Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
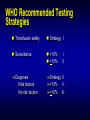
HIV Testing CDC power point edited by M. Myers Message There are numbers of tests They should be used in combination (strategies) Combinations must be consistent Laboratory Tests diagnosis of infection acute, recent, established or late stage disease prognostic markers monitoring of ARV therapies immunological and virological markers toxicities diagnosis of opportunistic infections drug resistance testing ‘typical’ primary HIV-1 infection symptoms symptoms HIV proviral DNA HIV antibodies ‘window’ period HIV viral load HIV-1 p24 antigen 0 1 1° infection 2 3 weeks 4 5 6 / 2 Time following infection 4 6 years 8 10 HIV Assays: Methodologies FOR THE DIAGNOSIS (DETECTION) Virus Detection EIA Simple, rapid tests Immunoblots Antibody Antigen Detection Incident assays DNA (RNA) + HIV Testing Direct Detection of Virus HIV antigen– serology - In isolation - Diagnosis of primary infection viraemia Virus culture / isolation Nucleic acid detection - (NAT) Clinical uses Proviral DNA vs. plasma RNA (viral load) resolution of inconclusive serology / neonatal subtyping drug resistance monitoring Available Assays EIAs including rapid, simple particle agglutination, dot/blot Western blot Antigen & Ab/Ag Incidence assays Direct Virus Detection Particle Agglutination Western Blot Expensive – $ 80 - 100 technically more difficult visual interpretation lack standardisation - performance - interpretation - indeterminate reactions – resolution of ?? ‘Gold Standard’ for confirmation Antibody testing limitations Difficulties in interpretation Limitations - ‘window period’ antibodies appear within 3-4 weeks Direct detection – HIV p24 antigen or DNA/RNA (NAT) – pre-antibody Combo test = earlier detection Primary infection + therapy = delayed antibody response Ag/Ab Combo tests Ab & Ag Ag & Ab Detection of Ag & Ab in a single test utility in primary infection – preseroconversion ‘window period’ Incident populations – ‘at risk’ Blood bank Automated platforms available Issues with Combo Assays Testing strategies False reactivity rates Confirmation strategies Replacement of other assays (especially in the USA) Cost Legal issues What about simple assays? HIV Determine test Detect HIV-1 & HIV-2 Cannot differentiate Procedural control – anti Hu IgG Whole blood or serum/plasma Widely available No additional reagents required Room temperature storage 15 minutes to result BioRad HIV-1/2 Multispot Detects HIV-1 and HIV-2 Will differentiate 1 and 2 Procedural control – anti-Hu IgG Serum / plasma only Additional reagents (included) Requires refrigerated storage ‘Immunoconcentration’ principle 15 minutes to result WHO Recommended Strategies Strategy I Test all samples with one EIA Strategy II Strategy I with all reactives retested in a more specific test with different principle and/or antigen. Strategy III Strategy II with reactives tested in a third test differing from the first two tests. WHO Recommended Testing Strategies Transfusion safety Strategy I Surveillance >10% <10% Diagnosis Risk factors No risk factors Strategy II >10% II <10% III I II Testing Strategies AIM: To develop the logic used in establishing the use of HIV tests (testing strategies) Objectives of Testing Strategies To achieve the correct diagnosis in the most efficient manner To maintain consistency in testing To know the predictive value of the testing process To develop baseline data for assessing changes To deliver useful results Aims in Developing HIV Testing Strategies To arrive at the correct sero-diagnosis To minimise total testing; thus cost Minimise samples classed as indeterminate or dual reactors Detect HIV-1 negative but HIV-2 positive Follow likely seroconverters (HIV-1 or -2) Screening Assays Are used to detect antibody-- specific or nonspecific Are designed to handle large numbers of samples with rapid throughput Must be high performance Should include a full range of HIV antigens Serological Testing Strategy SCREENING TEST, highly sensitive NEG REACTIVE SUPPLEMENTAL TEST, highly sensitive & higher specificity POS NEG IND POS ADDITIONAL TESTS NEG IND HIV Testing Strategy HIV1/2 SCREEN NEG REACTIVE POS HIV-1 WB NEG IND POS ADDITIONAL TESTS NEG IND POINT OF REPORTING Supplemental Assays Range of assays that further define sero-status High Performance (higher specificity) The Use of Screening Assays Define samples as negative for a given analyte Enable high throughput Predictive Values Positive Predictive Values: The likelihood of a sample identified as a reactive by a test being truly POSITIVE for the analyte used as the basis of the test. PPV = True Positives X 100% True Positives + False Reactives Predictive Values Negative Predictive Values: The likelihood that a sample identified as a nonreactive by a test is truly NEGATIVE for the analyte used as the basis of the test. NPV = True Negatives X 100% True Negatives + False Negatives WHO Recommended Strategies Strategy I Test all samples with one EIA Strategy II Strategy I with all reactives retested in a more specific test with different principle and/or antigen. Strategy III Strategy II with reactives tested in a third test differing from the first two tests. WHO Recommended Testing Strategies Transfusion safety Strategy I Surveillance >10% <10% Diagnosis Risk factors No risk factors Strategy II >10% II <10% III I II WHO Guidelines Other possibilities strategy for confirmation combination of affordable & simple assays different test principles different antigen preparations two or three ELISAs or rapid tests diagnosis confirmed by second sample detection of virus (PCR) antigen detection (limited lab.facilities) Always use a QC sample Cost of HIV Testing comparative costs ELISA (Ab only) - $2 per test EIA (Ab/Ag combo) - $3.50 rapid test - $10-20 per test Western blot $80 - 100 p24 antigen $30 PCR - qualitative $80 - 100 PCR - quantitative (viral load) $90 – 150* DNA sequencing (resistance) $400 – 700 Summary of Testing Strategies Screening test x1 Eliminates laboratory error R Screening test x2 RR or R- POS + Supplemental test Other tests NEG - NEG NEG