Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
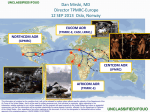
Overview International Health Regulations (IHR 2005) LtCol. Sam Barringer, DVM United States Air Force Academy UNCLASSIFIED UNCLASSIFIED Overview "As we have seen recently with SARS and H5N1 avian influenza, diseases respect no boundaries. In today's world, a threat anywhere means danger everywhere.“ (December 13, 2006) --HHS Secretary Michael O. Leavitt, on occasion of official United States acceptance of revised IHR UNCLASSIFIED Background Purpose of the WHO International Health Regulations 2005 …to prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade (IHR 2005, Article 2). Homeland Security Presidential Directive HSPD-21 Calls on HHS to "establish a national biosurveillance system for human health, with international connectivity where appropriate, that is predicated on State, regional, and communitylevel capabilities and creates a networked system to allow for two-way information flow between and among Federal, State, and local public health authorities and clinical health care providers." Strategy submitted to Homeland Security Council October 31, 2008 UNCLASSIFIED IHRs History • During the Forty-Eighth World Health Assembly in 1995, WHO and Member States agreed on the need to revise the IHR (1969). The revision of IHR (1969) came about because of its inherent limitations, most notably: • Narrow scope of notifiable diseases (cholera, plague, yellow fever). The past few decades have seen the emergence and re-emergence of infectious diseases. The emergence of “new” infectious agents Ebola Hemorrhagic Fever and the reemergence of cholera and plague in South America and India, respectively; • Dependence on official country notification; and • Lack of a formal internationally coordinated mechanism to prevent the international spread of disease. • These challenges were placed against the backdrop of the increased travel and trade characteristic of the 20th century. • The IHR (2005) entered into force, generally, on 15 June 2007, and are currently binding on 194 countries (States Parties) across the globe, including all 193 Member States of WHO. UNCLASSIFIED Recent Outbreaks From WHO World Health Report 2007 UNCLASSIFIED IHRs: Key Changes from 1969 • Notify WHO of events meeting defined criteria – beyond prescribed list • Enhance their events management – especially alert and response actions • Meet minimum core capacities – notably in surveillance, response, and at points of entry UNCLASSIFIED UNCLASSIFIED IHR Purpose The World Health Organization’s IHRs are legally binding regulations that form international law which aim to: a) assist countries to work together to save lives and livelihoods endangered by the spread of diseases and other health risks, and b) avoid unnecessary interference with international trade and travel. UNCLASSIFIED UNCLASSIFIED IHRs: Serves a Common Interest • Serious and unusual disease events are inevitable. • A health threat in one part of the world can threaten health anywhere or everywhere. • Provides a formal code of conduct: – helps contain or prevent serious risks to public health – discourages unnecessary or excessive traffic or trade restrictions, for "public health purposes" UNCLASSIFIED UNCLASSIFIED IHRs: Serves a Common Interest • International agreement giving rise to international obligations • Focuses on serious public health threats with potential to spread beyond a country′s borders, to other parts of the world • Such events are defined as a Public Health Emergency of International Concern (PHEIC) • Outlines assessment, management, and information sharing for PHEICs UNCLASSIFIED UNCLASSIFIED IHRs: In Brief • ARE – Written in legal language – Supported by guidelines to aid compliance – Intended to contain public health threats and minimize economic disruption • ARE NOT – Self—explanatory – Recommendations for safe travel – A scientific consensus on everything possible to prevent disease spread UNCLASSIFIED UNCLASSIFIED IHRs: Notifiable Diseases ALWAYS Notifiable: – Smallpox – Poliomyelitis, wild—type – Human influenza, new sub—type – Severe Acute Respiratory Syndrome (SARS) UNCLASSIFIED UNCLASSIFIED IHRs: Notifiable Diseases Other Potentially Notifiable Events: – Examples: cholera, pneumonic plague, yellow fever, viral hemorrhagic fever, and