Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
BIOLOGICAL ACTIVITIES OF MEDICINAL PLANTS
TRADITIONALLY USED TO TREAT SEPTICAEMIA IN THE
EASTERN CAPE,
SOUTH AFRICA
By
ROBERT FRED CHINYAMA
Submitted in fulfilment of the requirements for the degree of
MAGISTER TECHNOLOGIAE BIOMEDICAL TECHNOLOGY
in the
Faculty of Health Science
at the
Nelson Mandela Metropolitan University
December 2009
SUPERVISOR:
Dr N. SMITH
CO-SUPERVISOR:
Mrs E. BAXTER
DECLARATION
I, the undersigned, hereby declare that the research work contained in this study is my own
original work, and all the sources I have used or quoted have been indicated and acknowledged
by means of complete references.
………………………………….
i
ABSTRACT
Over the past 25 years, there has been a resurgence of worldwide scientific research in the fields
of ethnopharmacology. The Western world has acknowledged the continued use of traditional
medicines by the majority of third world countries, and the need for novel drug development.
Hence, much of the pharmaceutical research in recent years has focused on the ethnobotanical
approach to drug discovery (Light et al., 2005).
In South Africa, as in most developing parts of the world, traditional herbal medicine still forms
the backbone of rural healthcare. The government health services in South Africa provide only
western medical care although the majority of the population consult traditional healers for some
or all of their healthcare needs (McGaw et al., 2005).
Medicinal plants like Harpephyllum caffrum are used as blood purifiers or emetics (Watt and
Breyer-Brandwijk, 1962), and also for treating acne and eczema. The antimicrobial activity of
this plant can be used to treat septicaemia, which is ranked the sixth leading cause of death
among neonates and the eighth leading cause of death for infants through the first year of life
(Heron, 2007).
In this study, the plants investigated for antimicrobial activity were Harpephyllum caffrum,
Hermannia cuneifolia, Chironia baccifera, Rhigozum obovatum, Felicia muricata and Pentzia
incana. These plants were tested against ATTC (American Type Culture Collection) strains and
microorganisms isolated from clinical isolates of patients suffering from septicaemia. The assay
methods used included the agar diffusion method using the Mast multipoint inoculator, the
microtitre dilution method were used to determine the minimum inhibitory concentration, thin
layer chromatography fingerprints accompanied by bioautographic assay were used to detect the
inhibition of bacterial growth by active compounds separated from plant extracts and the Ames
test was required to assess the possibility of bacterial mutagenesis upon the exposure to plant
extracts which can lead to carcinogenicity.
In agar diffusion method, extracts of Harpephyllum caffrum inhibited nine strains of Candida
albicans, three species of Acinetobacter and four strains of E.faecalis. Extracts of Hermannia
cuneifolia inhibited four strains of B.cereus and three strains of Staphylococcus aureus. Extracts
of Chironia baccifera inhibited one strain of Acinetobacter and five strains of E.faecalis.
ii
Extracts of plants Rhigozum obovatum, Felicia muricata, and Pentzia incana showed no
antimicrobial activity.
In the microtitre dilution method used to determine the minimum inhibitory concentration
(MIC), the results were different from the agar diffusion method. More activity was observed.
Extracts of Harpephyllum caffrum inhibited three strains of E.coli, six strains of S.aureus, three
species of Acinetobacter and one strain of Klebsiella pneumonia. Extracts of Hermannia
cuneifolia inhibited four strains of B.cereus, three strains of S.aureus, two strains of K.oxytoca
and one species of Acinetobacter. Extracts of Chironia baccifera inhibited three strains of
S.aureus, one strain of MRSA, one species of Acinetobacter and one strain of S.haemolyticus.
The MIC values ranged from 0.049 to 6.25mg/ml.
Using the thin layer chromatography fingerprints, bioautography showed the presence of various
inhibitory chemical compounds. Methanol and acetone extracts of Harpephyllum caffrum,
separated very well and showed various inhibition zones on exposure to Candida albicans,
Enterococcus faecalis and Staphylococcus aureus. The different inhibition zones were recorded
as R f values ranging from 0.25 to 0.95. The zones indicate the different inhibiting chemical
compounds present in the plant. Petroleum ether, ethyl acetate, chloroform and formic acid were
the solvents used in the assay in the ratio 8:7:5:1, respectively.
In the Ames test (Maron and Ames, 1983) the methanol and acetone extracts of Harpephyllum
caffrum and Hermannia cuneifolia were negative which means they were devoid of any
mutagenic properties. Methanol extracts of Harpephyllum caffrum showed similar results in the
Ames assay as reported by Verschaeve and Van Staden (2008).
Establishing the antimicrobial activity of these plants contribute to the systematic scientific
investigation of indigenous South African medicinal plants.
iii
ACKNOWLEDGEMENTS
I, the author, would like to express my sincerest gratitude and appreciation to the following
people for their contribution in one way or the other towards the completion of this study.
Dr N. Smith for her patient guidance, encouragement, support and assistance during the duration
of this project.
Mrs E. Baxter for her loving guidance, encouragement, support and instructions throughout the
course of this study. Furthermore, for sourcing medicinal plants every time they were needed.
Mrs L. Beyleveld and Mrs B. Jordan for the ordering of supplies and for their kindness and
support during the study.
The National Research Foundation and Nelson Mandela Metropolitan University for the
financial assistance.
Malawi Union of the Seventh-Day Adventist Church and Malamulo College of Health Sciences
for their sponsorship and financial support during the period of study.
My wife Thandiwe and my children Josephine, Wilson and Yamiko for their unconditional love,
perseverance and endurance during the time when I was away from them.
Finally, I thank the Almighty God, for the good health, wisdom to study and for enabling the
above mentioned individuals to be so kind to me. God’s name be praised.
iv
TABLE OF CONTENTS
DECLARATION ............................................................................................................................. i
ACKNOWLEDGEMENTS ........................................................................................................... iv
TABLE OF CONTENTS .................................................................................................................v
LIST OF FIGURES ..................................................................................................................... viii
LIST OF TABLES ......................................................................................................................... ix
LIST OF ABBREVIATIONS ..........................................................................................................x
CHAPTER 1: INTRODUCTION ....................................................................................................1
1.1 Aim ........................................................................................................................................ 3
1.2 Objectives .............................................................................................................................. 3
CHAPTER 2: LITERATURE REVIEW .........................................................................................4
2.1 Introduction ............................................................................................................................ 4
2.2 Septicaemia ............................................................................................................................ 4
2.2.1 Bacteriology ....................................................................................................................6
2.2.2 Size and shape of bacteria ...............................................................................................6
2.2.3 Mycology ........................................................................................................................7
2.2.4 Prevention, diagnosis and treatment ...............................................................................8
2.2.5 Antibiotic therapy ...........................................................................................................9
2.2.6 Antibiotic resistance......................................................................................................10
2.3 Bacteria and fungi selected for investigation ....................................................................... 11
2.4 Traditional Herbal Medicines .............................................................................................. 11
2.5 Medicinal plants and their importance ................................................................................. 13
2.5.1 Economic importance of traditional medicine ..............................................................16
2.6 Medicinal plants under investigation ................................................................................... 19
2.6.1 Chironia baccifera ........................................................................................................20
2.6.1.1 Active ingredients ................................................................................................. 21
2.6.1.2 Pharmacological effects ........................................................................................ 21
2.6.2 Harpephyllum caffrum ..................................................................................................22
2.6.2.1 Active ingredients ................................................................................................. 22
2.6.2.2 Pharmacological effects ........................................................................................ 23
v
2.6.3 Hermannia cuneifolia ...................................................................................................23
2.6.3.1 Economic and cultural value ................................................................................. 24
2.6.4 Pentzia incana (Karoo bush) ........................................................................................24
2.6.5 Rhigozum obovatum ......................................................................................................25
2.6.5.1 Description ............................................................................................................ 26
2.6.5.2 Distribution ........................................................................................................... 26
2.6.5.3 Derivation of name and historical aspects ............................................................ 27
2.6.5.4 Uses and cultural aspects ...................................................................................... 27
2.6.6 Felicia muricata ............................................................................................................27
2.7 Traditional healers’ beliefs and practices ............................................................................ 27
2.8 Poisonous plants................................................................................................................... 29
2.9 Mutagenic effect .................................................................................................................. 31
2.10 The concept of Western medicine versus Traditional medicine ........................................ 33
2.11 Methods of diagnosis and treatment of disease ................................................................. 34
2.12 Methods of preparation and administration of traditional remedies .................................. 35
2.13 The study area .................................................................................................................... 36
CHAPTER 3: RESEARCH METHODOLOGY ...........................................................................37
3.1 Introduction .......................................................................................................................... 37
3.2 Sampling technique .............................................................................................................. 37
3.3 Plant preparation, extraction and methods. .......................................................................... 38
3.3.1 Preparation ........................................................................................................................ 38
3.3.2 Plant Extraction.............................................................................................................39
3.3.3 Assays ...........................................................................................................................41
3.3.3.1 Agar diffusion method .......................................................................................... 43
3.3.3.2 Determination of minimum inhibitory concentration ........................................... 44
3.3.3.3 Thin Layer Chromatography (TLC) fingerprints .................................................. 45
3.3.3.3.1 Materials and Techniques .............................................................................. 45
3.3.3.4 The Ames test ....................................................................................................... 46
CHAPTER 4: RESULTS ...............................................................................................................48
4.1 Introduction .......................................................................................................................... 48
vi
4.2 Agar diffusion method ......................................................................................................... 48
4.3 Minimum inhibitory concentration (MIC) ........................................................................... 67
4.4 Thin Layer Chromatography................................................................................................ 72
4.4 The Ames test....................................................................................................................... 76
CHAPTER 5: DISCUSSION AND CONCLUSION ....................................................................78
REFERENCES ..............................................................................................................................86
vii
LIST OF FIGURES
Figure 2.1: Chironia baccifera ..................................................................................................... 21
Figure 2.2: Harpephyllum caffrum ............................................................................................... 22
Figure 2.3: Hermannia cuneifolia ................................................................................................. 23
Figure 2.4: Hermannia cuneifolia leaves and seeds ..................................................................... 24
Figure 2.5: Pentzia incana ............................................................................................................ 25
Figure 2.6: Rhigozum obovatum ................................................................................................... 26
Figure 2.7: Felicia muricata ......................................................................................................... 27
Figure 3.1: Powdered leaves of Rhigozum obovatum ................................................................... 39
Figure 3.2: Centrifuged extracts in the respective solvents .......................................................... 40
Figure 3.3: Centrifuged extracts in evaporating beakers .............................................................. 40
Figure 3.4: Methods used for antimicrobial investigation versus No. of Publications ................. 42
Figure 3.5: Mast Multipoint Inoculator ........................................................................................ 43
Figure 3.6: Salmonella typhimurium reaction on API Kit ............................................................ 47
Figure 4.1: Agar plate containing extracts of Pentzia incana showing slight inhibition of bacteria
....................................................................................................................................................... 48
Figure 4.2: Agar plates containing extracts of P.incana, F.muricata & H.cuneifolia .................. 49
Figure 4.3: Agar plate containing methanol extracts of H.cuneifolia compared with the control
plate ............................................................................................................................................... 50
Figure 4.4: Agar plate containing acetone extracts of H.cuneifolia compared with the control
plate ............................................................................................................................................... 50
Figure 4.5: Agar plate containing aqueous extracts of H.cuneifolia compared with the control
plate ............................................................................................................................................... 51
Figure 4.6: Microtitre plate showing colour intensity .................................................................. 67
Figure 4.7: Microtitre plate showing MIC values ......................................................................... 67
Figure 4.8: Plant extracts spotted on TLC silica plates ................................................................ 73
Figure 4.9: TLC silica plates spotted with extracts developing in air tight glass jar .................... 73
Figure 4.10: Developed TLC silica plates after evaporating and drying ...................................... 74
Figure 4.11: F1 to F6 are TLC silica plates after the bioautographic assay viewed under UV light
....................................................................................................................................................... 75
viii
LIST OF TABLES
Table 2.1: Comparison of Gram-positive and Gram-negative cell walls ....................................... 7
Table 2.2: Western versus Traditional Diagnosis and Treatment ................................................. 34
Table 3.1: Microtitre plate layout with plant extracts ................................................................... 44
Table 4.2: Summary of microorganisms inhibited by extracts of Hermannia cuneifolia ............ 54
Table 4.3: Antimicrobial results of Pentzia incana extracts ......................................................... 55
Table 4.4: Antimicrobial results of Rhigozum obovatum extracts ................................................ 57
Table 4.5: Antimicrobial results of Felicia muricata extracts ...................................................... 60
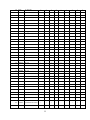
Table 4.6: Antimicrobial results of Harpephyllum caffrum extracts ............................................ 63
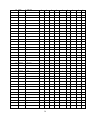
Table 4.7: Antimicrobial results of Chironia baccifera extracts .................................................. 65
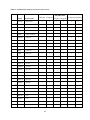
Table 4.8: Mean MIC results of 39 selected microorganisms tested with extracts of H.caffrum . 68
Table 4.9: Mean MIC results of 39 selected microorganisms tested with extracts of C.baccifera
....................................................................................................................................................... 69
Table 4.10: Mean MIC results of 39 selected microorganisms tested with extracts of H.cuneifolia
....................................................................................................................................................... 71
Table 4.11: R f values of major zones present in chromatograms of methanol and acetone
Harpephyllum caffrum extracts..................................................................................................... 76
Table 4.12: Number of histidine+ revertants in Salmonella typhimurium strain TA100 ............. 76
ix
LIST OF ABBREVIATIONS
A
A
-
Acetone
A.baumanii
–
Acinetobacter baumanii
A.haemolyticus
–
Acinetobacter haemolyticus
AIDS
-
Acquired Immunodeficiency Syndrome
A.lwoffi
–
Acinetobacter lwoffii
APC
–
Activated Protein C (drotrecogin alfa
activated)
API
–
Analytical Profile Index
AST
–
Antimicrobial Susceptibility Test
ATCC
–
American Type Culture Collections
-
Bacillus cereus
C.albicans
–
Candida albicans
C.lusitaniae
–
Candida lusitaniae
C.krusei
–
Candida krusei
CNS
–
Coagulase Negative Staphylococcus
CSF
–
Cerebral Spinal Fluid
C.baccifera
-
Chironia baccifera
CPFA
–
Coupled Plasma Filtration Adsorption
CRRT
–
Continous Renal Replacement Therapy
–
Dimethyl Sulphoxide
Ed.
-
Editor
ed.
-
Edition
E.agglomerans
–
Enterococcus agglomerans
B
B.cereus
C
D
DMSO
E
x
E.cloacae
–
Enterococcus cloacae
E.faecalis
-
Enterococcus faecalis
E.coli
–
Escherichia coli
F.muricata
–
Felicia muricata
FTIR
-
Fourier transform-infrared
-
Grams
F
G
g
H
H.caffrum
–
Harpephyllum caffrum
H.cuneifolia
–
Hermannia cuneifolia
HIV
–
Human Immunodeficiency Virus
HPF
–
High Power Field
HPLC
-
High Performance Liquid Chromatograph
–
р-iodonitrotetrazolium violet
K.oxytoca
–
Klebsiella oxytoca
K.pneumoniae
–
Klebsiella pneumoniae
–
Leuconostoc pseudomesenteroides
M
–
Methanol
MDR
–
Multi-drug Resistance
MH
–
Mueller-Hinton
MIC
–
Minimum Inhibitory Concentration
MOF
–
Multiple Organ Failure
MRSA
–
Methicillin Resistant Staphylococcus aureus
I
INT
K
L
L.pseudomesenteroides
M
xi
MRSE
–
Methicillin Resistant Staphylococcus epidermidis
nm
-
Nanometer
NMMU
-
Nelson Mandela Metropolitan University
PAS
–
Physiologically Active Substances
PBS
-
Phosphate buffered saline
P.incana
–
Pentzia incana
P.stuartii
–
Providentia stuartii
P.orizihabitans
–
Pseudomonas orizihabitans
P.stutzeri
–
Pseudomonas stutzeri
P.aeruginosa
–
Pseudomonas aeruginosa
-
Distance of travel of the zone divided by the
N
P
R
Rƒ
distance of the mobile phase front.
rpm
-
Revolution per minute
R.obovatum
–
Rhigozum obovatum
S
Salm
–
Salmonella
SATMERG
–
South African Traditional Medicines Research
Group
SIRS
–
Systemic Inflammatory Response Syndrome
S.aureus
–
Staphylococcus aureus
S.haemolyticus
–
Staphylococcus haemolyticus
S.hominis
-
Staphylococcus hominis
S.group b
–
Beta-hemolytic Streptococcus group b
S.bovis
–
Streptococcus bovis
TLC
–
Thin Layer Chromatography
TCM
-
Traditional Chinese Medicine
T
xii
TM
–
Traditional Medicine
UA
–
Urine analysis
UV
–
Ultra-violet light
W
–
Water
WBC
–
White Blood Cells
WHO
–
World Health Organization
U
W
xiii
CHAPTER 1: INTRODUCTION
The amount of medicinal plants and herbal medicinal products used worldwide has risen
dramatically in the last decades (Reich and Schibli, 2006).
Southern Africa has over 30,000
species of higher plants, mostly endemic, of which about 3,000 are used in traditional medicine
(Van Wyk and Gericke, 2000). The use of plants in herbal medicine is an age old practice and is
still prevalent all over the world, while the dependence on plants as the source of medicine is still
very common in developing countries, where traditional medicine plays a major role in health
care delivery (Adhikarla, 1984; Farnsworth, 1984a).
In most developing countries, where coverage by health services is limited, it is to the traditional
practitioner or to folk medicine that the majority of the population turns when sick. The
treatment they receive is largely based on the use of medicinal plants. Early in this century, the
greater part of medical therapy in the industrialized countries was dependent on medicinal plants
but, with the growth of the pharmaceutical industry, their use fell out of favour. Even so, 25% of
all prescriptions dispensed between 1959 and 1980 from community pharmacies in the United
States contained plant extracts or active principles prepared from higher plants (Farnsworth,
1984b). Now the pendulum is swinging back and the value of medicinal plants in treatment is
receiving increasing attention worldwide.
According to data from the World Health Organization [WHO] (2006), plants are sources of
biologically active compounds, used by about 80% of the world population, both in natural form
as teas, and as manufactured drugs. In wealthy countries, growing numbers of patients rely on
alternative medicine for preventive or palliative care. In France, 75% of the population has used
complementary medicine at least once; in Germany, 77% of pain clinics provide acupuncture;
and in the United Kingdom, expenditure on complementary or alternative medicine stands at
US$ 2,300 million per year (WHO, 2009). Traditional medicine is an integral part of the South
African cultural life, a position that is unlikely to change to any significant degree in the coming
years. For instance, it is estimated that between 12 and 15 million South Africans still depend on
traditional herbal medicines from as many as 700 indigenous plant species (Brandt et al., 1995;
Meyer et al., 1996).
There has been an increasing incidence of microbial infections in recent years, largely due to the
increase in AIDS-related opportunistic fungal pathogens and the emergence of resistance
1
microbial species (Silva et al., 2001; Afolayan et al., 2002). Bacterial infections are prevalent in
developing countries due to factors such as inadequate sanitation, poor hygiene and overcrowded
living conditions (Rasoanaivo and Ratsimamanga-Urveg, 1993).
