Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
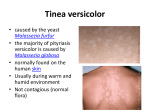
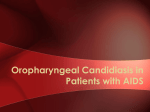
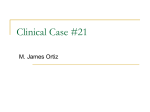
Yeast infection of the Skin Dr. Ahmed A. Kawen Dermatology & Venereology Pityriasis Versicolor It is a common fungal skin infection. The old name, tinea versicolor, should be dropped, as the disorder is caused by commensal yeasts (Pityrosporum) and not by dermatophyte. Cause: Pityriasis versicolor is caused by the dimorphic organism (Malassezia), which is the pathogenic form of the commensal yeasts (Pityrosporum). It is a lipophilic organism (presents in highest number in areas with increased sebaceous activity). P. versicolor Recent researches has shown that, the genus Malassezia includes 12 species, all these species are lipophilic except M. pachydermatis is non lipophilic. The majority of pityriasis versicolor is caused by Malassezia globosa, while the classical old species is Malassezia furfur. Predisposing factors: Cushing syndrome, pregnancy, OCP, malnutrition, corticosteroid therapy, heat, and humidity; cause the Pityrosporum to convert to its pathogenic form (Malassezia). Presentation and course: The disease mostly seen in adolescent and young adult (age of high sebaceous activity) and rare in children, and mostly occur in summer months. Typical sites are the upper trunk; neck, chest, upper back, & shoulders (areas with high sebaceous activity). P. versicolor ●It presents as asymptomatic or slightly itchy, scaly, hypopigmented (in dark skin) or hyperpigmented (in white skin) macules (so termed versicolor). The scales are accentuated by stretching. ●The infectivity of the disease is very low and can be regarded as non-infectious. ●Mechanisms of pigmentary change are unclear; darkening may result from hyperkeratosis, but lightening result from direct inhibitory effect on melanocytes by the carboxylic acids which is released by the organisms Tinea Versicolor More apparent in the summer. Tinea Vesicolor Hyperpigmented Variety Looks Like: intertrigo, erythrasma …. Diagnosis: •Scrape lightly – fine white scale •KOH Positive for short hyphae and spores (Spaghetti and meatballs) •Woods Light – pale yellow white fluoresce. •Culture rarely done. Tinea Vesicolor – Woods Light Yellow White Tinea Versicolor Microscope P. Versicolor - Differential •Vitiligo •Pityriasis Alba •Pityriasis Rosea Vitiligo White without scale. Pityriasis Alba Frequently on face, KOH neg. Few lesions. May have fine white scale. Pityriasis Rosea •Papules or plaques with Collarette of scale, KOH (-), Woods light neg. Treatment: Topical: it is indicated for limited disease, treatment options include: 1- Imidazole (miconazole, clotrimazole, and ketoconazole) cream, twice daily for 2–4 weeks. Ketoconazole shampoo for 5-10 minutes daily for 3 days. 2- Selenium sulphide suspension or shampoo for 10 minutes daily for one week. 3-Terbinafine spray. 4- Recently Iraqi researches proved that lactic acid solution and diclofenac gel are effective alterative therapies. Systemic Treatment Indicated for extensive or resistant infection or frequent recurrences, include: - Itraconazole (200 mg once daily for one week), -fluconazole (400 mg single dose), -or ketoconazole (400 mg single dose). - P. Versicolor-Treatment Notes : - Hypopigmentation resolves slowly -No scale when scraped indicates cure. -Sunlight helps restore pigment •Prevention: recurrence is common after any treatment, so it may be prevented by: once weekly application of ketoconazole shampoo or Selenium shampoo’s prophylaxis before summer in some patients or once monthly oral itraconazole, fluconazole, or ketoconazole for 6 months. Introduction Pityrosporum folliculitis : Is a common inflammatory skin disorder that is seen mainly in young adult person. Its an infection of the hair follicle that is thought to be caused by the common cutaneous lipophilic yeast like fungus, Malassezia furfur . The disease is often misdiagnosed as truncal acne so that traditional acne therapies, especially antibiotics, worsen PF. Diagnosis of pityrosporum folliculitis(PF):Depends on the following criteria :- 1-characteristic morphological picture: The rash of pityrosporum folliculitis is dimorphic, with pruritic erythematous follicular papules and pustules. affecting mainly the upper back and some time adjacent areas are involved. 2- Positive Wood’s light examination. 3- Positive Direct microscopical examination. 4-Skin biopsy stained with PAS stain positive for pityrosporum. 5-prompt response to the antifungal drugs. Differential diagnosis of pityrosporum folliculitis: - Truncal acne:-differentiated from PF by the following : -Lesions of acne are polymorphic with presence of comedones, cysts or scars. -The distribution of truncal acne on the back (affect mostly the periphery). -Presence of other acne lesion elsewhere (e.g. face) . - Absence of itching. -Failure of response to the antifungal treatments. -Bacterial folliculitis. -Steroid –induced folliculitis . -Pustular drug eruption . patient with Pityrosporum folliculitis: Before treatment with antifungal. patient with truncal acne: After treatment with antifungal.. Candidiasis(Candidosis or Moniliasis) C. albicans is a common inhabitant of the gastrointestinal and genitourinary tracts, and skin C. albicans is an opportunistic organism. Under the right conditions e.g. decreased immunity, moisture and decreased competing flora, It can cause lesions of the skin, nails, and mucous membranes Predisposing factors: 1- Mechanical factors: local occlusion, moisture and/or maceration, dentures, occlusive dressings, and obesity. 2- Nutritional factors: iron deficiency, and malnutrition. 3- Physiologic alterations: extremes of age, and pregnancy. 4- Systemic illnesses: endocrine disease (diabetes mellitus, cushing disease), malignancy, and immunodeficiency. 5- Iatrogenic: catheters and medications (steroid, broad spectrum AB, and OCP). Presentation of Candidiasis primary lesion is a red pustule. Most Common: pustules dissect horizontally through the stratum corneum leaving a red, glistening denuded surface with long continuous border with satellite lesions. Clinical pictures; 1. 