West Nile fever – Other biological, radiological, or chemical events may fit the decision algorithm and be reportable UNCLASSIFIED UNCLASSIFIED WHO Pandemic Phases UNCLASSIFIED UNCLASSIFIED Making the Determination • • • • Is the public health impact of the event serious? Is the event unusual or unexpected? Is there a significant risk of international spread? Is there a significant risk of international travel or trade restrictions? WHO makes the final determination that a Public Health Emergency International Concern exists UNCLASSIFIED UNCLASSIFIED Serious Implication on Public Health? • There is potentially high morbidity and/or mortality • The geographic scope is large or spreading over a large area (e.g. multi—state or regional); is in area of high population density • The agent is highly transmissible/pathogenic • The event has compromised containment or control efforts • Therapeutic/prophylactic agents are unavailable, absent, or ineffective • Cases occurring among health care staff • Assistance for investigation & response required UNCLASSIFIED UNCLASSIFIED Unusual or Unexpected? • The disease—causing agent is yet unknown or a new (emergent) pathogen • The population affected is highly susceptible • The affected country’s Government is encouraging local and state Governments to aid compliance • The event is unusual for the season, locality or host • There is a suspicion that this may have been an intentional act • Agent had been eliminated or never reported in this country before. UNCLASSIFIED UNCLASSIFIED Significant Risk for International Spread? • Epidemiologic link to a similar event outside the affected country – International travel or gathering – Contact with traveler or mobile population • Potential cross—border movement of pathogen/agent/host • Conducive transmission vehicles: air, water, food or environmental UNCLASSIFIED UNCLASSIFIED Risk for Trade or Travel Restrictions? • There is a history of similar events in the past that have resulted in restrictions • The event is associated with an international gathering or a tourist area • The event is or has gained significant government or media attention • There is a zoonotic disease or the potential for an epizootic event, or exported/imported food/water— related UNCLASSIFIED UNCLASSIFIED Making the Determination In summary … • Local situational assessment required – Decision instrument available • WHO will also assess before any publication or formal response UNCLASSIFIED UNCLASSIFIED Reporting Timeline 48—hour Time Requirement • After a Governmental Agency learns of a potential PHEIC within its state or territory, it must assess the event within 48 hours. 24—hour Time Requirement • The Government Agency has 24 hours to notify WHO after it believes that a potential PHEIC may exist. UNCLASSIFIED UNCLASSIFIED Global Health and IHRs Shared responsibility – to establish core capacities: • Surveillance and response • Points of entry • Country—specific procedures—key element of WHO′s strategy for global health security UNCLASSIFIED UNCLASSIFIED Global Health and IHRs Robust National Response Effort is Expected: • Context—specific • Flexible • Interventional health measures permitted UNCLASSIFIED UNCLASSIFIED Global Health and IHRs Entrance Screening Permissible • Medical exams and interviews • Vaccination and other measures by consent • Quarantine/isolation – respect for human rights UNCLASSIFIED UNCLASSIFIED IHR References • WHO IHR website: http://www.who.int/csr/ihr/en/ • HHS Global Health website: http://www.globalhealth.gov/ihr/ • HHS Announcement the U.S. accepted the IHR (2005): http://www.hhs.gov/news/press/2006pres/20061213.html • CDC IHR website: http://www.cdc.gov/cogh/ihregulations.htm • Baker MG, Fidler DP. Global public health surveillance under the new International Health Regulations. EID; July 2006, Vol. 12. http://www.cdc.gov/ncidod/eid/vol12no07/05-1497.htm • The CDC’s National Notifiable Diseases Surveillance System (NNDSS) notifiable diseases website: http://www.cdc.gov/epo/dphsi/nndsshis.htm • McNabb, Scott J.N., PhD, MS, Kohl, Katrin S., MD, PhD, MPH, International Health Regulations: Revised for Today‘s World, U.S. Centers for Disease Control and Prevention, Coordinating Office for Global Health. Available at http://www.cdc.gov/cogh/ihrMaterial/powerpoint.htm UNCLASSIFIED Any Questions? UNCLASSIFIED