Bloodstream infections cause substantial morbidity and mortality. Increasing rates of
antimicrobial resistance, changing patterns of antimicrobial usage and the wide application of
new medical technologies may change the epidemiology and outcome of bloodstream infections.
According to the Journal of Clinical Microbiology, 44% of the total number of deaths as a
percentage of septic episodes due to infection is caused by Candida species, 41% by anaerobes,
36% by Pseudomonas aeruginosa, 29% by Enterococci, 28% by Coagulase Negative
Staphylococci, 23% by Staphylococcus aureus, 20% by Escherichia coli and Streptococcus
viridans, 16% by Klebsiella species, 14% by Enterobacter species and 7% by Streptococcus
pneumoniae (Diekema et al., 2003).
Sepsis remains the major cause of mortality worldwide, claiming millions of lives each year. The
past decade has seen major advances in the understanding of the biological mechanisms involved
in this complex process. Unfortunately, no definitive therapy yet exists that can successfully treat
sepsis and its complications (Tetta et al., 2003b). Despite vast resources spent on sepsis research,
the condition remains complex and poorly understood, and to this day treatment consists
essentially of critical organ support. Multiple therapies have failed in the past (Tetta et al.,
2003a).
It is believed that most of the plants used by Africans in the Eastern Cape in the preparation of
herbal remedies possess pharmacologically active compounds (Coetzee, 2000). For example, in a
study by Fourie et al., (1992) at least 31% of 300 plants screened showed marked activity, 21%
were considered inactive, and 48% moderately active. On the other hand, Brown (1969) was of
the opinion that plant remedies should be regarded with scepticism because the efficacy of many
had not been proven.
Despite the availability of different approaches for the discovery of therapeutic agents, natural
products still remain as one of the best reservoirs of new structural types (Hostettmann, 1999).
To this effect, in the constant effort to improve the efficacy and ethics of modern medicinal
practice, researchers are increasingly turning their attention to folk medicine as a source of new
drugs (Wayne, 1998; Hoareau and Dasilva, 1999).
2
1.1 Aim
The purpose of this study is to investigate the biological activities of medicinal plants.
Challenges in biological screening remain a key focus in drug discovery from medicinal plants
(Balunas and Kinghorn, 2005).
1.2 Objectives
• To determine the antimicrobial activity of the plant extracts.
• To determine the minimum inhibitory concentration (MIC) of the plant extracts.
• To analyze the thin layer chromatography fingerprints found in the selected medicinal plants.
• To evaluate the mutagenicity of the plant extracts.
3
CHAPTER 2: LITERATURE REVIEW
2.1 Introduction
The purpose of this chapter is to discuss:
a) Septicaemia with regard to its definition, causes, severity and risk factors, classification,
prevention, diagnosis and treatment.
b)
Traditional herbal medicine, its importance, its toxicity and mutagenic effect, how it is
prepared and administered, as well as its comparison to western medicine.
c)
Medicinal plants under investigation, including botanical classifications and vernacular
names, macroscopical morphology and geographical distributions.
d)
Traditional healers’ methods of diagnosis, beliefs and practices.
e)
The study area.
Furthermore, a brief summary of the known major phytochemical constituents of each of the
plant species under investigation is also given, as well as the ethnopharmacological application
of these plants by various cultures, and previous scientific research conducted on the efficacy of
some plants in treating the conditions for which they are used.
2.2 Septicaemia
Septicaemia is defined as a very serious condition with severe toxaemia and shock (Reid and
Robert, 2005). It is also known as sepsis or blood poisoning. Sepsis is a systemic immune
response that leads to multiple organ failure (MOF) (Wenzel, 2002). Severe sepsis and septic
shock are the most common causes of MOF (Beal and Cerra, 1994). MOF remains the most
frequent cause of death in patients admitted to the intensive care unit, with a mortality rate
exceeding 50% (Baue et al., 1998; Wenzel, 2002). Sepsis occurs when the bloodstream becomes
infected with bacteria. If the bacteria continue to multiply, the condition progresses to septic
shock, blood pressure plummets and organ systems begin to shut down. Over 600,000 cases of
septicaemia occur in the United States each year, and approximately two-thirds of these cases are
diagnosed in hospitalized patients (Longe and Frey, 2006).
Sepsis is ranked as the sixth leading cause of death among neonates and the eighth leading cause
of death for infants through the first year of life (Heron, 2007). The incidence of neonatal sepsis
is 1 to 5 per 1,000 live births (Fanaroff and Martin, 2006). Although no significant sex difference
4
has been reported, it was noted as early as the 1960s that male infants had a higher incidence of
neonatal sepsis than females, which may be related to X-linked immunoregulatory genes
(Fanaroff and Martin, 2006). Other risk factors for neonatal sepsis include a history of immune
deficiency disorders such as severe combined immunodeficiency syndrome and some inborn
errors of metabolism such as galactosemia, which may present in the first week of life with
Escherichia coli sepsis or urosepsis (Robinson et al., 2008).
Sepsis encompasses a complex mosaic of interconnected events that generates systemic
inflammatory response syndrome (SIRS), sepsis syndrome, and septic shock (Tetta et al.,
2003a). According to an observational study conducted by Dombrovskiy et al. (2006) entitled as
“to determine the frequency of severe sepsis and drotrecogin alfa use in hospitalized patients in
New Jersey”, patients with sepsis were identified using the following International Classification
of Diseases, 9th Edition, Clinical Modification. The classifications were septicaemia, salmonella
septicaemia, septicemic plague, anthrax septicaemia, meningococcal septicaemia, waterhouseFriderichsen syndrome, herpetic septicaemia, gonococcal septicaemia, systemic candidiasis, and
systemic inflammatory response syndrome due to infectious process without organ dysfunction.
They defined severe sepsis as sepsis associated with organ dysfunction, as established by the
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference
(American College of Chest Physicians, 1992).
Septicaemia is common in Africa because of cultural practices like circumcisions. About 25% of
the total world male population is circumcised and circumcision remains one of the oldest and
commonest operations performed all over the world (Ben Chaim et al., 2005; Puig Sola et al.,
2003; Wilkinson, 1997). The complications rates of the procedure range between 0.19% and
3.1% (Ben Chaim et al., 2005; Wiswell and Geschke, 1989; Manji, 2000; O’Brien et al., 1995).
Neonatal circumcision as practiced is quite common worldwide. The people of pacific origin
prefer their children to be circumcised between the ages of 6 and 10 years (Afsari et al., 2002).
Circumcisions undertaken in non-clinical settings can have significant risks of serious adverse
events, including death. Among 50 patients admitted to hospital with post-circumcision
complications in Nigeria and Kenya between 1981 and 1998, 80% had been circumcised by
medically untrained traditional surgeons. One of these patients died from septicaemia (Magoha,
1999).
5
Among the Xhosa tribe in the Eastern Cape, South Africa, it is done in adolescence as an
initiation rite to manhood (Mogotlane et al., 2004). Mayatula and Mavundla, (1997) found that
an unsterilized unwashed blade was being used on a dozen or more initiates in a single session
(Naude, 2002). Initiates were also significantly dehydrated during their 2 week period of
seclusion in the belief that this reduces weeping of the wound, and after-care was in the hands of
a traditional attendant with no basic medical training (Mayatula and Mavundla, 1997). The
combination of dehydration and septicaemia could result in acute renal failure, gangrene, tetanus
or even death (Mayatula and Mavundla, 1997; Naude, 2002). The Eastern Cape Provincial
Department of
Health recorded 2,262 hospital admissions, 115 deaths and 208 genital
amputations involving circumcisions between 2001 and 2006 (Meissner and Buso, 2007). In a
number of cases Helichrysum species were used to treat circumcision wounds. An investigation
on Helichrysum aureonitens for antimicrobial activity and antimicrobial compound isolation
yielded 3,5,7-trihydroxyflavone (Meyer and Afolayan, 1995; Meyer and Dilika, 1996; Afolayan
and Meyer, 1997; Dilika et al., 1997), a compound with antimicrobial activity mainly against
Gram-positive bacteria.
2.2.1 Bacteriology
As a number of indications for the bacterial species relate to infection and infectious conditions,
it is pertinent to include a brief review of bacteriology and mycology in an attempt to understand
the antimicrobial actions of the plant extracts.
2.2.2 Size and shape of bacteria
The majority of bacteria range from 0.20 to 2.0 micrometres (µm) in diameter and from 2 to 8µm
in length. They are unicellular structures which may occur as cylindrical (rod shaped), spherical
(coccoid) or spiral forms (Talaro and Talaro, 1996; Tortora et al., 1994; Hugo, 1992). Coccoid
cells have a tendency to grow in aggregates. Other bacteria exist in assemblies of pairs
(diplococci), groups of four (sarcinae), unorganized arrays like a bunch of grapes
(staphylococci) and in chains like string of beads (streptococci). Rod shaped bacteria
occasionally occurs in chains while spiral shaped bacteria normally occur singly (Talaro and
Talaro, 1996; Tortora et al., 1994).
Bacteria can be divided into two main groups according to the characteristics of their cell wall.
Table 2.1 below shows the comparison of Gram-positive and Gram-negative cell walls.
6
Table 2.1: Comparison of Gram-positive and Gram-negative cell walls
Characteristic
Gram-positive
Gram-negative
Number of major layers
1
2
Chemical make-up
Peptidoglycan
Lipopolysaccharide
Teichoic Acid
Lipoprotein
Lipoteichoic Acid
Peptidoglycan
Overall Thickness
Thicker (20-80 nanometres) Thinner (8-11 nanometres)
Outer Membrane
No
Yes
Periplasmic Space
Absent
Present in all
Porin Proteins
No
Yes
Permeability to Molecules
More permeable
Less permeable
(Taken from Talaro and Talaro, 1996)
2.2.3 Mycology
Mycology is the study of fungi; their genetic and biochemical properties, their taxonomy, their
use to humans as a source of medicines like penicillin, food as well as their dangers such as
poisoning and infection. Pathogenic fungi have the ability to actively attack and invade tissues
(Bauman, 2007; Hawksworth, 1974). Fungi are ubiquitous in the environment, and infection due
to fungal pathogens has become more frequent (Walsh and Groll, 1999; Fleming et al., 2002).
Although, fungal-related disease may not be as common as other bacterial infections, when they
are present, they could be difficult to eradicate, especially in immunosuppressive situations
(Bryce, 1992). Mycotic infections have been observed to be the primary cause of mortality in
patients with severely impaired immune mechanisms (Kelbergh, 1997).
Research indicated that all over the world, 58-81% of all patients contract a fungal infection at
some time during the primordial stage or after developing AIDS and 10-20% have died as a
direct consequence of fungal infections (Drouhent and Dupont, 1989). Opportunistic fungal
pathogens have become a common cause of morbidity and mortality with the rise in HIV
(Garbino et al., 2001). In HIV patients, the presence of oral candidiasis is the earliest
opportunistic infection (Fan-Havard et al., 1991). Clinically, the fungal infection is identified as
creamy-white, curd-like patches on the tongue or other oral mucosal surfaces which are removed
by scrapings. If left untreated, this leads to difficulty in chewing and swallowing and is
7
sometimes associated with severe diarrhoea (Drouhent and Dupont, 1989; Dube and Mutloane,
2001). Hence, those who suffer from oral candidiasis often lose substantial weight because of a
sore throat, which prevents them from eating (Sanne, 2001). Candida albicans was included in
this study because it is a pathogenic microorganism causing oral thrush particularly in immunocompromised individuals (Samaranayake, 2000).
Furthermore, since the first human kidney was transplanted in 1954, the frequency of organ
transplantation has increased and the number of immuno-compromised hosts has grown steadily
with the introduction of novel immuno-suppressive agents and improved rates of survival. Thus
the incidence of opportunistic infections, including fungal infections, has also increased (Rubin
et al., 1981; Winston et al., 1995; Fishman and Rubin, 1998). As a result, antifungal therapy is
playing a greater role in health care and the screening of traditional plants in search of novel
antifungals is now more frequently performed (McCutcheon et al., 1994; Jones et al., 2000;
Motsei et al., 2003).
The search for novel antifungal agents relies mainly on ethnobotanical information and
ethnopharmacologic exploration. The medicinal knowledge of North American First Nations
peoples has been shown to be a valid resource. Studies have revealed a high degree of correlation
between traditional medicinal uses and laboratory analysis (McCutcheon et al., 1994; Bergeron
et al., 1996; Jones et al., 2000). The traditional preparations of these medicines often involve a
broth or tea. However, much of the antifungal research conducted to date has assessed ethanol or
methanol extracts while few studies have utilized aqueous extracts, a closer approximation of the
traditional medicine.
Alcohol extracts provide a more complete extraction, including less polar compounds, and many
of these extracts have been found to possess antifungal properties. Yet success with aqueous
extracts has also been observed (Ali-Shtayeh and Abu Ghdeib, 1999).
2.2.4 Prevention, diagnosis and treatment
There is no specific laboratory test for early diagnosis of septicaemia (Longe and Frey, 2006).
Nevertheless, in an effort to diagnose sepsis, the following laboratory tests are performed: a
complete blood cell count (CBC), blood culture, urinalysis (UA), urine culture, and cerebrospinal
fluid (CSF). The tests are performed on all patients presenting with possible sepsis (American
8
College of Emergency Physicians, 2003). In neonates, 1-2 ml of blood is acceptable for a blood
culture. The urine culture should be obtained via sterile urethral catheterization or suprapubic
aspiration in infants, and using an aseptic technique in adults. A urine analysis showing 10 or
greater white blood cells (WBCs)/high-power field (HPF) and/or bacteria on Gram stain suggest
a urinary tract infection. Accepted normal range values for preterm and term neonates
respectively are 0-25, 0-22 cells/mm3 (WBCs); 65-150, 20-170 mg/dl (protein); 24-63, 34-119
mg/dl (glucose) (McMillan et al., 1999).
Africans in the Eastern Cape have a long tradition of using plants in treating both human
(Hutchings, 1989a) and animal (Masika, et al., 1997) ailments. However, the effectiveness of the
various herbal remedies remains controversial. Historically, cases where herbal remedies were
effective in treating livestock diseases in the Eastern Cape have been reported. Smith wrote in
the late 19th century that, whenever herds sickened and died, the herbal preparations administered
by African herdsmen produced results far in advance of European remedies of that time. A
documented case involved the treatment of a horse with a cancer-like growth by the latex of a
plant Euphorbia. Samples that were sent to Germany revealed it to be a new species of Asclepiad
which was later used in the treatment of cancer patients (Johannes, 1915).
It is said that treatment of bacterial infections is a frequent problem due to the emergence of
bacterial strains resistant to numerous antibiotics (Keasah et al., 1998; Marimoto and Fujimoto,
1999). Only recently, activated protein C (APC) (drotrecogin alfa [activated]) has been the first
biologic agent approved in the United States for the treatment of severe sepsis though with
controversies (Tetta et al., 2003a).
Infectious diseases are usually characterised by clear symptoms, so it is likely that traditional
healers have been able to recognise such diseases and have developed effective therapies.
Moreover, as antibiotics mostly have clear effects, the chance of finding antimicrobially active
traditional medicine is considered to be high (Sofowora, 1984; Elmi et al., 1986).
2.2.5 Antibiotic therapy
Natural products from microorganisms have been the primary source of antibiotics, but with the
increasing acceptance of herbal medicine as an alternative form of health care, the screening of
medicinal plants for active compounds has become very important because these may serve as
promising sources of novel antibiotic prototypes (Meurer-Grimes et al., 1996; Rabe and Van
9
Staden, 1997; Koduru et al., 2006). In older studies, the green parts of the plant, Harpephyllum
caffrum, have given negative tests for the presence of antibiotics (Osborn, 1943). Yet, with
improved methods it was found to have antimicrobial properties against microorganisms like
Candida albicans.
2.2.6 Antibiotic resistance
Bacteria have evolved numerous defences against antimicrobial agents, and drug-resistant
pathogens are on the rise. This resistance is conferred by multi-drug resistance pumps,
membrane translocases that extrude structurally unrelated toxins from the cell. These protect
microbial cells from both synthetic and natural antimicrobials (Stermitz et al., 2000).
The growing problem of resistance in pathogenic microorganisms against many of the antibiotics
in routine use, combined with the existing problem of the adverse effects of many antibiotic
treatments, has recently increased research on the antimicrobial activities of various extracts and
compounds isolated from the plant species used in herbal medicine (Nostro et al., 2000; Kokoska
et al., 2002).
Currently, the emergence of resistant pathogens to many of the commonly used antibiotics has
provided an impetus for further attempts to search for new antimicrobial agents to combat
infections and overcome the problems of resistance to currently available antimicrobial agents
(Balandrin et al., 1985; Xu and Lee, 2001). The use of plant extracts and phytochemicals can be
of great significance in therapeutic treatments and could help curb the problem of these multidrug resistant organisms. In a study done with Pseudomonas aeruginosa, which is resistant to
different antibiotics, its growth was inhibited by extracts from clove, jambolan, pomegranate and
thyme (Nascimento et al., 2000).
The pattern of antimicrobial resistance varies widely. It is highest in countries where effective
therapy is either unavailable or too expensive and facilities for diagnosis are inadequate. The
pattern of antimicrobial resistance is often associated with a high prevalence of HIV infection
(Ison et al., 1998).
10
2.3 Bacteria and fungi selected for investigation
Gram-positive and Gram-negative bacterial strains were included in this study together with
some fungi. The bacterial strains include specific ATCC strains bought from Mast QC Sticks but
supplied by Davis Diagnostics, and clinical isolates obtained from National Health Laboratory
Service, Port Elizabeth, South Africa.
2.4 Traditional Herbal Medicines
Traditional medicine is the sum total of knowledge, skills and practices based on the theories,
beliefs and experiences indigenous to different cultures. It is used to maintain health, as well as
to prevent, diagnose, improve or treat physical and mental illness (WHO, 2008). The art of
healing with herbal remedies is empirical, and it is usually transferred directly by oral teaching
from master (father) to apprentice (son). Written documentation of the principles and practices of
herbal therapy has been sporadic at best. In some areas, documenting the art and practice of
herbalists is urgent because the knowledge is threatened with extinction (Masika et al., 2000).
In the World Health Report of 1995, ‘Bridging the gap’, the Director General of the WHO stated
that ‘poverty is the world’s deadliest disease’ (Anon, 1995). Due to this, some 80 per cent of the
world’s inhabitants rely mainly on traditional medicines for their primary health-care needs and
utilize medicinal plants (Akerele, 1993). Reliance of human communities on plant-based
remedies has a long-standing history and remains a vibrant culture interfacing with modern
healthcare (Makunga et al., 2008). A list of 21,000 species of medicinal plants used world wide
has been prepared (Penso, 1983), but others believe that this is a conservative estimate with the
number of species used being between 35,000 to 70,000 (Farnsworth and Soejarto, 1991). Dr X.
Zhang, a Medical Officer of Traditional Medicine for WHO, has stated that the majority of the
population in developing countries make use of their local medicinal plants because of the lack
of medical doctors, pharmaceutical products and money (Zhang, 1996).
