Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
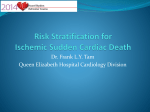
PRIMARY PREVENTION PATIENTS SIMILAR TO SECONDARY PREVENTION PATIENTS Shu Zhang¹, Jeff Cerkvenik², Sarah Willey², Diego Rodriguez Guerrero 3 , Alexandr Robertovich Chasnoits4, Balbir Singh5, Azlan Hussin6, Chi Keong Ching7, Dejia Huang8, Yen-Bin Liu9, Young-Hoon Kim10 1 Fuwai Cardiovascular Hospital, Beijing, China, 2Medtronic, Minneapolis, Minnesota, USA, 3Instituto de Cardiología - Fundación Cardioinfantil, Bogota, Colombia, 4Republican Scientific Practical Centre Cardiology, Minsk, Belarus, 5Medanta, The Medicity Hospital, Gurgaon, Haryana, India, 6Institut Jantung Negara, Kuala Lumpur, Malaysia, 7National Heart Centre of Singapore, Singapore, Singapore, 8 West China Hospital, Chengdu, China, 9National Taiwan University Hospital, Taipei City, Taiwan, 10 Korea University Medical Center, Seoul, Korea Purpose: Primary prevention (PP) ICD therapy is underutilized relative to secondary prevention (SP) ICD therapy. While ICDs provide a mortality benefit in PP ICD patients, these patients may be at lower risk of ventricular arrhythmias relative to SP patients. We set out to find a subgroup of PP patients who resembled SP patients. Methods: The US OMNI ICD registry was used for this analysis. A subgroup of the PP group of patients (Group 1.5) potentially more likely to benefit from ICDs was identified based on history of non-sustained ventricular tachycardia (NSVT) and left ventricular ejection fraction (LVEF) < 25% at implant. Time to first appropriately treated VT/VF event was the endpoint of interest and hazard ratios were used to compare Group 1.5 to SP patients. Results: The OMNI study included 2,242 ICD/CRT-D patients with known indication, of which 1,894 were PP. Within the PP group, 52% were in Group 1.5. Results over 4+ years (Figure) show a significant difference (p<0.01) in appropriately treated VT/VF between primary and SP groups. However, when comparing the Group 1.5 subset of PP patients to the SP patients, there was not a statistically significant difference (p=0.38), with a hazard ratio of 0.91 (95% c.i.: 0.73-1.13). Conclusion: Primary prevention patients with a history of NSVT or low LVEF (<25%) have a similar rate (within 9%) of appropriate ICD therapies as secondary prevention patients. These results suggest that this subset of primary prevention patients have similar risk of arrhythmias as patients who have previously experienced a documented life threatening ventricular arrhythmia.