Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
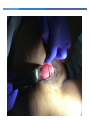
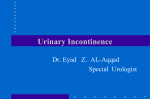
Stephen T Jeffery University of Cape Town, South Africa Urogynaecology and laparoscopy clinic www.urogynaecology.co.za Impact of Pelvic Floor Dysfunction Very different from the experience in well resourced settings. Heaviest burden is in the prevailing problem of obtsetric fistula. Let’s kick off with a few typical cases Case 1 • 56 year old • Complains of urgency, urgency incontinence daily episodes • Also incontinence with coughing, laughing and sneezing • On exam – obvious stress leak with cough Case 1 Options? Case 1: If she was living in Chicago / London / Paris For the urgency incontinence Bladder retraining by specialist continence nurse Pelvic floor exercises by women’s health physiotherapist Trial of anticholinergic therapy including tolteridine, solifenacin, oxybutynin slow realease, mirabregnon Possibly Intradetrusor Botox Poterior tibial nerve stimulation Sacral Nerve Stimulation Case 1: If she was living in Chicago / London / Paris For the stress incontinence Tension –free vaginal or transobturator tape Case 1: If she was living in Accra / Kathmandu/ For the urgency incontinence May have some advice about PFE / Bladder drill / Fluid advice May get some Oxybutynin Case 1: If she was living in Accra / Kathmandu/ For the stress incontinence Depends on training Possibly have a Burch / Pubovaginal sling No option of a TVT or TOT Case 1: If she was living in Accra / Kathmandu/ AND would she even have sought help for this problem? Case 2 21 year old Constant urinary leakage Delivered a macerated, dead baby at home 6 months ago Case 2 Case 3: Only likely to see in resource constrained setting Case 4: Prolapse Urinary Incontinence Fecal Incontinence Other common referral problems • Hematuria • Recurrent UTIs • Bladder pain syndrome • Sexual dysfunction/dyspareunia • Pelvic pain • Defecatory difficulty • Obstructed defecation The most staggering statistics are the related to fistula Pelvic Floor Health in Resource Constrained Settings Under-reported Under-diagnosed Undertreated Significant direct and indirect costs First of all – get the basics right Approach • Important symptoms: Urinary incontinence Stress Urgency / urgency incontinence Nocturia Leakage with sex How many pads Symptoms of voiding dysfunction Medications: Look for diuretics and Beta blockers Approach • Red flag symptoms – Voiding difficulties – Haematuria – Severe bladder pain Prolapse related queries Does the bulge protrude through the introitus? How big is it in relation to known objects such as a golf ball, egg, lemon, orange? How exactly is the problem BOTHERING her? What are her fears about the bulge? What are her expectations for treatment? Approach Faecal symptoms Faecal Urgency Faecal Incontinence Defaecatory difficulty Change in bowel habit Bleeding Straining and digitation Distinguishing between flatus and solid stool Rectal prolapse Approach Sexual Dysfunction Approach • General Medical History – Multiple sclerosis – Parkinsons – Stroke – Risk factors for surgery Approach •Surgical History – Previous incontinence/ prolapse surgery? – Does she still have a uterus? – Previous gynaecological surgery? Neuro Exam S2, S3, S4 nerves – peri-anal skin Decreased ankle reflexes – SCI or Cauda Equina Abdomen Ileal disease – RLQ (Crohns) Abdominal mass Don’t only zoom in on the vagina Fistula Skin Irritation Digital Rectal Exam Squeeze Some correlation with manometry Case • 45 year old with Stage III vaginal vault and rectal prolapse. She is sexually active. • Total Vaginal Length is 8 cm • What options would you present to this patient? Urine dipstix • Pyuria UTI is an important cause of urgency • Glycosuria DM – Peripheral autonomic neurop, UTI • Haematuria Bladder Ca Bladder diary Don’t forget the bladder diary Don’t forget the bladder diary Check Urine Residual Catheter Or Ultrasound Cheap “cystometry” (acknowledgements to Lauri Romanzi) Cheap “cystometry” (acknowledgements to Lauri Romanzi) 1 Position patient in lithotomy, with head raised if possible 2 Separate labia, STAND TO THE SIDE, as pt strains, then coughs – note presence/absence SUI, record data 3 Clean meatus with Betadine 4 Insert red rubber catheter use lubricant 5 Empty bladder, record volume Cheap “cystometry” (acknowledgements to Lauri Romanzi) 6 Evaluate urine for infection (dipstick, visual inspection) & record findings – defer filling if infected 7 Invert catheter & attach 60 ml catheter tip syringe 8 Fill bladder via gravity in 50 ml increments using normal saline 9 Note volume at which patient reports 1st urge, moderate fullness, total fullness 10 Evaluate filling phase for presence/absence involuntary bladder contractions (detrusor instability) record findings Cheap “cystometry” (acknowledgements to Lauri Romanzi) ⑪ At capacity, remove catheter and have patient strain (Valsalva) & cough again – record presence/absence SUI ⑫ If patient does not demonstrate SUI supine, repeat strain & cough in standing position, record presence absence SUI ⑬ Have patient void into container – record audible characteristics of flow, volume voided, & calculate post-void residual (PVR) Treatment options for stress and urge urinary incontinence, prolapse Supporting Pelvic floor physiotherapy • pessaries, tampon • Pelvic floor reeducation • incontinence pads • Kegel exercises • Biofeedback Behavioral intervention • reducing fluid intake Surgical therapy • prevent intoxications (coffee etc) • mid-urethral slings • bladder training • colposuspension • cough technique • bulking agents • reduction of weight • prevent psychological and somatic stress situations • Prolapse surgery Drug therapy No therapy • Anti-cholinergics, α-sympaticomimetics • ??? • Fistula surgery • Estrogen 55 Inexpensive treatment options Basic fluid advice Group physio therapy sessions Anticholinergics Always worth trying Oxybutynin If you can’t afford second line anticholinergic therapy, don’t worry – most of them don’t really work! Persistence on Specific Medications for OAB Based on Prescription Data Cheap posterior Tibial Nerve Stimulation Pessaries Pessaries Follow up 6 monthly Clean and re-insert each time No need to replace with new one Other essential tools of the trade Identify keen doctors and support them Don’t underestimate the power of energy and enthusiasm! Training, training, training! Identify your specific challenges Lack of training Lack of resources No patients Anaesthesia Radiological investigations Competing interests Oncology Obstetrics Emergency gynae Build your team Urologist Colo-rectal Physio Nurses www.urogynaecology.co.za www.urogynaecology.co.za