Today, most of the population in urban South Africa, as well as smaller rural communities, is
reliant on herbal medicines for their health care needs. Apart from their cultural significance, this
is because herbal medicines are generally more accessible and affordable (Mander, 1998), easily
available and cheaper than modern medicine (Otshudi et al., 2000). As a consequence, there is an
increasing trend, world wide, to integrate traditional medicine with primary health care. Dual
11
health
systems
and
the
regulation
of
medicines
exist
simultaneously
for
both
complementary/traditional medicines and pharmaceuticals in most developing countries.
According to WHO, 65 out of 193 of its member states have regulatory systems dealing with
traditional medicines.
In countries such as Vietnam and China, the modern and traditional health systems are integrated
at the level of medical education and practice (Bodeker, 2001). In India, there are more than
200,000 registered traditional medicine practitioners, the majority having received training in
degree granting colleges of Ayurvedic or Unani medicine.
As a result of a telephone survey conducted in the USA, it was estimated that some 42.5 million
visits were made to herbalists in 1990, and that 425 million visits would have been made to
unconventional therapists contrasting with the 388 million actual visits made to primary healthcare physicians (Eisenberg et al., 1993). In South Africa there has been interest in integrating the
different health systems, such as the 48-bed hospital in Kwa-Mhlanga founded by a traditional
African healer that combines the different aspects of traditional African, western and other
complementary healing practices (Helwig, 2000).
Although traditional remedies were regarded as of little relevance to modern drug discovery in
earlier years, they are now regarded as an important source of potentially therapeutic drugs (Cox
and Balick, 1994).
The global demand for natural, healthy living conditions during the last century led to a greater
awareness of traditional medicine (Koo and Wright, 1999). From an economic point of view, the
high cost of imported conventional drugs and/or inaccessibility to western health care facilities
implies that traditional mode of health care is the only form of health care that is affordable and
available to the rural people. On the other hand, even when western health facilities are available,
traditional medicine is viewed as an efficient and an acceptable system from a cultural
perspective (Munguti, 1997) and as a result, traditional medicine usually exists side by side with
western forms of health care (Sindiga, 1994). As First World countries became more aware of
the positive correlations between traditional remedies and scientific proof of their healing effect,
pharmaceutical formulations were developed on the basis of natural biochemical compounds.
The identity of various bioactive substances were determined and synthesized by pharmaceutical
companies for uses against a wide range of diseases (Walsh, 1998).
12
Recently, biologically active compounds and extracts isolated from such plant species used in
herbal medicine have been the centre of interest (Nishino et al., 1987; Abdulla et al., 1989;
Brantner et al., 1996; Anonymous, 1997). Numerous kinds of metabolites have been isolated
from various plants and its chemical structures have been elucidated (Ghazal et al., 1992;
Brantner et al., 1996).
2.5 Medicinal plants and their importance
Plants were once a primary source of all the medicines in the world and they still continue to
provide mankind with new remedies. Natural products and their derivatives represent more than
50% and higher plants contribute no less than 25% to the total of all drugs in clinical use in the
world (Kinghorn and Balandrin, 1993). There is a growing interest in natural and traditional
medicines as a source of new commercial products (Van Wyk et al., 1997).
It is believed that there are about 27 million consumers of medicinal plants in South Africa
(Mander, 1998). These medicinal plants form an important foundation in various ethnobotanical
studies and phytochemical analysis in the different traditions worldwide. Medicinal plants and
their derivatives contribute to more than fifty percent of all drugs used worldwide (Van Wyk et
al., 1997; Kong et al., 2003).
Despite well-documented ethnobotanical literature, very little scientific information (e.g.
efficacy, phytochemistry) has become available on indigenous medicinally used plants. It is only
recently (1997-2008) that a number of findings have emerged on the chemistry and biological
activity of plants used in traditional healing. This recent emergence in the scientific validation of
South African medicinal plants can possibly be attributed to public awareness, method
advancements and a number of citations in local books confirming the need for such studies
(Hutchings et al., 1996; Van Wyk et al., 1997). Available reports tend to show that indigenous
folk-medicinal plant preservation and study is vital because such plants are fully adapted to local
environments and to conditions compared to introduced species (Qin and Xu, 1998).
Pharmacologically active compounds and phytochemicals isolated from such endemic and
indigenous plants used in folk medicine have been the center of interest during the past few
decades (Farnsworth, 1994; Benzi and Ceci, 1997).
13
For some of the old medicinal plant extracts, purification and isolation of a single active
ingredient has enabled standardized doses to be given in tablet or capsule form. From the view
point of the patient, it matters little as to whether or not the capsule or tablet contains a synthetic
or a natural medicinal drug. Attempts to synthesize these active compounds have largely been
successful, but in most cases this has proved to be uneconomic in comparison to isolation from
plant material. Thus today, drugs such as morphine (the potent pain-killer from the opium poppy)
and digoxin (for treatment of congestive heart failure, from foxglove) are isolated from their
plant sources. Despite considerable efforts to produce synthetic analogues with safer profiles for
use in humans, both of these drugs continue to play prominent roles in medicine. It is claimed
that natural products isolated from higher plants (including their derivatives and analogues)
account for 25 per cent of the number of drugs in clinical use today (Balandrin et al., 1993).
Over the years, various alternative uses for plants were discovered and developed, such as plant
derivatives used in the formulation of health and functional foods (Coghlan, 1996; Mozersky,
1999; Mukhtar and Ahmad, 2000). Having access mostly to their immediate surroundings, the
natural environment provided indigenous people with remedies for the relief of pain and disease.
A broad range of medicinal plants is used against microbial related illnesses, such as infections,
diarrhoea or intestinal problems, asthma, psoriasis, articular rheumatism and skin problems
(Hutchings et al., 1996; McGaw et al., 2000).
The regulation of traditional medicinal plant use embodies three fundamental aspects: quality,
safety and efficacy. Unfortunately, comprehensive safety and efficacy data on traditional
medicines are lacking (Springfield et al., 2005). The shortage of safety and quality controls of
South African Medicinal plants is further compromised by the fact that there is currently no
pharmacopoeia that documents indigenous medicinal plants of South Africa (Fennell et al.,
2004).
In other countries, pharmacopoeias or medicinal manuals of useful available plants were
compiled, later called medicinal plants (Van Wyk and Gericke, 2000; Lall, 2000). Today, these
natural resources are still used. They make a significant contribution to primary health care
especially in developing countries (Grierson and Afolayan, 1999), but also in the western world.
Already an estimated 122 drugs from 94 plants species have been discovered through
ethnobotanical leads (Fabricant and Farnsworth, 2001).
14
Of the 250,000 species of higher plants on earth, the majority have not been examined in any
detailed way for their pharmacological properties. One of the largest investigations into potential
new drugs from plants has been undertaken by the National Cancer Institute in the USA.
Between 1960 and 1982, some 35,000 samples of higher plants were collected and provided
114,000 extracts which were screened for anticancer activity (Cragg et al., 1993). Recently,
important new anticancer drugs such as taxol (a highly effective drug against breast and ovarian
cancers, extracted from the bark of the Pacific yew [Taxus brevifolius]) and vincristine (a binary
indole alkaloid used in breast and uterine cancer chemotherapy (Bruneton, 1995) extracted from
Catharanthus roseus), have been developed (Van Wyk et al., 1997).
Aloe plants have been used in folk medicine for the treatment of various conditions including
gastrointestinal disorders, insect bites, skin burns and other skin injuries. There are many
products ranging from aloe gels, powders, capsules and creams that have recently appeared on
the commercial market prepared from different aloe species (El Sohly et al., 2004). Products
such as ‘Aloe 4 U’ commercially sold in South Africa consists of many different aloe species
mixed together to reportedly give a stronger effect (Ndhlala et al., 2009).
Ndukwe et al. (2004) conducted a study investigating the antibacterial activity of chewing sticks,
his study confirms that chewing sticks have a potential to prevent oral ailments. A majority of
the plants tested in his study reveals that chewing sticks are capable of inhibiting Gram-positive
and Gram-negative bacteria such as Bacillus subtilis, Porphyromonus gingivalis and
Fusobacterium nucleatum. Several African tribes use the common traditional chewing sticks
called ‘Muthala’, scientifically known as Diospyros lysioides DESF (Khan, 1978) and/or Euclea
natalensis A.D.C. (Lall and Meyer, 2000).
Plant remedies are becoming popular in modern-day western countries, where natural products
are now often preferred to synthetic chemicals (Elvin-Lewis, 2001). Not only the natives used
plants for their healing properties, but settlers and farmers were also dependent on these
resources, especially before the development of and access to pharmacies or commercial
products (Moolman, 1984).
Natural remedies are known to be used predominantly by Latin American, Asian and African
countries, which include India (Jain, 1994; Valsaraj et al., 1997; Srinivasan et al., 2001); Turkey
(Sokmen et al., 1999); Israel (Alkofahi et al., 1997; Mahasneh and El-oqlah, 1999; Khafagi and
15
Dewedar, 2000); Mexico (Navarro et al., 1996; Rojas et al., 2001); Rwanda (Boily and Van
Puyvelde, 1986; Sindambiwe et al., 1999) and South Africa (Cunningham, 1991; Grierson and
Afolayan, 1999; Lin et al., 1999). Third world countries are often subject to shortage of funds,
medical facilities, qualified personnel and newly developed medicine, which make them more
dependent on their natural resources (Mammem and Cloete, 1996; Shale et al., 1999).
Sadly, consequences posed on plant biodiversity by commercial harvesters have become more
evident, especially over the last century (Cunningham, 1991). Therefore, organizations initiated
programs to conserve and manage endangered flora. More attention has been focused on
biodiversity conservation and protection of natural products, especially in the northern
hemisphere. Still, the greatest natural variety, and subsequently also the most rapid loss of
biodiversity in the world, is currently found in Southern countries (Koo and Wright, 1999).
The high demand of medicinal plants in South Africa has led to over 10% of more than 20,000
plant species being threatened with a decreased availability and listed in the South African Red
Data books (Goldring, 1996; George and Van Staden, 2000). The Durban municipality in Kwa
Zulu-Natal has a medicinal plant nursery, Silverglen, which cultivates about 120 at risk plant
species. Despite the fact that certain more conventional traditional healers believe that plants
grown as agricultural crops will not have the same medicinal properties as those harvested from
the wild (Cunningham, 1993), 82% of urban-based healers and 69% of the clinic patients in the
Eastern Cape reported that they would make use of cultivated plants for medicinal purposes
(Dold and Cocks, 2002).
2.5.1 Economic importance of traditional medicine
Herbal treatments are the most popular form of traditional medicine, and are highly lucrative in
the international marketplace. Annual revenues in Western Europe reached US$5 billion in
2003-2004. Herbal medicine revenue in Brazil was US$160 million in 2007 (WHO, 2008).
However, the use of herbal medicine is increasingly becoming mainstream with retail sales of
herbal products in Australia estimated to be A$200 million (Wohlmuth et al., 2003).
The worldwide use of herbal medicinals has soared in the past decade reaching annual sales in
excess of 60 billion U.S. dollars and is expected to reach 55 trillion U.S. dollars by 2050.
Although most herbal remedies are consumed by adults, a growing proportion is consumed by
16
children of all ages. Two recent surveys report that up to 20% of children who are scheduled for
elective surgery consume herbal medicine (Lerman, 2005). This has happened over the past
years.
According to a survey by the International Trade Centre, trade in medicinal plants and their
derivatives in pharmacy has declined in many industrialized countries, owing to the volume of
competitive synthetic products currently marketed. Overall, the trade in botanicals has increased,
through their use in the health food and cosmetic industries. Imports, however, represent only a
minute percentage of the value of internal trade in medicinal plants. For example, in the United
States, imports in 1980 were valued at US$ 44.6 million compared to an internal trade in
medicinals and botanicals in 1981 estimated at US$ 3900 million. Over-the-counter sales of
herbal medicines in the USA and Canada during 1990 reached US$860 million with an annual
growth rate of 15% (Zhang, 1996). In Europe, the sales of herbal products have been referred to
as ‘Europe’s growth market’ which amounted to US$1.4 billion during 1992 (Anon, 1992).
De Smet (2005) reported the market estimates of 2003. He stated that European countries spent
almost $5 billion on over-the-counter herbal medicines. He continued saying that, all European
countries have not accepted herbal treatments with equal interest. While Germany and France are
leading on the over-the-counter sales, physicians in Great Britain prescribe herbal medicines,
which are not covered by the National Health Service.
A survey of herbal products sold in UK pharmacies indicated that about 150 medicinal herbs are
in common use (Newall et al., 1996). The majority of herbal products sold in the UK, whether
from pharmacies, health-food shops, supermarkets or mail order outlets, are not licensed as
medicines. Such products are controlled under food legislation and are referred to as food
supplements, or dietary integrators or nutraceuticals.
In a report by Akerele and collegues, the annual production of traditional plant remedies in China
was valued at US$ 571 million and the countrywide sales of crude plant drugs at US$ 1,400
million (Li Chaojin, 1987). Traditional medicines in China were reported to account for 30% 50% of medicines consumed and the total sales of their herbal medicines amounted to US$2.5
billion in 1993. In addition, China exported medicinal herbs in 1993 with an estimated value of
US$40 million (Bodeker, 1994). An article by WHO (2008), states that in China, sales of herbal
products totalled to US$14 billion in 2005.
17
One Italian company (Indena of Milan) specializes in the preparation of medicinal plant extracts
and utilizes some 12,000 metric tones of dried plant material annually. The company prepares
some 1,139 plant extracts for medicinal use together with 202 pure compounds, which are
isolated directly from plant material and used as such or as semi-synthetic derivatives. The main
markets for these products are Europe, USA, Japan and South Korea. Among the most popular
extracts used in Europe are garlic (Allium sativum, antimicrobial, blood cholesterol lowering),
ginkgo (Ginkgo biloba, circulatory insufficiency), saw palmetto (Serenoa repens, diuretic,
reduction of enlarged prostate), milk thistle (Silybum marianum, treatment of liver disorders)
bilberry (Vaccinium myrtillus, inflammation of mucous membranes and diarrhoea), and grape
seeds (Vitis vinifera, antioxidant and cardiovascular disease treatment) (Bombardelli, 1996).
Inappropriate methods of collection, processing and storage with undesirable contaminants in the
products, have all contributed to the negative impact with regards to African natural plant
products competing in international markets (Tadmor et al., 2002). The bulk of the medicinal
plant trade takes place at informal street markets and involves the sale of unprocessed or semiprocessed products. Raw plant material undergoes very little processing (e.g. grinding or boiling)
before being administered to the patient (Mander and Le Breton, 2006).
A recent study on South African medicinal plants recommended for the treatment of HIV/AIDS
revealed that many plants had high bacterial and fungal numbers due to low environmental
sanitation and a low standard of processing during preparation (Govender et al., 2006). A study
on African herbal teas showed samples containing a high microbial count, unacceptable in
modern food and food supplement markets (Tadmor et al., 2002).
The global market for traditional therapies stands at US$ 60 billion a year and is steadily
growing. In addition to the patient safety issue and the threat to knowledge and biodiversity,
there is also the risk that further commercialization through unregulated use will make these
therapies unaffordable to many who rely on them as their primary source of health care. For this
reason, policies on the protection of indigenous or traditional knowledge are necessary (WHO,
2009).
18
2.6 Medicinal plants under investigation
Medicinal plants contain molecular structures and a built-in ability to produce substances
(secondary metabolites) to protect itself from injury and disease. Plants are able to produce a
wide array of secondary metabolites through intricate metabolic pathways. Lovkova et al.
(2001), reports that the pharmacological activities of saponin-containing medicinal plants result
in their marked therapeutic effects. Secondary metabolites synthesized by plants serve as defence
mechanisms against predation by microorganisms (Cowan, 1999). These defence chemicals or
secondary metabolites of plants can serve several types of functions and are found in abundance
in plant species (Tsao et al., 2002). The ability of plants to manufacture secondary metabolites
has been widely exploited by man. Plant biotechnology can make important contributions to the
natural products sector even though, use of this technology in Africa is limited (Makunga et al.,
2008).
Medicinal plants contain the ability to initiate the production or release of specific compounds.
These substances are able to inhibit the growth of particular microorganisms and suppress their
associated infections. The use of higher plants and preparations made from the medicinal plants
to treat infections is an age-old practice in a large part of the world population, especially in
developing countries, where there is dependence on traditional medicine for a variety of diseases
(Ahmad et al., 1998). Bioassay-guided fractionation of plant species may lead to the discovery of
new antibacterial agents and a better understanding of how ethnomedicine can treat infections.
The larger part of the current research in ethnopharmacology is focused on understanding the
molecular mechanisms whereby plants construct chemical defense systems (Trankina, 1998).
Another key area that was relevant to this project was: Phytotherapy (healing using plants). The
protocols and principles of these two disciplines were intertwined to determine the medicinal
value of selected plant species as well as their possible implementation as scientifically validated
health care alternatives in less advantaged communities.
Due to genetic, ecological and environmental differences, plants harvested from wild generally
vary in quality and consistency of active compounds (Bopana and Saxena, 2007). Medicinal
plant gatherers collect their materials throughout the year to supply the persistent demand for
medicinal plants. If mature trees or plants cannot be found, then younger ones suffice, which
results in availability of inconsistent plant material of the same species (Von Ahlefeldt et al.,
19
2003). Plant age, seasonal variation and geographical deviation in harvest site are contributing
factors towards variation in biological activity (Taylor and Van Staden, 2001; Shale et al., 2005;
Buwa and Van Staden, 2007).
Collections of Harpephyllum caffrum Bernh. (Anacardiaceae) bark from the same female tree at
different times of the year showed the highest antibacterial activity in summer months (Buwa
and Van Staden, 2007). Buwa and Van Staden, (2007) studied the effects of collection time on
the antimicrobial activities of Harpephyllum caffrum bark. Three collections were made from a
female tree in the Eastern Cape during 2003/2004 and tested for antibacterial and antifungal
activity. The highest antibacterial activity was detected with plant material collected in June
2003 and December 2003, with a decline in activity in extracts collected in September 2004.
Highest antifungal activity was detected in plant material collected in December 2003. TLC
analysis revealed some variation in chemical composition of each of the H.caffrum bark extracts
tested.
Plant-based antimicrobials and antibacterials represent a vast untapped source for medicines and
hence have enormous therapeutic potential (Phillipson, 1994). They are effective in the treatment
of infections while mitigating many of the side effects associated with synthetic antimicrobial
and antibacterials (Mathews et al., 1999; Bagghi, 2000). Many medicinal herbs are rare and
difficult to identify. To the untrained eye, especially when found in cut or chopped form, one
plant may look just like another. One species can however be the source of a life-saving drug
while a very similar plant may be a deadly poison (McKenna, 1996).
