hope to patients waiting for suitable treatments. However, some of these small molecules are under preclinical investigation, and more tests and clinical trials need to be conducted before they are proven safe and efficacious in humans. There are various challenges that need to be overcome, such as undesirable absorption profile, low drug level at the therapeutic site due to the presence of efflux proteins, and secondary resistance that arises from PTK mutations. The treatment and prevention of cancer requires an enormous effort from the scientific community and health care professionals. Continuing studies on small molecule inhibitors of PTKs will lead to new understandings of critical signalling pathways and certainly more breakthrough therapies for the treatment of cancer. .References 1. Blume-Jense, P. and T. Hunter, Oncogenic kinase signalling. Nature, 2001. 411: p. 355–365. 3. Kurzrock, R, et al., The molecular genetics of Philadelphia chromosome positive leukemias. N Engl J Med, 1988. 319: p. 990-998. 4. Cardama, A, and J. Cortes, Molecular biology of bcr-abl1-positive chronic myeloid leukemia. Blood, 2009. 113: p. 1619-1630. 5. Mauro, M.J., et al., ST1572, a tyrosine kinase inhibitor for the treatment of chronic meylogenous leukemia: validating the promise of molecularly targeted therapy. Cancer Chemother Pharmacol, 2001. 48(suppl 1): p. S77-78. 6. Bunchdunger, E., et al., Inhibition of the Abl protein-tyrosine kinase in vitro and in vivo by a 2-phenylaminopyrimidine derivative. Cancer Res, 1996. 56: p. 100-104. 7. Druker, B.J., et al., Activity of a specific inhibitor of the BCR-ABL tyrosine kinase in the blast crisis of chronic myeloid leukemia and acute lymphoblastic leukemia with the Philadelphia chromosome. N Engl J Med, 2001. 344(14): p. 1038-1042. 9. Talpaz, M., et al., Dasatinib in imatinib resistant philadelphia chromosome positive leukemias. N Engl J Med, 2006. 354(24): p. 2531-2541. 10. Kantarijian, H.M., et al., Nilotinib (formerly AMN107), a highly selective Bcr-Abl TK inhibitor is effective in patients with philadelphia chromosome positive chronic myelogenous leukemia in chronic phase following imatinib resistance and intolerance. Blood, 2007. 110(10): p. 3540-3546. 11. Tiwari, A.K., et al., Nilotinib (AMN107, Tasigna) reverses multidrug resistance by inhibiting the activity of the ABCB1/Pgp and ABCG2/BCRP/MXR transporters. Biochem Pharmacol, 2009. 78(2): p.153-161. 12. Thiesing, J.T., et al., Efficacy of ST1571 and abl tyrosine kinase inhibitor in conjunction with other antileukemic agents against bcr-abl positive cells. Blood, 2000. 96 (9): p. 3195-3199. 13. Benharroch, D., et al., ALK positive lymphoma: single disease with broad morphology. Blood, 1998. 91(6): p. 2076-2084. 14. Morris, S.W., et al., Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science, 1994. 263: p. 1281-1284. 15.George, E.R., et al., Activating mutations in ALK provide a therapeutic target in Journal of Undergraduate Life Sciences Volume 4 • No. 1 • Spring 2010 2.Ghose, A.K., et al., Knowledge based prediction of ligand binding modes and rational inhibitor design for kinase drug discovery. Journal of Medicinal Chemistry, 2008. 51(17): p. 5149-5170. 8. Shah, N.P., et al.,Overriding imatinib resistance with a novel abl kinase inhibitor. Science, 2004. 305(16): p. 399-401. 5 neuroblastoma. Nature, 2008. 455(16): p. 975-978. 16. Galkin, A.V., et al., Identification of NVP-TAE684, a potent, selective, and efficacious inhibitor of NPM-ALK. PNAS, 2007. 104(1): p. 270-275. 17. Naoe, T., et al.,FLT3 tyrosine kinase as a target molecule for selective antileukemia therapy. Cancer Chemother Pharmacol, 2001. 48(suppl 1): p. S27-S30. 18. Stone, R.M., et al., Patients with acute myeloid leukemia and an activating mutation in FLT3 respond to a small-molecule FLT3 tyrosine kinase inhibitor, PKC412. Blood, 2005. 105: p. 54-60. 19. Weisberg, E., et al., Inhibition of mutant FLT3 receptors in leukemia cells by the small molecule tyrosine kinase inhibitor PKC412. Cancer Cell, 2002. 1: p. 433-443. 20. Chesi, M., et al., Frequent translocation t(4;14)(p16.3;q32.3) in multiple myeloma is associated with increased expression and activating mutations of fibroblast growth factor receptor 3. Nature Genetics, 1997. 16: p. 260-264. 21. Trudel, S., et al., CHIR-258, a novel, multitargeted tyrosine kinase inhibitor for the potential treatment of t(4;14) multiple myeloma. Blood, 2005. 105: p. 2941-2948. 22. Xin, X., et al., CHIR-258 is efficacious in a newly developed fibroblast growth factor receptor 3-expressing orthotopic multiple myeloma model in mice. Clinical Cancer Res, 2006. 12(16): p. 4908-4915. 23. Canadian Cancer Society/National Cancer Institute of Canada. Canadian Cancer Statistics 2008. 2008. 6 Journal of Undergraduate Life Sciences