Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
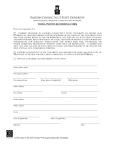
Union City Evolution PLAYER AUTO-BIOGRAPHY: TEAM: PLAYER NAME: _________________________ BOYS: 8U 12U 9U 13U 10U 11U 14U JV/VARSITY NICKNAME GIRLS:_____________ AGE:_____ HEIGHT:_________ WEIGHT:_________ POSITION:__________________________ ADDITIONAL SPORTS: ___________________ PREFERRED FUTURE COLLEGE:______________________ Parental Consent, Release and Liability Waiver Form for Publication Please check one and sign below. I give permission for photographs,digital images, and all information enclosed on above auto-biography form of my child to be used without compensation by the Union City Evolution Organization in Union City, CA for Web pages, advertising and/or promotional purposes. By signing below, I am expressly releasing the Union City Evolution Organization, its affiliates, employees, licensees and assignees from any and all claims which I may have for invasion of privacy, right of publicity, defamation, copyright infringement, or any other causes of action arising out of the use, adaptation, reproduction, distribution, broadcast or exhibition of such photographs and digital images. I do not give permission for photographs, digital images, and all information enclosed on above autobiography form of my child to be used by the Union City Evolution Organization in Union City, CA for Web pages, advertising and/or promotional packages. Printed Name of Player:____________________ Printed Name of Parent or Guardian:___________________ Signature of Parent or Guardian:__________________________ Date:________________________