2.6.1 Chironia baccifera
Chironia baccifera is a shrub with widespread distribution in the Western and Eastern Cape
Provinces of South Africa (Springfield et al., 2005). It is also known as aambeibossie,
bitterbossie (Afrikaans); Christmas berry, Wild gentian, Piles bush, Toothache berry (English). It
belongs to the family of Gentianaceae. This is an important medicine in South Africa,
traditionally used by the Khoi as a purgative for haemorrhoids and to treat boils. A decoction of
the whole plant is taken as a blood purifier to treat acne and sores. An infusion may be used as a
remedy for diarrhoea, or for leprosy (Van Wyk and Gericke, 2000). A tea or decoction made of
the whole plant is drunk as a cleanser for skin problems and haemorrhoids {1/4 cup of fresh herb
to 1 cup of boiling water, draws for 3 minutes, then strain}(Roberts, 1990). It has shown that 45g
20
of dried plant is fatal to a rabbit and half a pound fatal to a sheep. Confirmation of toxicity in the
sheep and the rabbit discloses cyanosis of the mucosae, degenerative changes in heart muscle
and liver, much blood in and oedema of the lungs and catarrhal gastroenteritis (Watt and BreyerBrandwijk, 1962).
Figure 2.1: Chironia baccifera
(Taken from http://www.plantzafrica.com/plantcd/chironbac.htm)
For labour, it is one of the most important Cape herbs. An infusion of fresh leaves and stems, and
fruits if present, is very bitter and is taken post-partum to expel a retained placenta (Dawid
Bester, pers. comm.). Furthermore, the plant is used to treat stomach ulcers, syphilis, kidney and
bladder infections and diabetes. Side-effects that are known include a slightly loose stool, but
never to the extent of causing diarrhoea (Dawid Bester, pers. comm.). The plant has been
reported to be diaphoretic (Van Wyk and Gericke, 2000), cause sleepiness and increase
perspiration (Roberts, 1990).
2.6.1.1 Active ingredients
C.baccifera roots contain various secoiridoids, of which gentiopicroside is the main component,
together with smaller amount of swertiamarine, chironioside and others (Wolfender, 1993).
Other species of the family Gentianaceae, such as Gentiana lutea (yellow gentian) and C.krebsii
are known to contain gentiopicroside (Dictionary of Natural Products, 1996) and chironioside
(Wolfender, 1993), respectively. These are bitter substances, traditionally used in the liquor
industry (Bruneton, 1995).
2.6.1.2 Pharmacological effects
The bitter iridoids are known to stimulate appetite, but the compounds responsible for the
healing properties of Chironia appear to be unknown (Van Wyk et al., 1997).
21
2.6.2 Harpephyllum caffrum
This plant is also known as umgwenya (Xhosa, Zulu); mothekele (Northen Sotho); wild plum
(English); wildepruim (Afrikaans). It belongs to the family of Anacardiaceae (mango family),
which is the fourth largest tree family in Southern Africa. The natural distribution is restricted to
Southern Africa (Palmer and Pitman, 1972). H.caffrum grows from the Eastern Cape northwards
through KwaZulu-Natal, Swaziland, Southern Mozambique, Limpopo Province and into
Zimbabwe. The generic name Harpephyllum is of Greek derivation, meaning sickle-like leaves,
referring to the shape of the falcate leaflets. The specific name caffrum is derived from its place
of origin, Kaffraria, now part of the Eastern Cape. This word means ‘indigenous’.
Figure 2.2: Harpephyllum caffrum
(Taken from www.plantzafrica.com/planthij/harpephylcaf.htm).
The edible fruits are commonly used for eating and for making jams and jellies. They contain
citric and malic acids (Watt and Breyer-Brandwijk, 1962). The tree has some potential as a
commercial fruit crop but preliminary trial plantings in Israel were rather disappointing. The bark
is a popular traditional medicine and cosmetic for facial saunas and skin washes (Van Wyk and
Gericke, 2000). Williams (1930) claimed that the bark yields 18.2 per cent of tanning matter and
the leaf and twig 11.4%.
It is also used to treat acne and eczema (Pujol, 1990) and decoctions of the bark are used as
blood purifiers or emetics (Watt and Breyer-Brandwijk, 1962). According to Mr Mutwa
(pers.com), the bark is primarily used to purify the blood in a person with “bad blood,” which
manifests as pimples on the face.
2.6.2.1 Active ingredients
The chemical constituents of Harpephyllum caffrum are poorly known (Dictionary of Natural
products, 1996), but the presence of polyphenolic compounds and flavonoids have been reported
22
(El Sherbeiny and El Ansari, 1976). These include organic acids, such as protocatechuic acid,
and flavonols, such as kaempferol.
2.6.2.2 Pharmacological effects
The benefits derived from the use of this traditional medicine may be related to the phenolic
compounds (El Sherbeiny and El Ansari, 1976).
2.6.3 Hermannia cuneifolia
This is also known as agtdaegeneesbossie, broodbos, geneesbossie, pleisterbos, geelpleisterbos,
vet-en-broodbos (Afrikaans) and belongs to the family, Sterculiaceae. It is a sturdy, muchbranched shrublet, up to 500 mm high. Leaves occur in tufts and coarsely toothed, both surfaces
are covered with star-like hairs. It has yellow flowers that become red-brown with age and is
sweetly scented. The plant is very palatable and drought resistant. This plant is used medicinally
to heal wounds, therefore the name, geneesbos. The Europeans apply an infusion or a decoction
of this plant to sores and take the preparation internally (Watt and Breyer-Brandwijk, 1962).
Distribution: widespread in fynbos, karoo and grassland, from the Western Cape, Free State, to
Lesotho.
Figure 2.3: Hermannia cuneifolia
(Taken from www.plantzafrica.com/planthij/hermannia.htm).
23
The genus was named after Prof. Paul Herman (1640-1695), a German professor of botany at
Leyden and one of the first travelers and collectors at the Cape. Hermannias possess strong,
thick, rootstocks and underground stems, which enable them to withstand fires in the highveld
and overcome times of severe drought in arid areas. They are mostly very palatable to stock and
small game, and are generally heavily grazed.
2.6.3.1 Economic and cultural value
Many members of the genus are used medicinally, for anything ranging from respiratory
diseases, coughs and internal aches, as stimulants or purgatives, to soothing wounds and cuts.
Figure 2.4: Hermannia cuneifolia leaves and seeds
The common name pleisterbos (Hermannia cuneifolia) refers to the use of the leaves as plasters.
In some places the leaves are infused in a tea, and used to clean the blood. A root infusion was
used by the early European colonial settlers against epilepsy. A lotion of the leaf was used for
eczema and shingles. Certain species have magical significance and are used to drive out spirits
and to wash the divining bones (www.plantzafrica.com/planthij/hermannia.htm).
2.6.4 Pentzia incana (Karoo bush)
The plant belongs to the family Asteraceae. It is a small shrub in the sunflower family. Its yellow
ball-like flowers appear during the winter. Near Middelburg C.P., an infusion of the leaf of
Pentzia incana is commonly used by the Africans for the relief of stomach troubles (Kling,
1923).
24
Figure 2.5: Pentzia incana
(Taken from www.fs.fed.us/.../weeds/iw_karoo_bush.shtml).
For erysipelas and for pain after eating, the woody parts of Pentzia incana and of Antizoma
capensis are chewed and the saliva swallowed (Kling, 1923). It is said to be of value as pasture
(Botha, 1939) and is reported to be much eaten by all types of domestic stock (Burtt, 1912;
Marloth, 1913-32; Sim, 1907). Henrici (1952) has studied the starch and sugar content of the
plant.
2.6.5 Rhigozum obovatum
It is an ideal shrub or small tree to bring life to gardens in dry areas where water is in short
supply and garden maintenance is low. Although the yellow pomegranate looks drab during a
large part of the year, it turns into a spectacular showy sight after the first rains in spring or early
summer when it is covered in a mass of bright yellow flowers. When rain is sporadic it may have
several flushes of bloom.
25
Figure 2.6: Rhigozum obovatum (Pictured by Mrs E. Baxter)
2.6.5.1 Description
This is a much-branched, spiny shrub or small tree 1.0 - 4.5 m high. The leaves are opposite or in
a cluster, trifoliolate (compound leaf with three leaflets) or rarely simple, and they are borne on
short, spine-tipped side shoots. The leaflets are obovate (egg-shaped and widest at the tips), 5-13
x 2-5 mm, greyish green, often finely notched, the margin is entire, rolled under, and the petiole
is 2-6 mm long. The flowers are produced singly along the branches where the leaves emerge.
They are showy, bright yellow, tubular or funnel-shaped with 5 lobes. Flowers are followed by
fruits which are pendulous, flattened, pod-like capsules, up to 80 mm long, white brownish in
colour, and split along the flat surface when mature to release buff-coloured seeds with papery
wings.
2.6.5.2 Distribution
This beautiful plant grows in the central to eastern Karoo, extending into south-eastern Lesotho
and the Southern Free State. It often grows on rocky outcrops (koppies) in this summer rainfall,
but semi-arid region. While winters are cold, the plant is frost tolerant. It can be grown on the
highveld provided it is not over-watered and it will flower there and produce viable seed.
26
2.6.5.3 Derivation of name and historical aspects
Rhigozum is derived from the Greek rhigios meaning stiff and ozos, a branch, a reference to the
plant's rigid branches and obovatum is derived from the Latin word meaning egg-shaped with the
widest point near the tip, referring to the leaf shape.
2.6.5.4 Uses and cultural aspects
It is heavily browsed by game and stock.
2.6.6 Felicia muricata
Felicia muricata belongs to the family Asteraceae. It is locally known as Ubosisi in the Eastern
Cape of South Africa. This is a small drought resistant perenial herb growing up to 20cm in
height. The leaves are simple and are arranged in alternate fashion. Its name was derived from
muricate (rough, with sharp tubercles or protuberances). The species is regarded as an indicator
of desertification, becoming increasingly invasive in grassland regions (Jordan and Kruger,
1993).
Figure 2.7: Felicia muricata (Taken from www.zimbabweflora.co.zw/speciesdata/species.php?)
F.muricata is used by the traditional healers in the management of headaches, stomach catarrh,
pains and inflammation (Hutchings, 1989; Hutchings and Van Staden, 1994; McGaw et al.,
1997). Extracts from the plant have been reported to show 80-90% inhibitory activity against
cyclooxygenase, an important enzyme in the prostaglandin biosynthesis pathway (McGaw et al.,
1997; Okoli and Akah, 2004).
2.7 Traditional healers’ beliefs and practices
Traditional healers in South Africa are most commonly known as “inyanga” and “isangoma”.
These terms are used to refer exclusively to herbalist and diviner respectively, but in modern
27
times the distinction has become blurred, with some healers practising both arts. In addition to
the herbalists and diviners who are believed to be spiritually empowered, there are traditional
birth attendants, prophets, spiritual healers (Zulu: “abathandazi”), spirit mediums, intuitives and
dreamers. Most elderly folk in rural areas have knowledge of herbal lore, and function as firstaid healers with a family repertoire of herbal remedies or “kruierate” (Van Wyk et al., 1997).
Van Wyk et al. (1997) suggest that there is the magical, ritual, spiritual and symbolic aspects of
the use of indigenous medicinal plants which have not been much recorded. The informal oraltradition medical systems of the Khoi-San people, the Nguni and the Sotho-speaking peoples
have not yet been systematised, and are passed on by word of mouth from one generation to the
next. These medical systems and their herbal, animal and mineral materia medica have ancient
origins which may date back to palaeolithic times.
Traditional healers often unknowingly conserved their natural remedies by selective harvesting.
The bark of some trees could only be removed at one side of the trunk to “ensure healing of the
patient,” hereby preventing ring barking of the tree. Furthermore, bark that is used for treating
kidney diseases are sometimes only harvested from the eastern and western sides of the tree,
traditionally symbolizing the kidneys, thereby preventing ring-barking (Van Wyk et al., 1997).
Similarly, when a piece of bulb was to be cut from a bulbous plant, the new hole in the soil had
to be left open, in this way ensuring healing of the fresh wound in the plant tissue (Reyneke,
1971). In Gazankulu, a Shangaan taboo dictates that if the remaining root system of
Elephantorrhiza elephantine is not covered after a portion has been removed, the patients treated
with it will not get better.
Herbalists claim to use underground plant parts more frequently, believing that they contain the
highest concentration of potent healing agents (Shale et al., 1999). These slow growing storage
organs can normally be kept for longer periods, retaining their medicinal compounds for later
use.
In general, natives rely on wild plants instead of cultivated varieties, and traditional healers
normally prefer to work with freshly harvested material (Zschocke and Van Staden, 2000). More
collections of medicinal plants are made in areas with higher altitude, also called the ‘highlands’
(Shale et al., 1999). Traditional healing practices are usually specific regarding the plant parts
that should be used in disease treatment, as well as their appropriate usage. Almost any part of
28
the plant e.g. roots, bark, leaves, bulbs, rhizomes, tubers, stems, flowers, fruits, seeds, gums,
exudates and nectar, can be used for medicinal purposes. The choice of usage may depend on the
nature of disease, characteristics of certain plants and the recommended method of
administration (Van Wyk et al., 1997). The most common methods of administering plant
medicines are outlined as orally, sublingually, rectally, topically, nasally, smoking, steaming and
bathing (Van Wyk et al., 1997).
It might be interesting to study the traditional combination of one plant part added to another
substance. This combination is used to treat women of various ailments. Examples of the plants
used are: Achyranthes aspera, Cassia auriculata, Dichrostachys cinerea and Sida acuta, all of
which are mixed with onions, Blepharis madaraspatensis with limestone, Leucas aspera with
garlic, and Phyllanthus amarus with goat’s milk. The reason as to why the plant parts are mixed
with other substances and administered by local/indigenous people is unclear (Bhanumanthi et
al., 1999). When Chironia baccifera is combined with Peucedanum galbanum (wildeselery), it
makes a well-known Cape remedy for arthritis (Pvt. Daniels, pers. comm.). Chironia baccifera
and C. palustris have been used for colic and diarrhoea in children. While under the name
Pentzia virgata, Pentzia incana has been used in the Western Cape districts, with Tarchonanthus
camphorates and possibly also with Pentzia globosa, as a poultice on the chest for the relief of
bronchitis (Kling, 1923). A number of interesting outcomes have been found with the use of a
mixture of natural products to treat diseases, most notably the synergistic effects and
polypharmacological application of plant extracts (Gibbons, 2003). Scientific investigation
should be conducted in this direction (Bhanumanthi et al., 1999).
2.8 Poisonous plants
The subject of the toxicity of medicinal plants is very topical and at the center of passionate
debate. Because of this concern, many healers have been treated like poisoners or witches.
Today, to protect its citizens, governments have prepared a list, sometimes arbitrary, of the plants
they consider to be dangerous, prohibiting their cultivation, processing and sale. Although herbs
appear to be harmless and beneficial to everybody, numerous toxic compounds were found in
remedies such as deadly nightshade and jimson weed (Dantra). Medicinal plants collected from
the wild may be contaminated by other species or plant parts through misidentification (WHO,
2003). Poisoning from traditional medicines is frequently a consequence of misidentification
29
(Stewart et al., 1998). Poisonings by traditional plant-based remedies in South Africa is not
uncommon, particularly in children (Stewart et al., 1999; Steenkamp et al., 2002). Nonetheless,
medicinal personnel tend not to ask about the use of traditional medicines administered to young
children, especially not babies (Van Wyk and Els, 2008). A recent case study reported a single
case of neonatal organo-phosphate-like poisoning, presumed to be caused by traditional
medicine. The traditional healer was contacted and a sample of the traditional medicine
administered to the child was sent for analysis. Unfortunately, the specimen was misplaced
during transfer and no analysis could be performed (Van Wyk and Els, 2008).
Some medicinal herbs contain toxic compounds such as pyrrolizidine alkaloids (e.g. species of
Crotalaria, Heliotropium, Senecio, Symphytum), which may cause liver toxicity and cancer or
venocclusive disease. Other toxic compounds present in some herbal plants include lectins,
toxins, lignans, saponins, diterpenes, and cyanogenetic glycosides. Contrary to popular belief,
herbs may cause adverse reactions including allergic, cardiac, endocrine, and irritant effects.
There is also the possibility that herbal treatment may interact with other medicines, for example
if a herb lowers blood pressure or increases blood coagulation time or is a sedative, then it may
interact with concurrent antihypertensive, anticoagulant or sedative therapy (Newall et al., 1996).
The deliberate addition of biologically active material to a plant preparation (known as
adulteration) is a common method of malpractice used to enhance the efficacy of the products
(Yee et al., 2005). There had been no reports of deliberate adulteration of traditional African
herbal remedies until recently with reports of two separate incidences in which South African
traditional remedies were adulterated with Western pharmaceuticals causing severe toxicity
(Snyman et al., 2005).
It is certainly useful to clear the most dangerous plants and to avoid contact with them or to
avoid using them, but it is important to remember that they merit our respect and the right to live.
Indeed, they often contain highly concentrated active principles that are sometimes useful in
small doses for an expert in pharmacognosy (Schneider, 2002).
More recently, mainly in the last century, the Western World, with its new inventions and
technology, succeeded to distinguish between toxic or ineffective plant remedies, and those that
proved to be pharmacologically useful (Lall, 2000). Results from these investigations provided
significant scientific support for the traditional usage of plants, leading to an increasing trust in
30
the rich heritage of knowledge left behind by native folklore (Hutchings et al., 1996; Lin et al.,
1999; Shale et al., 1999; Kelmanson et al., 2000).
The prescription and use of traditional medicine in South Africa is currently not regulated, with
the result that there is always the danger of misadministration especially of toxic plants. The
potential genotoxic effects that follow prolonged use of some of the more popular herbal
remedies, are also cause for alarm (SATMERG, 1999).
Many South African medicinal plants are harvested from the wild. This not only threatens
medicinal plant biodiversity and population stability but also leads to speculations with regard to
safety as industrial encroachment has led to contamination of water sources and natural habitats.
The deposition of processed and unprocessed mining and industrial waste materials (Naicker et
al., 2003; Roychoudhury and Starke, 2006) have led to questions of safety for South African
medicinal plants that are harvested near to these resources. According to Verster et al. (1992)
large quantities of polluted water and tones of dry sewage sludge is being disposed on South
African soils, much of this on agricultural land. Numerous reports have revealed heavy metal
contamination of South African rivers and soils (Abbu et al., 2000; Binning and Baird, 2001;
Okonkwo and Mothiba, 2005). As a result of polluted harvest sites or poor farming practices,
medicinal plant products may be contaminated with pesticides, microbial contaminants, heavy
metals, toxic substances and adulterants (Chan, 2003).
2.9 Mutagenic effect
Mutagenesis is observed as reversion to the histidine prototroph, i.e. mutated organisms are
capable of growing in the absence of exogenous histidine (Maron and Ames, 1983; Wall et al.,
1988). Salmonella typhimurium tester strains contain mutations in the histidine operon, thus
making them dependent on histidine for growth. In addition, the tester strains contain mutations
in certain repair systems, and this greatly increases their ability to detect mutagens (Maron and
Ames, 1983). Strain TA98, which detects compounds causing various frameshift mutations, and
strain TA100, which detects mutagens causing base-pair substitutions, are most often used
(Maron and Ames, 1983; Wall et al., 1988).
There is a continuous search for new medical preparations against a great number of ailments,
including cancer. This is because existing medication often has unwanted side effects or because
31
of loss of efficiency in the long run. Epidemiological studies indicate that many cancers are
dependent on multiple mutational etiologies, as well as on inherited mutator phenotype. The
search for inhibitors of mutagenesis may therefore be useful as a tool to discover
anticarcinogenic agents. The approximately 25,000 plant species of South Africa form a potential
pool for the screening of new anti-tumour compounds. Such screening may include the screening
for inhibitors of mutagenesis. Screening traditional medicinal plants that have been used for ages
against several illnesses, including cancer, and that proved to be efficient in curing people may
be one way to narrow the search (Van Wyk et al., 1997).