2. Oral candidiasis; thrush & perleche. Cutaneous candidiasis; – – – 3. 4. Intertrigo. Erosio-interdigitalis blastomycetica. Paronychia. Genital candidiasis; Systemic candidiasis; Oral Candidasis Oral candidiasis (Thrush) The mucous membrane of the mouth may be involved in healthy infant In the newborn the infection may be acquired from contact with the vaginal tract of the mother Types of thrush (1)Pseudomembranous Candidiasis (Thrush): White-to-creamy plaques on any mucosal surface. Removal with a dry gauze pad leaves an erythematous mucosal surface. Can involve dorsum of tongue, buccal mucosa, hard/soft palate, pharynx, esophagus. (2) Erythematous (Atrophic) Candidiasis: Smooth, red, atrophic patches(atrophic papillae) (3) Hyperplastic candidiasis: white plaques that cannot be wiped off. It is often the first manifestation of AIDS. Thrush Oral candidasis Angular Cheilitis(Perleche) White plaques with slight erythema of the mucous membrane at the angles of mouth. Maceration and fissures may be present Is commonly related to C.albicans, but may be caused by coagulasepositive S. aureus and Gramnegative bacteria. Similar changes may caused by nutritional deficiency e.g. riboflavin and iron. Angular cheilitis Genital candidiasis: A- Vulvovaginitis: white curdy plaques adherent to the inflamed mucous membranes, and a whitish discharge. The eruption may extend to the groin folds. Overgrowth of candida can cause the labia to be erythematous, moist. There might be e pruritus, burning and curd-like discharge Pregnancy, high-dose estrogen and longterm tamoxifen treatment are a predisposing factors About 20% of asymptomatic women are vaginal carriers. During pregnancy, this rises to 40% Candidiasis can be sexually transmitted and this is probably most important in recurrent infections B-Balanitis and Balanoposthitis in males similar changes occur under the foreskin, and on the glance. Balanitis is more common in the uncircumcised man The skin is erythematous and glazed with pustules and erosions Candidal intertrigo Flexural candidiasis: Can involve groins or armpits; intergluteal cleft; under large breasts; under overhanging abdominal folds; or in the umbilicus. Red moist patches surrounded by a fringe of macerated epidermis (“collarette” scale). Tiny pustules and papules are observed closely adjacent to the patches, termed “satellite or daughter” lesions A moist glazed area of erythema and maceration appears in a body fold; the edge shows soggy scaling, with outlying satellite papulopustules. These changes are most common in the groin, axillae, or under the breasts. Napkin candidiasis: it is a type of flexural candidiasis, occurs usually due to occlusion by wet diapers, and misuse of steroid combination compounds (as nystacort, which contain potent steroid and weak antifungal agents). Intertrigo Intertrigo ddx Differentiated from contact dermatitis by: (1) Involvement of the folds (2) Occurrence of many small erythematous “satellite” or “daughter” lesions scattered along the edges of the larger patch(es) Rx: Topical anticandidal agents are effective. Recurrent cases may be associated with gut colonization and need Rx with oral nystatin Perianal candidiasis May present as a pruritus ani Pruritus and burning can be very severe Characterized by erythema, maceration and less commonly fissure Rx: topical anticandidal agents are effective. Oral antifungals are alternative Paronychia: Candida albicans may be the sole pathogen in chronic paronychia, or be found with other micoorganisms as Proteus or Pseudomonas. The proximal and sometimes the lateral nail folds of one or more fingers become bolstered and red and the cuticles are lost. Mostly seen in house wife (water and detergent exposure). Acute paronychia is usually bacterial (staph. aureus). Candidal nail infection: generally results from candidal paronychia and starts near the nail fold. The nail plate becomes ridged and yellow. Usually the fingernails are affected more than toenails Patients commonly have an atopic background Frequently seen in diabetics and those with heavy hand work Erosio interdigitalis blastomycetica Oval shaped macerated white area on the finger webs, mostly the third web between the middle and ring finger. Mostly seen in diabetic patients, or in persons with frequent water exposure of their hands. On the feet it is the fourth web space that is most often involved Clinically, this may be indistinguishable from tinea pedis Erosio-interdigitalis blastomycetica - Chronic mucocutaneous candidiasis: It is a chronic, treatment-resistant, candidal infections of the skin, nails, and mucous membranes. There are specific inherited abnormalities in cell-mediated immunity,several different forms have been described including those with autosomal recessive and dominant inheritance patterns. Chronic mucocutaneous candidiasis: Systemic candidiasis: This is seen against a background of severe illness, leucopenia or immunosuppression. The skin lesions are begin as erythymatous macules that may become papular, nodular, pustular, or ulcerative. Investigations: 1- KOH examination: candida appears as oval cells (yeast), and sometimes as elongated cells (pseudohyphae). 2- Culture: Sabouraud's Dextrose Agar. 3- Investigations for the suspected predisposing factors. ●Wood's light is not useful in all types of candidal skin infection. Treatment: General measures: Predisposing factors should be sought and eliminated. Topical: Imidazole group (miconazole, clotrimazole, and ketoconazole), amphotericin, nystatin, and gention violet, all are effective topically. Systemic Oral itraconazole (twice daily) or fluconazole (once weekly) can be used, they are indicated for: 1- Recurrent candidiasis in immunocompromised. 2- Sever or recurrent genital infection. 3- Candidal paronychia and nail infections. 4- Chronic mucocutaneous candidiasis. 5- Systemic candidiasis. THANK YOU