Recently, there has been considerable interest in mutagenicity (Elgorashi et al., 2002-2003) and
antimutagenicity (Verschaeve et al., 2004) of medicinal plants used by traditional herbalists.
Previously, the possible mutagenic effects of 51 South African species frequently used in
traditional medicine, were reported (Elgorashi et al., 2003). Frequently used plants in traditional
medicine are assumed safe, due to their long-term use (Elgorashi et al., 2002) and are considered
to have no side effects because they are “natural” (Popat et al., 2001). This concept is largely
circumstantial and it is important to determine toxicology of plant extracts, especially those that
are used frequently over long periods. As new natural compounds come on the market in drug
form as industrial and agricultural inputs, their toxic or genotoxic action on man or on genetic
material must increasingly be evaluated to prevent the use of substances that could interact and
cause severe cellular and molecular organization disorders. Genetic assays used in these studies,
especially the Salmonella/microsome test, allow faster screening of these mutagenic and
probably carcinogenic substances at a lower cost (Mortelmans and Zeiger, 2000). The Ames test
(Maron and Ames, 1983) was used in this study as it is widely used in the determination of
possible gene mutations caused by plant extracts. A positive response in any single bacterial
strain either with or without metabolic activation is sufficient to designate a substance as a
mutagen (Zeiger, 2001).
It is important to note that most of the traditional medicinal plants have never been the subject of
exhaustive toxicological tests such as is required for modern pharmaceutical compounds. Based
on their traditional use for long periods of time they are often assumed to be safe. However,
research has shown that a lot of plants which are used as food ingredients or in traditional
medicine have in vitro mutagenic (Cardoso et al., 2006; Déciga-Campos et al., 2007) or toxic
and carcinogenic (De Sá Ferreira and Ferrão Vargas, 1999) properties.
32
Plants sometimes synthesize toxic substances, which in nature act as a defence against infections,
insects and herbivores, but also may affect the organisms that feed on them. An assessment of
cytotoxic and mutagenic potential of extracts used in traditional medicine is necessary to ensure
their safe usage (Cavalcanti et al., 2006).
2.10 The concept of Western medicine versus Traditional medicine
Herbs and plants were used as the very first medicinal therapies known to man. With time, the
original inhabitants of an area gained knowledge as to which plants could be used for certain
disease or states of illness. In addition, they also gained knowledge of which plants were
hazardous or poisonous. The very first original pharmacy, in fact, was Mother Nature, with her
expensive variety of medicinal plants (White and Foster, 2000). Knowledge of the plants used in
the preparation of remedies was not in the public domain. Many treated it as a secret to be
guarded closely (Masika et al., 2000).
Literature by Felhaber (1999) discusses Southern African traditional healers and their belief that
healing rests on the assumption that if the mind is healed, the body takes care of itself. Whereas
in Western medicine, the opposite is often considered true: If the body is healed, the mind takes
care of itself. According to research by Hewson (1998), a growing number of articles show that
physicians can improve their clinical effectiveness by adopting the traditional approach of
embracing both physical and mental aspects of illness.
Felhaber (1999) also explains that the main method of alternative healing is to work WITH the
body instead of working AGAINST the disease, as is the case with Western therapies. Rather
than fighting against bacteria, an attempt is made to enhance the body’s own built-in defence
mechanism.
Health is defined by the WHO as a complete state of physical and mental well-being, and not
merely the absence of disease or infirmity. This definition is in line with the practice of
traditional healers who look at the whole body (physical, mental, spiritual), whereas biomedicine
heals only the affected parts of the body and is forever looking for germs (Kubukeli, 2000).
Western medicine may diagnose a disease in terms of a bacterial infection for example, and treat
that infection effectively with antibiotics. An African traditional healer will seek to understand
why the patient became ill in the first place, and the treatment administered will address the
33
perceived cause, usually in addition to specific therapies to alleviate the signs and symptoms of
the condition (Van Wyk et al., 1997).
Although traditional and Western therapies are usually seen as opposing entities, they actually
have quite a lot in common: an approximate amount of pharmaceutical products sprout directly
from medicinal plants; these plants and pharmaceutical products, contain healing agents that can
change body processes. That is the reason why these compounds are used as medicine in order to
transform the body from a state of illness and disorder to a state of emotional and physical health
(White and Foster, 2000).
Felhaber (1999) has formed the opinion that there are few areas for collaboration between
traditional healers and modern medicine. This is an unfortunate situation, because traditional
healers perform an important role in the delivery of health care, especially in rural areas where
access to Western medical care is limited. In contrast, Taylor and Van Staden, (2001) explains
that the evaluation and authentication of traditional medicine can contribute towards the
formulation of an integrated health care system combining both traditional and Western
practices.
2.11 Methods of diagnosis and treatment of disease
Table 2.2: Western versus Traditional Diagnosis and Treatment
Western Diagnosis
Traditional Diagnosis
Diagnosis of illness in a patient is based The diagnostic process investigates how
upon:
the disease originated (in relation to natural
• The patient’s medical history;
causes), and why the disease is manifesting
• A physical examination of the patient or
itself (the deeper meaning or motivation
• Any special investigations or tests that behind the causes).
are thought to be necessary by the Diagnosis is made after combining
medical practitioner to assist in the information gathered from observing the
successful treatment of the patient.
patient, patient self-diagnosis and
divination or spiritual guidance.
Western Medicine
Traditional Medicine
Antibiotics are used to treat infectious Traditional treatment has elements of being
34
diseases. They must be taken for the entire curative, protective and preventive, and can
length of time for which they have been either be natural or ritual, or both.
prescribed. Stopping the drug before the Formulas are prepared from various natural
prescribed time can cause bacteria that are substances (animal, mineral and vegetable)
resistant to the drug to grow out of control, and can be applied in various ways
which makes treating the illness even more according to the body site and severity of
difficult the second time.
the illness.
(Compiled from: Felhaber, 1999; Gould & Mackenzie, 2002; Maher, 1999)
In the context of Nguni people’s perception, illness is a condition of internal corruption
(accumulation of toxins) and ‘uncleanliness’ (Hutchings, 1989b). As a result, many herbal
medicines were found to seek the cleansing of the inner system of the patient by inducing
purging and vomiting (Masika et al., 2000).
2.12 Methods of preparation and administration of traditional remedies
The methods of preparation are critical, as it includes the amount of fresh or dry plant material to
be used, the addition of appropriate volumes of solvents such as water or alcohol, and additional
activities such as boiling for a specified length of time, or partial burning to achieve a desired
colour. The common forms and methods of preparation are enemas, extracts, infusions,
decoctions or teas, inhalations, snuffs, linctuses, tinctures, lotions, liniments, mixtures, ointments
and nasal drops. For internal use, the preparation is mostly prepared as a tincture, decoction or
infusion. For external use, the powder or the juice of the plant can be directly applied on the
wound or introduced in incisions (Van Wyk et al., 1997).
The most common methods of administering plant medicines are orally (mainly infusions,
decoctions, syrups and tinctures, powdered herbs, partially burned herbs or the ash of burned
herbs taken directly by mouth, usually followed by a mouthful of water), sublingually (under the
tongue), rectally (infusions and decoctions are commonly administered as enemas), topically,
nasally, smoking, steaming and bathing (Van Wyk et al., 1997). In administering Harpephyllum
caffrum by traditional healers, it is first given as a facial steaming, then as a phalaza, and then
orally as an imbiza daily. The bark is used fresh and can be collected in any season (Van Wyk
and Gericke, 2000).
35
Modern pharmaceuticals are typically oral dosage forms containing single synthetic chemicals
that have potent clinical activity. However, natural products from higher plants continue to be
used in pharmaceutical preparations either pure or as extracts (Gogtay et al., 2002).
2.13 The study area
South Africa boasts with a unique and diverse botanical heritage with over 30,000 plant species
of which 3,000 species are used therapeutically (Van Wyk et al., 1997). Not only is the South
African flora rich in diversity but it is also mostly endemic (Mulholland, 2005). In addition to
this unique botanical heritage, South Africa has a cultural diversity with traditional healing being
integral to each ethnic group. African traditional medicine is the oldest medicinal system, often
culturally referred to as the Cradle of Mankind (Gurib-Fakim, 2006).
The Eastern Cape Province in South Africa, falls within the latitudes 30o00'- 34o15'S and
longitudes 22o45' – 30o15'E. It is bounded by the sea in the East and the drier Karoo (semi-desert
vegetation) in the west. The elevation ranges from sea-level to approximately 2,200m in the
north of the province (Grierson and Afolayan, 1999). To the north-west the province borders on
KwaZulu-Natal and meets the southern tip of the Drakensberg range; further south, mountains
and hills predominate, the northern section in the dry karoo being flatter. The long curve of
coastline, large area (at nearly 170,000 square kilometers covering 13.9% of the country) and the
considerable east-west and north-south distances it covers, and the vegetation is veld type
number 7, known as the Eastern Cape thorn veld (Acocks, 1975). The coastal areas receive good
summer rainfall and have a moderate climate, becoming more sub-tropical to the north-west.
According to a study by Hostettmann et al. (2001), plant species growing in a hostile
environment (such as warm and humid conditions) will attempt to protect itself by synthesizing
insecticidal, fungicidal, antibacterial or virucidal constituents, e.g. roots often synthesize
antifungal substances as soil is rich in pathogenic fungi.
36
CHAPTER 3: RESEARCH METHODOLOGY
3.1 Introduction
The current chapter discusses the materials and methods used in the sampling of Harpephyllum
caffrum, Chironia baccifera, Hermannia cuneifolia, Pentzia incana, Rhigozum obovatum and
Felicia muricata plant materials, as well as performance of antimicrobial activity screening of
the respective extracts of plants using four testing methods. The agar diffusion method using the
Mast multipoint inoculator, the determination of minimum inhibitory concentration using
microtitre plates, thin layer chromatography fingerprints used to detect the inhibition of bacterial
growth by active compounds separated from plant extracts, and the Ames test required to assess
the possibility of bacterial mutagenesis upon exposure to plant extracts which can lead to
carcinogenicity, are also discussed.
3.2 Sampling technique
Renewed interest in traditional pharmacopoeias has meant that researchers are concerned not
only with determining the scientific rationale for the plant’s usage, but also with the discovery of
novel compounds of pharmaceutical value. Instead of relying on trial and error, as in random
screening procedures, traditional knowledge helps scientists to target plants that may be
medicinally useful (Cox and Balick, 1994). Although there are other approaches of selecting
plant species for biological investigation, selecting species that are used in traditional medicine is
reported to be more valuable and many drugs that are of plant origin were discovered from plants
used in traditional medicine (Cotton, 1996). The investigated plants were selected on the basis of
their reported ethnobotanical use in South African traditional medicine and on availability
(Hutchings et al., 1996; Van Wyk et al., 1997). The materials were collected in the Eastern Cape
Province during the summer months. In their work, Mitscher et al. (1972) found that extracts are
generally richest in antibacterial agents after the flowering (sexual) stage of their growth is
complete, and that plants taken from stressful environments were particularly active.
In this study the following plants were chosen, Harpephyllum caffrum, Chironia baccifera,
Hermannia cuneifolia, Pentzia incana, Rhigozum obovatum and Felicia muricata, because of
their traditional medicinal use as well as pasture for livestock. In this part of the world, people do
not only use traditional medicine for their own welfare, but also for that of their animals. A
37
previous study has shown that almost 75% of resource-limited livestock owners use traditional
medicine to treat animal ailments (Masika et al., 2000).
3.3 Plant preparation, extraction and methods.
3.3.1 Preparation
Herbalists use various methods to prepare herbal remedies. One method is preparation of
infusions, where the plant parts are soaked in water, and left for some time to allow the active
ingredients to infuse into the water. Another method involves the preparation of decoctions
whereby the plant material is boiled in water. Other remedies are prepared in a powdered form
by grinding dried or roasted plant material. Pastes are made by mashing fresh plant parts. Other
medicines consisted of juices obtained by pressing the sap out of fresh leaves, stems, flowers and
other plant parts (Masika et al., 2000).
Proper drying conditions are largely overlooked by the collectors, growers and traders
(Ramakrishnappa, 2002). Inadequate drying may result in mould growth (Whitten, 1997), which
can lead to deterioration of the plant product (Ramakrishnappa, 2002). Yeasts and moulds can
cause opportunistic infections in humans and are more significant in HIV patients (Govender et
al., 2006). Hence great care was taken during the drying process.
Plant materials were dried in an oven at 40oC and weighed. Dried material is preferred in cases
where there is a delay between collection and processing. Unlike fresh material in which the
interfering water content can pose problems in subsequent processing by liquid-liquid extraction,
dry material has fewer problems with large-scale extraction (George et al., 2001). Mahanom et
al. (1999) evaluated three different drying methods that are routinely used in the detection of
physiologically active substances (PAS). These are:
• Oven drying at 70oC for 5 hours,
• Oven drying at 50oC for 9 hours and
• Freeze drying
The research concluded that drying treatments caused significant reduction in the levels of all
phytochemicals analysed. Oven drying caused greater reduction compared to freeze-drying.
Freeze-drying resulted in the lowest percentage losses of all the phytochemicals analysed,
followed by oven drying at 70oC and oven drying at 50oC.
38
Harborne (1998) advises that the drying procedure should be carried out under controlled
conditions to avoid too many chemical changes occurring. Plant materials should be dried as
quickly as possible, without using high temperatures, preferably in a good air draft. Once
thoroughly dried, plants can be stored for long periods of time.
Figure 3.1: Powdered leaves of Rhigozum obovatum
The dried plant parts were powdered using a pestle and mortar. Powdering of the plant material
increases the surface area accessible to the solvents, which results in better extraction (Harborne,
1998; George et al., 2001).
3.3.2 Plant Extraction
Extraction methods used pharmaceutically, involve separation of medicinally active portions of
plant tissues from the inactive/inert components by using selective solvents with appropriate
extraction technology. During extraction, solvents diffuse into the solid plant material and
solubilise compounds with similar polarity (Green, 2004).
An extraction method adapted from Eloff (2000) was employed using approximately 2g of dried
plant leaves, bark or stem for the six plants. Choosing a solvent for extraction depends on the
aim of the screening. For instance antibacterial screening of plants requires no interferences by
the solvent, in the bioassay procedure (George et al., 2001). A publication by Eloff (1998b)
identified acetone as the most favourable solvent for plant extraction in antimicrobial studies.
Plant extracts tested with methanol have proved valuable, as a high percentage of antibacterial
activity is present (Rabe and Van Staden, 1997). The solvents chosen for this study were acetone,
methanol because of low toxicity, ease of evaporation at low heat, promotion of rapid
39
physiologic absorption of the extract, preservative action and inability to cause the extract to
complex or dissociate (Hughes, 2002) and sterile distilled water.
The extraction procedure was performed as follows with the dried plant material:
• Weighed 2g of plant material and 30ml of each solvent, were placed in screw cap tubes,
respectively and shaken vigorously for 5 min.
Figure 3.2: Centrifuged extracts in the respective solvents
• Centrifugation of different extracts in tubes at 4000rpm for 5 min using the Eppendorf
centrifuge 5810 separated the supernatant from the plant material for each extract.
• Supernatant of each plant extract was transferred into pre-weighed beakers.
• Procedure was repeated twice more for re-extracting the remaining plant material with
additions of 30ml solvent, respectively.
•
The pre-weighed beakers containing the plant extract supernatants were allowed to dry
completely to obtain a solvent-free dried extract residue.
Figure 3.3: Centrifuged extracts in evaporating beakers
40
•
Methanol and acetone plant extract supernatants were subjected to overnight drying
under airflow in a fume cupboard.
•
Incomplete drying of the aqueous plant extract supernatants prompted alternative drying
at 37oC overnight.
•
Dried beakers were re-weighed and calculated extract residues resuspended in Dimethyl
Sulphoxide (DMSO).
•
Plant extract concentrations were standardized between the different plants and solvents
used for extraction.
According to Mathekaga and Meyer (1998), in vitro screening methods could provide the needed
preliminary observations necessary to select crude plant extracts with potential useful properties
for further chemical and pharmacological investigations.
3.3.3 Assays
The antimicrobial susceptibility test (AST) is an essential technique in many disciplines of
science. It is used in pathology to determine resistance of microbial strains to antimicrobials, and
in ethnopharmacology research, it is used to determine the efficacy of novel antimicrobials
against microorganisms, essentially those of medical importance. The test is the first step
towards new anti-infective drug development. There are various AST methods that are employed
by researchers and these could lead to variations in results obtained (Lampinen, 2005). Other
factors impacting on methods have been studied which include storage of plant material and its
effect on microbial efficacy (Eloff, 1999; Stafford et al., 2005).
Figure 3.4 below represents the proportion of studies and the methods used to assess
antimicrobial activity mostly for the period 1997 – 2008. The two most common methods used to
investigate the antimicrobial activity of South African medicinal plants are disc diffusion and
minimum inhibitory concentration (MIC) assays. Initially disc diffusion studies were the first
method of choice, possibly due to their simplicity and capacity to analyse a large number of test
samples. Many earlier publications (65.0% before 2004) used this method as a means of
determining activity (Van Vuuren, 2008).
41
Figure 3.4: Methods used for antimicrobial investigation versus No. of Publications
(Compiled by Van Vuuren, 2008)
Essential oils possess biological activity including antibacterial, antiviral, antifungal and antiinflammatory effects. Oils from Cinnamomum osmophloeum have been shown to possess
antibacterial activity against Escherichia coli, Enterococcus faecalis, Staphylococcus aureus
(including methicillin resistant S.aureus) and Vibrio parahaemolyticus, with cinnamaldehyde
being the main antibacterial component isolated. This compound has also been widely used in
antiseptic mouthwashes because of its activity against oral bacteria (Wallace, 2004).
The bacteria and fungi selected for investigation in this study were isolated from patients
diagnosed with septicaemia. The following ATCC strains and microorganisms from clinical
isolates were used: Escherichia coli (ATCC 35218); Bacillus cereus (ATCC 10876);
Staphylococcus
aureus
(ATCC 43300); Candida albicans (ATCC 66027); Pseudomonas
aeruginosa (ATCC 27853); Enterococus faecalis (ATCC 29212); The clinical isolates included
one strain of the following bacteria: Streptococcus bovis; Enterococcus faecalis; S. group b;
Methicillin Resistant Staphylococcus epidermidis; Staphylococcus hominis; Staphylococcus
Coagulase Negative; Providentia stuartii; Leuconostoc pseudomesenteroides; Enterobacter
agglomerans; Acinetobacter baumanii; Acinetobacter haemolyticus; Acinetobacter lwoffii;
Candida krusei; Candida lusitaniae; Staphylococcus haemolyticus and Aeromonas hydrophila;
plus 7 strains of Methicillin Resistant Staphylococcus aureus (MRSA); 2 strains of Klebsiella
pneumoniae; 5 strains of Klebsiella oxytoca; 5 strains of Salmonella species; 2 strains of
Enterobacter cloacae and 7 strains of Candida albicans. Each organism together with the ATCC
42
strains were stored in cryotubes (microbank™) supplied by Davies Diagnostics and were
subcultured onto specific culture media and incubated at 37oC overnight before testing.
3.3.3.1 Agar diffusion method
Mueller-Hinton (MH) agar was prepared according to the manufacturer’s directions and
autoclaved, allowed to cool to about 50oC before the addition of the extracts. The extracts were
prepared by dissolving in a known amount of DMSO per plate (0.4% V/V). Each plant extract
was carefully added into 25ml Mueller-Hinton agar to obtain the final agar plate concentration of
10mg/ml. These were poured into Petri dishes, swirled carefully until the agar begun to set and
left overnight for the solvents to evaporate (Afolayan and Meyer, 1997). The ATCC strains and
the clinical isolates were recovered for testing by growth in nutrient broth overnight at 37oC.
Nutrient broth was subcultured onto solid agar. A standardized inoculum was prepared by
suspending colonies in normal saline and adjusting the density to that of a 0.5 McFarland
standard solution (McFarland, 1907) which is equivalent to 106-108 CFU/ml. The final volumes
of 30μl prepared inoculums were transferred into each well of the sterile inoculum pots.
Antimicrobial activity of the tested microorganisms was carried out by the use of Mast
multipoint inoculator (Mast systems, London, UK) based on the principles of agar dilution
(Andrews, 2001) and plates were incubated at 37oC for 24 to 48 hrs.
Figure 3.5: Mast Multipoint Inoculator
Agar plates containing 0.5ml of acetone, methanol or DMSO were used as controls respectively.
Tests were performed in triplicate. Complete suppression of growth was required for an extract
to be declared active.
43
3.3.3.2 Determination of minimum inhibitory concentration
The most prominent South African publication (Eloff, 1998a), dedicated to antimicrobial
methods, is the quick, sensitive microtitre plate minimum inhibitory concentration determination
method, which has been extensively cited. Although the results of the agar diffusion assay cannot
always compare to the MIC data (Njenga et al., 2005), three extracts of plants namely
Harpephyllum caffrum, Hermannia cuneifolia and Chironia baccifera, which showed positive
antimicrobial activity against some of the microorganisms tested in the agar diffusion bioassay
were further tested for the determination of MIC. Dried plant extracts were dissolved at 50mg/ml
with the extracting solvents. All extracts were initially tested at 25mg/ml in 96-well microtitre
plates and serially diluted two-fold to 0.049mg/ml, after which 50µl bacterial culture was added
to each well. Each extract was tested against Escherichia coli (ATCC 35218), Bacillus cereus
(ATCC 10876), Staphylococcus aureus (ATCC 43300), Candida albicans (ATCC 66027),
Pseudomonas aeruginosa (ATCC 27853), Enterococcus faecalis (ATCC 29212) and 73
microorganisms from clinical isolates.
Bacterial culture strains that were subcultured on nutrient agar and placed in an incubator
overnight at 37oC, were prepared by suspending colonies in MH broth and adjusting the density
to that of a 0.5 McFarland standard prior to use in the bioassay. Extract-free solution was used as
a blank control. The microtitre plates were incubated overnight at 37oC. As an indicator of
bacterial growth, 40 µl p-iodonitrotetrazolium violet (INT) dissolved in water was added to the
wells and incubated at 37oC for 30 minutes. MIC values were recorded as the lowest
concentration of the extract that completely inhibited bacterial growth. The colourless
tetrazolium salt acts as an electron acceptor and is reduced to a red-coloured formazan product
by biologically active organisms (Eloff, 1998a). Where bacterial growth was inhibited, the
solution in the well remained clear after incubation with INT.
Table 3.1: Microtitre plate layout with plant extracts
Rows
Columns
•
A: Undiluted extract
•
1-3 Methanol extract
•
B: 1 in 2 dilution
•
4-6 Acetone extract
•
C: 1 in 4 dilution
•
7-9 Aqueous extract
•
D: 1 in 8 dilution
•
10-12 Sterility controls
44
•
E: 1 in 16 dilution
•
F: 1 in 32 dilution
•
G: 1 in 64 dilution
•
H: Positive Growth Controls
3.3.3.3 Thin Layer Chromatography (TLC) fingerprints
TLC is a type of liquid chromatography in which the stationary phase is a thin (~0.25mm)
uniform coating of a solid fine material spread, on a glass plate, aluminium foil, or plastic sheet
(Sherma and Fried, 2005) is utilized in a manner similar to that of the paper in paper
chromatography (Voet and Voet, 2004). It is recommended for the quality control of Traditional
Chinese Medicine (TCM) in the Chinese Pharmacopoeia (Committee of National
Pharmacopoeia, 2005). It is quick, convenient, and cost effective technique widely used for
pharmaceutical analyses. TLC has the special ability to assay many samples at the same time on
a single plate (Li, et al., 2004). It is recommended as an effective method for identification of
plant derivatives by Chinese, American and European Pharmacopoeias (Fuzzati, 2004). TLC
enables reliable separation and analysis of compounds from a wide variety of classes in many
types of biological samples (Sherma and Fried, 2005).
The plant extracts and herbal medicinal products are usually highly complex samples, and in
most cases it is difficult to identify all compounds by means of common approaches (e.g. onedimensional liquid chromatography). However, there are many methods, in which traditional
techniques are used in the analysis of complex samples. These methods are usually focussed only
on some components of which the identity is known, regarding them as “marker compounds”
(Chen et al., 2006). Contrary to synthetic drugs and isolated natural products the entire plant
extracts should be regarded as active components, so the aforementioned method may sometimes
appear insufficient in the quality control of highly complex natural samples (Cieśla and
Waksmundzka-Hajnos, 2009).
3.3.3.3.1 Materials and Techniques
The TLC fingerprints of different extracts were prepared by spotting 0.5 mg of methanol,
acetone and water extracts as a 1cm band onto a large TLC plate (silica gel 60 F 254 , 0.25 mm,
20cm×20cm, Merck).
45
The plates were developed in petroleum ether: ethyl acetate: chloroform: formic acid (8:7:5:1),
over a distance of 17 cm. Once the extracts were separated by TLC and the solvent evaporated,
the separated components were visualised under visible and ultraviolet light UV 300 using the 300
series Foto UV transilluminators (Gibbons and Gray, 1998).
BIOAUTOGRAPHY ASSAY: During the extraction and purification procedure, bioautography
assays (Slusarenko et al., 1989) were performed on TLC plates using the ATCC strains. An
inoculated layer of Mueller-Hinton broth was sprayed with fresh culture of bacteria over a
developed TLC plate and incubated for 24 to 48hrs at 37oC in a moist environment. As an
indicator of bacterial growth, 0.2mg/ml INT solution was sprayed over the plate and incubated at
37oC for 30 min. The inhibition of bacterial growth by compounds separated on the TLC plate
was visible as white spots against a grey background. The white spots on the front of the mobile
phase were used to calculate the R f values (= distance of travel of the zone divided by the
distance of the mobile phase front) (Sherma and Fried, 2005).
3.3.3.4 The Ames test
The Ames test assay is a rapid and effective bacterial assay for carcinogenicity that is based on
the high correlation between carcinogenesis and mutagenesis (Voet and Voet, 1995). The Ames
test (Maron and Ames, 1983; Mortelmans and Zeiger, 2000) is a well-known bacterial
mutagenicity test. In this test reverse His- → His+ mutations are visualised by plating Salmonella
typhimurium bacteria in a histidine poor growth medium. In this medium only His+ mutants are
able to form visible colonies. Different bacterial strains are available to identify different types of
mutations. Strain TA98 gives an indication of frame-shift mutations, while a positive response
from strain TA100 indicates base-pair substitution. For a substance to be considered genotoxic in
the Ames test, the number of revertant colonies on the plates containing the test compounds must
be more than twice the number of colonies produced on the solvent control plates (i.e., a ratio
above 2.0). In addition, a dose-response should be evident for the various concentrations of the
mutagen tested.
The procedure of the Ames test as performed is described in Elgorashi et al. (2003), Verschaeve
et al. (2004) and Reid et al. (2006). Stock solution of Salmonella typhimurium bacteria
(100µl/ml) in 20ml Oxoid nutrient broth were incubated for 16hrs at 37oC. The bacterial cultures
(500μl) were added to 500µl of plant extract in 1000μl phosphate buffer and 10ml of agar
containing histidine (0.5mM). The mixture was poured on a Davis minimal agar plate and
46
incubated at 37oC for 48hrs. Samples were tested in triplicate. Two dilutions (200 and 600µg/ml)
of histidine were used per sample. 4-Nitroquinoline-N-oxide (4-NQO) was used as a positive
control. Bacterial colonies were counted at the end of 48hrs. Results are expressed as means of
three independent experiments.
The Salmonella typhimurium strain TA100 (ATCC 49416) was bought from MicroBiologics.
The strain was subcultured on nutrient agar prior to the assay at Nelson Mandela Metropolitan
University (NMMU) Microbiology laboratory and it was confirmed using the Analytical Profile
Index (API) method inorder to rule out possible contamination.
Figure 3.6: Salmonella typhimurium reaction on API Kit
A disadvantage of the Ames test is that any one strain is not able to detect all classes of
mutagens. Therefore, it may be necessary to use several strains in a single assay, and this might
not be practical for certain screening programs (Skopek et al., 1978). In this study,
Harpephyllum caffrum and Hermannia cuinefolia were the plants that were selected for Ames
test because of their marked inhibitory activity in the agar difusion and serial dilution methods.
47
CHAPTER 4: RESULTS
4.1 Introduction
In chapter 3, the author discussed the materials and methods used in sampling, preparation,
extraction and antimicrobial testing. This chapter will look at the outcomes of the assays
performed.
4.2 Agar diffusion method
An extract is considered having antimicrobial activity with a specific solvent if it inhibits a
particular microorganism in all the three runs performed at 10mg/ml concentration. The results
of water, methanol and acetone extracts are presented in Tables 4.1 to 4.7 below. Generally,
Gram-negative bacteria have been reported to be more resistant to plant extracts than the Grampositive strains (Rabe and Van Staden, 1997; Grierson and Afolayan, 1999; Afolayan, 2003).
Harpephyllum caffrum, Chironia baccifera and Hermannia cuinefolia are the only plants whose
extracts inhibited some bacteria in the tables below.
Figure 4.1: Agar plate containing extracts of Pentzia incana showing slight inhibition of bacteria
The comparison of the plate with acetone extract of P.incana (left) to the growth control (right)
shows slight inhibition of the inoculated microorganisms. The left plate: observing the diameter
of colonies from the far left vertical line where there are four colonies to the third vertical line
48
where there are six colonies, the top most colony (B.cereus) has been markedly reduced in
diameter (slightly inhibited) due to the addition of the P.incana acetone extract.
Figure 4.2: Agar plates containing extracts of P.incana, F.muricata & H.cuneifolia
In figure 4.2 above, the top two plates contained acetone and methanol extracts of P.incana at a
concentration of 10mg/ml. The activity of the extracts showed slight inhibition as compared to
the two middle plates which contained methanol and acetone extracts of F.muricata that showed
no activity after 48 hours incubation. In contrast, methanol and acetone extracts of H.cuneifolia
49
inhibited four strains of B.cereus, one strain of Candida albicans, three Staphylococcus species
and three strains of Staphylococcus aureus as shown by the last two plates at the bottom of figure
4.2.
Figure 4.3: Agar plate containing methanol extracts of H.cuneifolia compared with the control plate
In figure 4.3 above, the plate at the right with large colonies is the growth control while the plate
at the left contained methanol extracts of H.cuneifolia which inhibited some microorganisms.
Figure 4.4: Agar plate containing acetone extracts of H.cuneifolia compared with the control plate
50
Figure 4.4 above, is a comparison of the growth control to acetone extracts of H.cuneifolia. It
shows inhibition of microorganisms as in figure 4.3 of methanol extracts.
Figure 4.5: Agar plate containing aqueous extracts of H.cuneifolia compared with the control plate
Lack of antimicrobial activity in aqueous extracts of H.cuneifolia has been shown by the two
plates in figure 4.5. All the microorganisms grew almost like the growth control after 48 hours
incubation.
Table 4.1: Antimicrobial results of Hermannia cuneifolia extracts
Number
Strain
H.cuneifolia 1st run
H.cuneifolia 2nd run
H.cuneifolia 3rd run
{10mg/ml}
{10mg/ml}
{10 mg/ml}
Bacteria Name
W
M
A
W
M
A
W
M
A
1
973723
A. baumannii
+
+
+
+
+
+
+
+
+
2
984736
A. haemolyticus
+
+
+
+
+
+
+
+/-
+/-
3
987221
A. lwoffi
+
+
+
+
+
+
+
+/-
+/-
4
10876
B.cereus ATCC
+
-
-
+
-
-
+
-
-
5
3
B. cereus
+
-
-
-
-
-
+
-
-
6
1
B. cereus
+
-
-
+
-
-
+
-
-
7
2
B. cereus
+
-
-
+
-
-
+
-
-
8
66027
C. albicans ATCC
+
+
+
+
+
-
+
+
+
9
66027
C. albicans ATCC
+
-
-
+
-
-
+
-
-
10
892996
C. albicans
++
+
+
+
-
-
+
+
+
11
3814
C. albicans
+
+
+
-
-
+
+
+
+
51
12
8102
C. albicans
+
+
+
+
-
-
+
+
+
13
1801
C. albicans
+
+
+
+
+
+
+
+
+
14
2996
C. albicans
+
+
+
+
+
+
+
+
+
15
3305
C. albicans
+
+
+
+
+
+
+
+
+
16
3271
C. albicans
+
+
+
+
+
+
+
+
+
17
991374
C. lusitaniae
18
972711
C. krusei
19
973420
CNS
+
+
+
+
+
+
+
+
-
20
981534
E. agglomerans
+
+
+
+
++
++
+
+
+
21
977418
E. cloacae
+
+
+
+
++
+
+
+
+
22
989694
E. cloacae
+
+
+
+
+
+
+
+
+
23
984997
E. cloacae
+
+
+
+
+
+
+
+
+
24
980654
E. faecalis
+
+/-
+/-
+
+
+
+
+/-
+/-
25
864936
E. faecalis
+
+
+
+
+
+
+
+
+
26
893080
E. faecalis
++
+
+
+
+
+
+
+
+
27
29212
E. faecalis ATCC
+
+
+
+
+
+
+
+
+
28
893314
E. faecalis
+
+
+
+
+
+
+
+/-
+/-
29
895614
E. faecalis
+
+
+
+
+
+
+
+
+
30
896074
E. faecalis
+
+
+
+
+
+
+
+
+
31
987039
ESBL E. coli
+
+
+
+
+
+
+
+/-
+/-
32
980232
E. coli
+
+
+
+
++
+
+
+
+
33
973732
E. coli
+
+
+
+
++
++
+
+
+
34
979562
E. coli
+
+
+
+
++
++
+
+
+
35
893080
E. coli
+
+
+
+
+
+
+
+
+
36
891784
E. coli
+
+
+
+
+
+
+
+/-
+/-
37
891838
E. coli
+
++
++
+
+
+
+
+
+
38
892894
E. coli
+
++
++
+
+
+
+
+
+
39
890897
E. coli
+
+
+
+
+
+
+
+
+
40
35218
E. coli ATCC
+
+
+
+
+
+
+
+/-
+/-
41
980244
K. oxytoca
+
+/-
+
+
+
+
+
+/-
+/-
42
984997
K. oxytoca
+
+
+
+
+
+
+
+
+
43
983633
K. oxytoca
+
+
+
+
+
+
+
+/-
+/-
44
980659
K. pneumoniae
+
+
+
+
+
-
+
+
+
45
984400
K. pneumoniae
+
+
+
+
++
++
+
+
+
L.
46
978882
pseudomesenteroides
+
+
+
+
-
-
+
+
-
47
977070
MRSE
+
-
-
+
-
-
+
-
-
52
48
978024
MRSE
+
+
+
+
+
+
+
+
-
49
976687
MRSE
50
976802
MRSA
+
-
-
-
-
-
+
-
-
51
867949
MRSA
+
+
-
+
+
-
+
+
+
52
976672
MRSA
+
+
-
+
+
+
-
-
-
53
990866
P. stuartii
+
+
+
+
+
+
+
+
+
54
984374
P. aeruginosa
+
+
+
+
+
+
-
+
+
55
1825
P. aeruginosa
+
+
+
+
+
+
+
+
+
P. aeruginosa
56
27853
ATCC
+
+/-
+
+
+
+
+
+
+
57
891825
P. aeruginosa
+
+
+
+
+
+
+
+
+
58
892026
P. aeruginosa
+
+
+
+
+
+
+
+
+
59
864263
P. aeruginosa
+
+
+/-
+
+
+
+
+/-
+/-
60
867357
P. aeruginosa
+
+
+
+
+
+
+
+
+
61
8128
P. aeruginosa
+
+
+
+
++
++
+
+
+
62
977403
P. orizihabitans
63
973004
P. stutzeri
64
897
P. aeruginosa
65
974563
Salmonella species
+
+
+
+
+
+
+
+
+
66
979403
Salmonella siecies
+
+
+
+
+
+
+
+/-
+/-
67
985626
Salmonella species
+
+
+
+
+
+
+
+
+
68
980342
Salmonella species
+
+
+
+
+
+
+
+
69
867716
S. aureus
+
+
-
+
+
-
+
+
-
70
978523
S. aureus
+
+
+
+
+/-
+/-
+
-
-
71
980218
S. aureus
+
+
-
+
-
-
-
-
-
72
867181
S. aureus
+
+
-
+
+
-
+
+
+
73
891564
S. aureus
+
+
+
+
+/-
-
+
+/-
+/-
74
4330
S. aureus ATCC
+
-
-
+
-
-
+
+
-
75
868060
S. aureus
+
+
+
+
+
+
+
+
+
76
984375
S. haemolyticus
+
+
+
+
-
-
+
-
-
77
984253
S. hominis
+
-
-
+
-
+
+
-
-
78
984254
Streptococcus bovis
79
991504
Strep. Group b
+
+/-
+/-
+
-
-
+
-
-
Note: H.cuneifolia: Hermannia cuneifolia; W: Water; M: Methanol; A: Acetone; MRSA:
Methicilin-resistant S.aureus; MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase
Negative Staphylococci; (-): No growth (+/-): Slight inhibition (very weak activity); (+): Normal
53
growth (no activity); (++): Stimulated growth; Blank box: Organism did not grow on the control
plates.
Some strains of Staphylococcus and Bacillus have been successfully inhibited by methanol and
acetone extracts of H.cuneifolia. The growth of Pseudomonas species was observed to be
affected by the addition of DMSO. The colonies were slightly smaller and flat on the DMSO
control as compared to the plain growth control. Seven strains of Escherichia coli were
stimulated on exposure to the H.cuneifolia extracts.
Table 4.1: Summary of microorganisms inhibited by extracts of Hermannia cuneifolia
Bacteria
Bacillus cereus ATCC
Strain
Solvent (10mg/ml)
WATER
METHANOL
ACETONE
+
-
-
10876
Bacillus cereus
1
+
-
-
Bacillus cereus
2
+
-
-
Bacillus cereus
3
+
-
-
Candida albicans ATCC
66027
+
-
-
MRSE
1
+
-
-
MRSA
1
+
-
-
Staphylococcus aureus ATCC
4330
+
+
-
Staphylococcus aureus
1
+
+
-
Staphylococcus aureus
2
+
+
-
Staphylococcus hominis
1
+
-
+
Note: (-): Inhibited; (+): Not inhibited; MRSA: Methicilin-resistant S.aureus;
MRSE: Methicillin-resistant S.epidermidis
Table 4.1 is a summary of all consistent results as shown by the activity of H.cuneifolia extracts
in the respective solvents. Four strains of Bacillus cereus, three Staphylococcus species, three
strains of Staphylococcus aureus and one strain of Candida albicans are microorganisms that
were inhibited by the extracts of H.cuneifolia at 10mg/ml concentration.
54
Table 4.2: Antimicrobial results of Pentzia incana extracts
P.incana 1st run
P.incana 2nd run
P.incana 3rd run
{10mg/ml}
{10mg/ml}
{10mg/ml}
Strain
Bacteria Name
W
M
A
W
M
A
W
M
A
1
973723
A. baumannii
+
++
++
+
++
++
+
++
++
2
984736
A. haemolyticus
+
+
+
+
+
+
+
+
+
3
987221
A. lwoffi
+
++
+
+
+
+
+
+
+
4
10876
B. cereus ATCC
+
-
-
+
+/-
+/-
+
+/-
+/-
5
3
B. cereus
+
-
-
+
+/-
+/-
6
1
B. cereus
+
+
-
+
-
+/-
+
+/-
+/-
7
2
B. cereus
+
+
+
+
+/-
+/-
+
+/-
+/-
8
66027
C. albicans ATCC
+
+
+
+
-
-
+
+
+
9
66027
C. albicans ATCC
+
+
+
+
+
+
+
+
+
10
892996
C. albicans
+
+
+
+
-
+
+
+
+
11
3814
C. albicans
+
+
+
+
+
+
12
8102
C. albicans
+
+
+
+
-
-
+
+
+
13
1801
C. albicans
+
+
+
+
+
+
+
+
+
14
2996
C. albicans
+
+
+
+
+
+
+
+
+
15
3305
C. albicans
+
+
+
+
+
+
+
+
+
16
3271
C. albicans
+
+
+
+
+
+
+
+
+
17
991374
C. lusitaniae
18
972711
C. krusei
19
973420
CNS
+
++
++
+
++
++
+
++
++
20
981534
E. agglomerans
+
+
+
+
+
+/-
+
+/-
+
21
977418
E. cloacae
+
++
++
+
++
++
+
++
++
22
989694
E. cloacae
+
++
++
+
++
++
+
++
++
23
984997
E. cloacae
+
++
++
+
+
+
+
+
+
24
980654
E. faecalis
+
+
+
+
+
+
+
+
+
25
864936
E. faecalis
+
+
+
+
+
+
+
+
+
26
893080
E. faecalis
+
+
+
+
+
+
+
+
+
27
29212
E. faecalis ATCC
+
+
+
+
+
+
+
+
+
28
893314
E. faecalis
+
+
+
+
+
+
+
+
+
29
895614
E. faecalis
+
+
+
+
+/-
+/-
+
+/-
+/-
30
896074
E. faecalis
+
+
+
+
+/-
+/-
+
+/-
+/-
31
987039
ESBL E.coli
+
++
++
+
++
++
+
++
++
32
980232
E. coli
+
++
++
+
+
+
+
+
+
33
973732
E. coli
+
++
++
+
+
+
+
+
+
Number
55
34
979562
E. coli
+
++
++
+
+
+
+
+
+
35
893080
E. coli
+
++
++
+
++
++
+
++
++
36
891784
E. coli
+
++
++
+
++
++
+
++
++
37
891838
E. coli
+
++
++
+
++
++
+
++
++
38
892894
E. coli
+
+
+
+
+
+
+
+
+
39
890897
E. coli
+
++
++
+
+
+
+
+
+
40
35218
E. coli ATCC
+
++
++
+
++
++
+
++
++
41
980244
K. oxytoca
+
++
++
+
++
++
+
++
++
42
984997
K. oxytoca
+
++
++
+
++
++
+
++
++
43
983633
K. oxytoca
+
+
+
+
+
+
+
+
+
44
980659
K. pneumoniae
+
++
++
+
+
+
+
+
+
45
984400
K. pneumoniae
+
++
++
+
++
++
+
++
++
L.
46
978882
pseudomesenteroides
+
+
+
+
-
+
+
+
+
47
977070
MRSE
+
+
+
+
+
+
+
+
+
48
978024
MRSE
+
+
+
+
+
+
+
+
+
49
976687
MRSE
50
867949
MRSA
+
+
+
+
-
+/-
+
+/-
+/-
51
976672
MRSA
+
+
+
+
+/-
+/-
+
+
+
52
976802
MRSA
+
+
+
+
-
-
+
+
+
53
990866
P. stuartii
+
++
++
+
+
+
+
++
++
54
984374
P. aeruginosa
+
+
+
+
+
+
+
+
+
55
1825
P. aeruginosa
+
+
+
+
+
+
+
+
+
P. aeruginosa
56
27853
ATCC
+
+
+
+
+/-
+/-
+
+
+
57
891825
P. aeruginosa
+
+
+
+
+
+
+
+
+
58
892026
P. aeruginosa
+
+
+
+
+
+
+
+
+
59
864263
P. aeruginosa
+
+
+
+
+
+
+
+
+
60
867357
P. aeruginosa
+
+
+
+
+
+
+
+
+
61
8128
P. aeruginosa
+
+
+
+
+
+
+
+
+
62
977403
P. orizihabitans
63
973004
P. stutzeri
64
897
P. aeruginosa
65
974563
Salmonella species
+
++
++
+
++
++
+
++
++
66
979403
Salmonella species
+
++
++
+
++
++
+
++
++
67
985626
Salmonella species
+
++
++
+
+
+
+
+
+
68
980342
Salmonella species
+
+
+
+
+/-
+/-
56
69
867716
S. aureus
+
+
+
+
-
+/-
+
+
+
70
978523
S. aureus
+
+
+
+
+
+
+
+/-
+/-
71
980218
S. aureus
+
-
+
+
+
+
+
+/-
+/-
72
867181
S. aureus
+
+
+
+
-
+/-
+
+/-
+/-
73
891564
S. aureus
+
+
+
+
+
+
+
+
+/-
74
4330
S. aureus ATCC
+
+
+
+
+
+
+
+
+
75
868060
S. aureus
+
+
+
+
++
++
+
+
+
76
984375
S. haemolyticus
+
+
+
+
-
+
+
+
+
77
984253
S. hominis
+
-
+
+
-
+
+
+
+
78
984254
Streptococcus bovis
79
991504
Strep. group b
+
+
+
+
-
+
+
+
+
Note: P.incana: Pentzia incana; W: Water; M: Methanol; A: Acetone; MRSA: Methicilinresistant S.aureus; MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase Negative
Staphylococci; (-): No growth (+/-): Slight inhibition (very weak activity); (+): Normal growth
(no activity); (++): Stimulated growth; Blank box: Organism did not grow on the control plates.
Four strains of Bacillus cereus, one strain of Enterobacter agglomerans, two strains of
Enterococcus faecalis, two strains of Methicillin Resistant Staphylococcus aureus and five
strains of Staphylococcus aureus species showed slight inhibition by extracts of P.incana at
10mg/ml concentration. The two strains of Klebsiella pneumoniae and nine strains of
Escherichia coli were stimulated by extracts of P.incana.
Table 4.3: Antimicrobial results of Rhigozum obovatum extracts
Number
Strain
R.obovatum 1st run
R.obovatum 2nd run
R.obovatum 3rd run
{10mg/ml}
{10mg/ml}
{10mg/ml}
Bacteria Name
W
M
A
W
M
A
W
M
A
1
973723
A. baumannii
+
-
+
+
-
+
+
+
+
2
984736
A. haemolyticus
+
-
-
+
-
+
+
+
+
3
987221
A. lwoffi
+
-
+
+
-
+
+
+
+
4
10876
B. cereus ATCC
++
++
++
+
++
++
+
++
++
5
3
B. cereus
++
++
++
+
++
++
+
++
++
6
1
B. cereus
++
++
++
+
++
++
+
++
++
7
2
B. cereus
++
++
++
+
++
++
+
++
++
8
66027
C. albicans ATCC
+
+
+
+
+
+
+
+
+
9
66027
C. albicans ATCC
+
+
-
+
-
+
+
+
+
57
10
2996
C. albicans
+
+
+
+
+
+
+
+
+
11
3814
C. albicans
+
+
+
-
-
+
+
+
+
12
8102
C. albicans
+
+
+
+
+
+
+
+
+
13
1801
C. albicans
+
+
+
+
+
+
+
+
+
14
892996
C. albicans
+
+
+
+
+
+
+
+
+
15
3305
C. albicans
+
+
+
+
+
+
+
+
+
16
3271
C. albicans
+
+
+
+
+
+
+
+
+
17
991374
C. lusitaniae
18
972711
C. krusei
19
973420
CNS
+
-
+
+
-
+
+
+
+
20
981534
E. agglomerans
+
+
+
+
+
+
+
+
+
21
977418
E. cloacae
+
+
+
+
+
+
+
+
+
22
989694
E. cloacae
+
+
+
+
+
+
+
+
+
23
984997
E. cloacae
+
+
+
+
+
+
+
+
-
24
980654
E. faecalis
+
+
+
+
-
+
+
+
+
25
864936
E. faecalis
+
+
+
+
+
+
+
+
+
26
893080
E. faecalis
+
+
+
+
+
+
+
+
+
27
29212
E. faecalis ATCC
+
+
+
+
+
+
+
+
+
28
893314
E. faecalis
+
+
+
+
+
+
++
+
+
29
895614
E. faecalis
+
++
++
+
+
++
+
+
+
30
896074
E. faecalis
+
+
+
+
+
+
+
+
+
31
987039
ESBL E. coli
+
+
+
+
+
+
+
+
+
32
980232
E. coli
+
+
+
+
-
+
+
+
+
33
973732
E. coli
+
+
+
+
+
+
+
+
+
34
979562
E. coli
+
+
+
+
+
+
+
+
+
35
893080
E. coli
+
++
+
+
+
+
++
+
+
36
891784
E. coli
++
++
++
+
+
++
++
+
++
37
891838
E. coli
++
++
++
+
+
++
++
+
++
38
892894
E. coli
++
++
++
+
+
+
+
+
+
39
890897
E. coli
++
++
+
+
+
+
+
+
+
40
35218
E. coli ATCC
+
++
+
+
+
+
++
+
+
41
980244
K. oxytoca
+
+
+
+
-
+
+
+
+
42
984997
K. oxytoca
+
+
+
+
-
+
+
+
+
43
983633
K. oxytoca
+
+
+
+
++
+
+
+
+
44
980659
K. pneumoniae
+
+
+
+
-
-
+
+
+
45
984400
K. pneumoniae
+
+
+
+
-
+
+
+
+
46
978882
L.
+
-
+
-
-
-
+
+
+
58
pseudomesenteroides
47
977070
MRSE
+
-
+
-
-
-
+
+
+
48
978024
MRSE
+
-
+
+
-
-
+
+
+
49
976687
MRSE
50
867949
MRSA
+
-
-
+
-
-
+
+
+
51
976672
MRSA
+
-
+
+
-
-
+
+
+
52
976802
MRSA
+
-
+
-
-
-
+
+
+
53
990866
P. stuartii
+
-
+
+
-
-
+
+
+
54
984374
P. aeruginosa
+
+
+
+
+
+
+
+
+
55
1825
P. aeruginosa
+
+
+
+
++
+
+
+
+
P. aeruginosa
56
27853
ATCC
+
+
+
+
+
+
+
+
+
57
891825
P. aeruginosa
+
+
+
+
+
+
+
+
+
58
892026
P. aeruginosa
+
+
+
+
+
++
++
+
+
59
864263
P. aeruginosa
+
+
+
+
+
++
++
+
+
60
867357
P. aeruginosa
+
+
+
+
+
++
++
+
+
61
8128
P. aeruginosa
+
+
+
+
+
++
++
+
+
62
977403
P. orizihabitans
63
973004
P. stutzeri
64
897
P. aeruginosa
65
974563
Salmonella species
+
+
+
+
++
++
+
++
++
66
979403
Salmonella species
+
+
+
+
++
++
+
++
++
67
985626
Salmonella species
+
+
+
+
++
+
+
+
+
68
980342
Salmonella species
+
+
+
+
++
+
+
+
+
69
867716
S. aureus
+
-
+
+
-
-
+
-
+
70
978523
S. aureus
+
-
+
+
-
-
+
+
+
71
980218
S. aureus
-
-
-
+
-
-
+
+
+
72
867181
S. aureus
+
-
+
+
-
-
+
+
+
73
891564
S. aureus
+
-
+
+
-
-
+
+
+
74
4330
S. aureus ATCC
+
-
+
+
-
-
+
+
+
75
868060
S. aureus
+
-
+
+
-
-
+
+
+
76
984375
S. haemolyticus
+
-
+
+
-
-
+
+
+
77
984253
S. hominis
-
-
-
-
-
-
+
+
+
78
984254
Streptococcus bovis
79
991504
Strep. group b
+
-
+
+
-
+
+
+
+
Note: R.obovatum: Rhigozum obovatum; W: Water; M: Methanol; A: Acetone; MRSA:
Methicilin-resistant S.aureus; MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase
59
Negative Staphylococci. (-): No growth (+/-): Slight inhibition (very weak activity); (+): Normal
growth (no activity); (++): Stimulated growth; Blank box: Organism did not grow on the control
plates.
While the strains of B.cereus in the study were inhibited by extracts of H.cuneifolia, they were
also stimulated and grew into extra large colonies on exposure to the extracts of Rhigozum
obovatum at 10mg/ml concentration. Six strains of Escherichia coli and two strains of
Salmonella species were stimulated by extracts of R.obovatum.
Table 4.4: Antimicrobial results of Felicia muricata extracts
Number
Strain
F.muricata 1st run
F.muricata 2nd run
F.muricata 3rd run
{10mg/dl}
{10mg/dl}
{10mg/dl}
Bacteria Name
W
M
A
W
M
A
W
M
A
1
973723
A. baumannii
+
++
++
+
+
+
+
+
+
2
984736
A. haemolyticus
+
+
+
+
+
+
+
+
+
3
987221
A. lwoffi
+
++
+
+
+
+
+
+
+
4
10876
B. cereus ATCC
+
++
+
+
+
+
+
++
+
5
3
B. cereus
+
++
+
+
++
+
6
1
B. cereus
+
++
+
+
+
+
+
++
+
7
2
B. cereus
+
++
+
+
+
+
+
++
+
8
66027
C. albicans ATCC
+
+
+
+
+
+
+
+
+
9
66027
C. albicans ATCC
+
+
+
++
+
+
+
+
+
10
2996
C. albicans
+
+
+
+
+
+
+
+
+
11
3814
C. albicans
+
+
+
+
+
+
+
12
8102
C. albicans
+
+
+
+
+
+
+
+
+
13
1801
C. albicans
+
+
+
+
+
+
+
+
+
14
892996
C. albicans
+
+
+
+
+
+
+
+
+
15
3305
C. albicans
+
+
+
+
+
+
+
+
+
16
3271
C. albicans
+
+
+
+
+
+
+
+
+
17
991374
C. lusitaniae
18
972711
C. krusei
19
973420
CNS
+
++
++
+
+
+
+
+
+
20
981534
E. agglomerans
+
++
+
+
+
++
+
++
+
21
977418
E. cloacae
+
++
++
+
+
+
+
+
+
22
989694
E. cloacae
+
++
++
+
+
+
+
+
+
60
23
984997
E. cloacae
+
++
+
+
+
+
+
+
+
24
980654
E. faecalis
+
+
+
+
+
+
+
+
+
25
864936
E. faecalis
+
+
+
+
+
+
+
+
+
26
893080
E. faecalis
+
+
+
+
+
+
+
+
+
27
29212
E. faecalis ATCC
+
+
+
+
+
+
+
+
+
28
893314
E. faecalis
+
+
+
+
+
+
+
+
+
29
895614
E. faecalis
+
+
+
+
+
+
+
+
+
30
896074
E. faecalis
+
+
+
+
+
+
+
+
+
31
987039
ESBL E.coli
+
++
+
+
+
+
+
+
+
32
980232
E. coli
+
++
++
+
+
+
+
+
+
33
973732
E. coli
+
++
++
+
+
+
+
+
+
34
979562
E. coli
+
++
++
+
+
+
+
+
+
35
893080
E. coli
+
++
+
+
++
+
+
++
+
36
891784
E. coli
+
++
++
+
++
+
+
++
+
37
891838
E. coli
+
++
++
+
++
+
+
++
+
38
892894
E. coli
+
++
++
+
+
+
+
+
+
39
890897
E. coli
+
++
++
+
++
+
+
++
+
40
35218
E. coli ATCC
+
++
++
+
++
+
+
++
+
41
980244
K. oxytoca
+
++
++
+
+
+
+
+
+
42
984997
K. oxytoca
+
++
++
+
+
+
+
+
+
43
983633
K. oxytoca
+
+
+
+
+
+
+
+
+
44
980659
K. pneumoniae
+
++
++
+
+
+
+
+
+
45
984400
K. pneumoniae
+
++
+
+
+
+
+
+
+
L.
46
978882
pseudomesenteroides
+
+
+
+
+
+
+
+
+
47
977070
MRSE
+
+
+
+
-
+
+
+
+
48
978024
MRSE
+
+
+
+
+
+
+
+
+
49
976687
MRSE
50
867949
MRSA
+
+
+
+
+
+
+
+
+
51
976672
MRSA
+
+
+
+
+
+
+
+
+
52
976802
MRSA
+
+
+
-
-
-
+
+
+
53
990866
P. stuartii
+
++
++
+
+
+
+
+
+
54
984374
P. aeruginosa
+
+
+
+
+
+
+
+
+
55
1825
P. aeruginosa
+
+
+
+
+
+
+
+
+
56
27853
P. aeruginosa ATCC
+
+
+
+
+
+
+
++
+
57
891825
P. aeruginosa
+
+
+
+
+
+
+
+
+
58
892026
P. aeruginosa
+
+
+
+
+
+
+
+
+
61
59
864263
P. aeruginosa
+
+
+
+
+
+
+
+
+
60
867357
P. aeruginosa
+
+
+
+
+
+
+
+
+
61
8128
P. aeruginosa
+
++
++
+
+
+
+
+
+
62
977403
P. orizihabitans
63
973004
P. stutzeri
64
897
P. aeruginosa
65
974563
Salmonella species
+
++
++
+
+
+
+
+
+
66
979403
Salmonella species
+
++
++
+
+
+
+
+
+
67
985626
Salmonella species
+
++
++
+
+
+
+
+
+
68
980342
Salmonella species
+
+
+
+
+
+
+
+
+
69
867716
S. aureus
+
+
+
+
+
+
+
+
+
70
978523
S. aureus
+
++
+
+
+
+
+
+
+
71
980218
S. aureus
+
+
+
+
+
+
+
+
+
72
867181
S. aureus
+
+
+
+
+
+
+
++
+
73
891564
S. aureus
+
+
+
+
+
+
+
++
+
74
4330
S. aureus ATCC
+
+
+
+
+
+
+
+
+
75
868060
S. aureus
+
+
+
+
+
+
+
+
+
76
984375
S. haemolyticus
+
+
+
+
+
+
+
+
+
77
984253
S. hominis
+
+
+
+
+
+
+
+
+
78
984254
Streptococcus bovis
79
991504
Strep. group b
+
+
+
+
+
+
+
+
+
Note: F.muricata: Felicia muricata; W: Water; M: Methanol; A: Acetone; MRSA: Methicilinresistant S.aureus; MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase Negative
Staphylococci; (-): No growth (+/-): Slight inhibition (very weak activity); (+): Normal growth
(no activity); (++): Stimulated growth; Blank box: Organism did not grow on the control plates.
The two strains of Klebsiella pneumoniae and ten strains of Escherichia coli were stimulated by
extracts of F.muricata. No antimicrobial activity has been observed by the extracts of
F.muricata. Out of the seventy-nine microorganisms tested against the four extracts of plants
H.cuneifolia, P.incana, R.obovatum and F.muricata, forty-eight microorganisms which were
inhibited in most of the runs were selected for further analysis using extracts of Harpephyllum
caffrum and Chironia baccifera. The investigation was conducted at 10mg/ml and 20mg/ml
concentration because during the preliminary testing the 10mg/ml concentration showed no
activity.
62
Table 4.5: Antimicrobial results of Harpephyllum caffrum extracts
Number
WATER
METHANOL
ACETONE
{10mg/ml}{20mg/ml} {10mg/ml} {20mg/ml} {10 mg/ml}{20 mg/ml}
Strain
Bacteria Name
1
973723
A. baumannii
-
-
-
-
-
-
2
984736
A. haemolyticus
-
-
-
-
-
-
3
987221
A. lwoffi
-
-
-
-
-
-
4
66027
C. albicans ATCC
-
-
-
-
-
-
5
66027
C. albicans ATCC
-
-
-
-
-
-
6
892996
C. albicans
-
-
-
-
-
-
7
3814
C. albicans
-
-
-
-
-
-
8
8102
C. albicans
-
-
-
-
-
-
9
1801
C. albicans
-
-
-
-
-
-
10
2996
C. albicans
-
-
-
-
-
-
11
3305
C. albicans
-
-
-
-
-
-
12
3271
C. albicans
-
-
-
-
-
-
13
991374
C. lusitaniae
-
-
-
-
-
-
14
972711
C. krusei
-
-
-
-
-
15
980654
E. faecalis
+
-
+
+
+
-
16
864936
E. faecalis
+
-
+
+
+
+
17
893080
E. faecalis
18
29212
E. faecalis ATCC
-
-
-
-
-
-
19
893314
E. faecalis
-
-
-
-
-
-
20
895614
E. faecalis
-
-
-
-
-
-
21
896074
E. faecalis
-
-
-
-
-
-
22
973732
E. coli
+
+
+
+
+
+
23
979562
E. coli
+
+
+
+
+
+
24
891784
E. coli
+
+
+
+
+
+
25
890897
E. coli
+
+
+
+
+
+
26
980244
K. oxytoca
+
+
+
+
+
+
27
984997
K. oxytoca
+
+
+
+
+
+
63
28
983633
K. oxytoca
+
+
+
+
+
+
29
984400
K. pneumoniae
+
+
+
+
+
+
30
L.
978882
pseudomesenteroides
31
976687
MRSE
32
990866
P. stuartii
+
+
+
+
+
+
33
984374
P. aeruginosa
+
+
+
+
+
+
34
1825
P. aeruginosa
+
+
+
+
+
+
35
27853
P. aeruginosa ATCC
+
+
+
+
+
+
36
891825
P. aeruginosa
+
+
+
+
+
+
37
892026
P. aeruginosa
+
+
+
+
+
+
38
864263
P. aeruginosa
+
+
+
+
+
+
39
867357
P. aeruginosa
40
8128
P. aeruginosa
+
+
+
+
+
+
41
977403
P. orizihabitans
42
973004
P. stutzeri
43
897
P. aeruginosa
+
+
+
+
+
+
44
979403
Salmonella species
+
+
+
+
+
+
45
985626
Salmonella species
+
+
+
+
+
+
46
868060
S. aureus
-
-
-
-
-
-
47
984254
Streptococcus bovis
48
991504
Strep. group b
Note: (+): growth; (-): Inhibition; (BLANK BOX): No growth on control plate;
MRSE: Methicillin-resistant S.epidermidis.
Three species of Acinetobacter, nine strains of Candida albicans, 2 other Candida species, four
strains of Enterococcus faecalis and one strain of Staphylococcus aureus were inhibited by
aqueous, methanol and acetone extracts of H.caffrum.
64
Table 4.6: Antimicrobial results of Chironia baccifera extracts
Number
WATER
METHANOL
ACETONE
{10mg/ml} {20mg/ml} {10mg/ml} {20mg/ml} {10 mg/ml}{20 mg/ml}
Strain
Bacteria Name
1
973723
A. baumannii
+
+
+
+
+
+
2
984736
A. haemolyticus
+
+
-
-
-
-
3
987221
A. lwoffi
+
+
+
+
+
+
4
66027
C. albicans ATCC
+
+
+
+
+
+
5
66027
C. albicans ATCC
+
+
+
+
+
+
6
892996
C. albicans
+
+
+
+
+
+
7
3814
C. albicans
+
+
+
+
+
+
8
8102
C. albicans
+
+
+
+
+
+
9
1801
C. albicans
+
+
+
+
+
+
10
2996
C. albicans
+
+
+
+
+
+
11
3305
C. albicans
+
+
+
+
+
+
12
3271
C. albicans
+
+
+
+
+
+
13
991374
C. lusitaniae
+
+
+
+
+
+
14
972711
C. krusei
+
+
+
+
+
+
15
980654
E. faecalis
+
+
-
-
-
16
864936
E. faecalis
+
+
-
-
-
-
17
893080
E. faecalis
18
29212
E. faecalis ATCC
+
+
-
-
-
-
19
893314
E. faecalis
+
+
-
-
-
-
20
895614
E. faecalis
+
+
-
-
-
-
21
896074
E. faecalis
+
+
-
-
-
-
22
973732
E. coli
+
+
+
+
+
+
23
979562
E. coli
+
+
+
+
+
+
24
891784
E. coli
+
+
+
+
+
+
25
890897
E. coli
+
+
+
+
+
+
26
980244
K. oxytoca
+
+
+
+
+
+
27
984997
K. oxytoca
+
+
+
+
+
+
65
28
983633
K. oxytoca
+
+
+
+
+
+
29
984400
K. pneumoniae
+
+
+
+
+
+
30
L.
978882
pseudomesenteroides
31
976687
MRSE
+
+
-
-
-
-
32
990866
P. stuartii
+
+
+
+
+
+
33
984374
P. aeruginosa
+
+
+
+
+
+
34
1825
P. aeruginosa
+
+
+
+
+
+
P. aeruginosa
+
+
+
+
+
35
+
27853
ATCC
36
891825
P. aeruginosa
+
+
+
+
+
+
37
892026
P. aeruginosa
+
+
+
+
+
+
38
864263
P. aeruginosa
+
+
+
+
+
+
39
867357
P. aeruginosa
40
8128
P. aeruginosa
+
+
+
+
+
+
41
977403
P. orizihabitans
42
973004
P. stutzeri
43
897
P. aeruginosa
+
+
+
+
+
+
44
979403
Salmonella species
+
+
+
+
+
+
45
985626
Salmonella species
+
+
+
+
+
+
46
868060
S. aureus
+
+
-
-
-
-
47
984254
Streptococcus bovis
48
991504
Strep. group b
Note: (+): growth; (-): Inhibition; (BLANK BOX): No growth on control plate
MRSE: Methicillin-resistant S. epidermidis.
One strain of Acinetobacter haemolyticus, six strains of Enterococcus faecalis, one strain of
Methicillin Resistant Staphylococcus epidermidis and one strain of Staphylococcus aureus were
inhibited by methanol and acetone extracts of Chironia baccifera.
Since the MIC method is more sensitive than the agar diffusion method, seven microbes which
were inhibited by extracts of H.caffrum, twelve microbes not inhibited by extracts of H.caffrum
66
and other twenty microbes from clinical isolates, totalling to thirty-nine microorganisms, were
tested further for MIC determination.
4.3 Minimum inhibitory concentration (MIC)
It was difficult to note other inhibition due to colour similarity; however, the
Figure 4.6: Microtitre plate showing colour intensity
colour intensity had enabled the possibility of differentiation when compared to growth controls.
Control wells with growth were much darker than the wells without growth.
Figure 4.7: Microtitre plate showing MIC values
As an organism develops resistance to the plant extract, the MIC will increase, and a greater
concentration will be needed to inhibit growth of the bacterial population. The following
section contains data table reflecting the MIC values of H.caffrum extracts. These values are
an average of the results obtained in triplicate runs.
67
Table 4.7: Mean MIC results of 39 selected microorganisms tested with extracts of H.caffrum
Number
Strain
Bacteria Name
Harpephyllum caffrum (mg/ml)
Water
Methanol
Acetone
1
1826
P. aeruginosa
+
+
+
2
8128
P. aeruginosa
+
+
+
3
893080
E. coli
0.391
0.049
0.049
4
891838
E. coli
0.391
0.049
0.049
5
892894
E. coli
0.391
0.049
0.195
6
4330
S. aureus
0.195
0.098
0.049
7
867949
MRSA
0.195
0.049
0.049
8
10876
B. cereus ATCC
0.195
0.049
3.125
9
3
B. cereus
0.391
0.195
0.195
10
1
B. cereus
0.391
0.781
0.195
11
2
B. cereus
0.391
0.195
0.195
12
867716
S. aureus
0.195
0.049
0.049
13
891564
S. aureus
0.195
0.049
0.049
14
867181
S. aureus
0.195
0.049
0.049
15
980244
K. oxytoca
0.391
0.049
0.049
16
984997
K. oxytoca
0.391
0.098
0.195
17
977070
MRSE
6.25
0.781
1.563
18
978024
MRSE
6.25
0.781
1.563
19
976672
MRSA
3.125
0.391
0.049
20
976802
MRSA
3.125
0.391
0.195
+
+
+
+
+
+
Salmonella
21
974563
species
Salmonella
22
980342
species
23
973723
A. baumannii
12.5
0.781
0.781
24
984736
A. haemolyticus
6.25
3.125
3.125
25
987221
A. lwoffi
6.25
1.563
1.563
26
35218
E. coli ATCC
0.391
0.049
0.049
27
984375
S. haemo lyticus
0.781
0.098
0.195
28
984253
S. hominis
0.391
0.781
0.195
29
980218
S. aureus
0.195
0.049
0.049
30
978523
S. aureus
0.195
0.049
0.049
31
987039
ESBL E. coli
0.391
0.049
0.049
32
977418
E. cloacae
+
+
+
68
33
989694
E. cloacae
+
+
34
984997
E. cloacae
+
+
+
35
981534
E. agglomerans
+
+
+
36
973420
CNS
0.195
0.098
0.098
37
980659
K. pneumoniae
0.39
0.049
0.195
38
990866
P. stuartii
+
+
+
39
980232
E. coli
0.391
0.049
0.049
Note: (+): No inhibition even at highest concentration; MRSA: Methicilin-resistant S.aureus;
MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase Negative Staphylococci.
Seventy six percent of the thirty-nine microorganisms selected showed MIC values. Strains of
Pseudomonas aeruginosa, Escherichia coli, Klebsiella and Salmonella species which were not
inhibited in the agar diffusion assay also showed MIC values ranging from 0.049 to 6.25mg/ml.
Table 4.8: Mean MIC results of 39 selected microorganisms tested with extracts of C.baccifera
Number
Strain
Bacteria Name
Chironia baccifera (mg/ml)
Water
Methanol
Acetone
1
1826
P. aeruginosa
+
+
+
2
8128
P. aeruginosa
+
+
+
3
893080
E. coli
+
+
+
4
891838
E. coli
+
+
+
5
892894
E. coli
+
+
+
6
4330
S. aureus
+
0.781
1.563
7
867949
MRSA
+
1.563
1.563
8
10876
B. cereus ATCC
+
+
+
9
3
B. cereus
+
+
+
10
1
B. cereus
+
+
+
11
2
B. cereus
+
+
+
12
867716
S. aureus
+
0.781
3.125
13
891564
S. aureus
+
0.391
1.563
14
867181
S. aureus
+
6.25
+
15
980244
K. oxytoca
+
+
+
16
984997
K. oxytoca
+
+
+
17
977070
MRSE
+
+
+
69
18
978024
MRSE
+
+
+
19
976672
MRSA
+
+
+
20
976802
MRSA
+
+
+
+
+
+
Salmonella
21
974563
species
Salmonella
22
980342
species
+
+
+
23
973723
A. baumannii
+
+
+
24
984736
A. haemolyticus
+
6.25
3.125
25
987221
A. lwoffi
+
+
+
26
35218
E. coli ATCC
+
+
+
27
984375
S. haemolyticus
+
3.125
1.563
28
984253
S. hominis
+
+
+
29
980218
S. aureus
+
0.781
+
30
978523
S. aureus
+
0.781
+
31
987039
ESBL E. coli
+
+
+
32
977418
E. cloacae
+
+
+
33
989694
E. cloacae
+
+
+
34
984997
E. cloacae
+
+
+
35
981534
E. agglomerans
+
+
+
36
973420
CNS
+
+
+
37
980659
K. pneumoniae
+
+
+
38
990866
P. sturtii
+
+
+
39
980232
E. coli
+
+
+
Note: (+): No inhibition even at highest concentration; MRSA: Methicilin-resistant S.aureus;
MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase Negative Staphylococci.
One nonfermentative Gram-negative bacilli, Acinetobacter haemolyticus and eight Grampositive microorganisms: six strains of Staphylococcus aureus, one strain of Staphylococcus
haemolyticus and one strain of Methicillin Resistant Staphylococcus aureus showed MIC values
ranging from 0.391 to 6.25mg/ml.
70
Table 4.9: Mean MIC results of 39 selected microorganisms tested with extracts of H.cuneifolia
Number
Strain
Bacteria Name
Hermannia cuneifolia (mg/ml)
Water
Methanol
Acetone
1
1826
P. aeruginosa
+
+
+
2
8128
P. aeruginosa
+
25
12.5
3
893080
E. coli
+
+
+
4
891838
E. coli
+
+
+
5
892894
E. coli
+
+
+
6
4330
S. aureus
+
0.19
0.19
7
867949
MRSA
+
0.19
0.09
8
10876
B. cereus ATCC
+
0.05
0.05
9
3
B. cereus
+
0.05
0.05
10
1
B. cereus
+
0.05
0.05
11
2
B. cereus
+
0.05
0.05
12
867716
S. aureus
+
0.09
0.09
13
891564
S. aureus
+
1.56
25
14
867181
S. aureus
+
3.125
+
15
980244
K. oxytoca
+
25
0.78
16
984997
K. oxytoca
+
25
+
17
977070
MRSE
+
+
25
18
978024
MRSE
+
3.125
12.5
19
976672
MRSA
+
1.56
12.5
20
976802
MRSA
+
+
6.25
+
+
6.25
Salmonella
21
974563
species
Salmonella
22
980342
species
+
+
6.25
23
973723
A. baumannii
+
+
+
24
984736
A. haemolyticus
+
25
12.5
25
987221
A. lwoffi
+
+
+
26
35218
E. coli ATCC
+
6.25
12.5
27
984375
S. haemolyticus
+
+
25
28
984253
S. hominis
+
12.5
12.5
29
980218
S. aureus
+
+
25
30
978523
S. aureus
+
+
25
31
987039
ESBL E. coli
+
+
12.5
32
977418
E. cloacae
+
+
+
71
33
989694
E. cloacae
+
+
12.5
34
984997
E. cloacae
+
+
+
35
981534
E. agglomerans
+
+
+
36
973420
CNS
+
+
+
37
980659
K. pneumoniae
+
+
+
38
990866
P. stuartii
+
+
+
39
980232
E. coli
+
+
+
Note: (+): No inhibition even at highest concentration; MRSA: Methicilin-resistant S.aureus;
MRSE: Methicillin-resistant S.epidermidis; CNS: Coagulase Negative Staphylococci.
All the Gram-positive microorganisms which were inhibited by H.cuneifolia in agar diffusion
method showed MIC values at concentrations ranging from 0.05 to 12.5mg/ml. Furthermore,
some Gram-negative bacteria like Pseudomonas aeruginosa, Klebsiella oxytoca, Salmonella,
Escherichia coli, Acinetobacter haemolyticus, and Enterobacter cloacae showed MIC values at
concentrations ranging from 0.78 and 25mg/dl. This agrees with the results of Thring et al.
(2007) where Candida albicans tested against extracts of Chironia baccifera indicated no
inhibition in all solvents used in the disc diffusion assay but showed MIC values of 1.25mg/ml
and 5mg/ml in methanol and ethyl-acetate extracts of Chironia baccifera, respectively. This
shows that the bioassay (MIC) is more sensitive than the disc or agar diffusion method as more
activity was recorded from the MIC bioassay.
4.4 Thin Layer Chromatography
The TLC fingerprints of different extracts were prepared by spotting 0.5 mg of methanol,
acetone and water extracts as a 1cm band onto a large TLC plate (silica gel 60 F 254 , 0.25 mm,
20cm×20cm, Merck).
72
Figure 4.8: Plant extracts spotted on TLC silica plates
The plates were developed in petroleum ether: ethyl acetate: chloroform: formic acid (8:7:5:1),
over a distance of 17 cm.
Figure 4.9: TLC silica plates spotted with extracts developing in air tight glass jar
Once the extracts were separated by TLC and the solvent evaporated, the separated components
were visualised under visible and ultraviolet light UV 300 (Gibbons and Gray, 1998).
73
1
2
3
Figure 4.10: Developed TLC silica plates after evaporating and drying
The bioautographic assay showed a number of clear white spots against a grey background. The
white spots (inhibition zones) give an indication of antimicrobial activity by compounds present
in these areas. Inhibition zones were visible in methanol and acetone extracts of Harpephyllum
caffrum tested areas.
F1
F2
F3
74
F4
F5
F6
Figure 4.11: F1 to F6 are TLC silica plates after the bioautographic assay viewed under UV light
Plate F1: Staphylococcus aureus growth inhibition visible as white spots.
Plate F2: Enterococcus faecalis growth inhibition visible as white spots.
Plate F3: Candida albicans growth inhibition visible as white spots.
Plate F4: Comparison of F3 and F1
Plate F5: Comparison of F3, F1 and F2
Plate F6: Comparison of F1 and F2. From left to right (F1 towards F2), the extracts added on the
spots are: water, methanol and acetone extracts of Harpephyllum caffrum; water, methanol and
acetone extracts of Hermannia cuneifolia. Water extracts of H.caffrum did not show any
inhibition zones. By separating bioactive extracts on the TLC, it is possible to get information on
the compounds present in the plant extract.
In figure 4.11 above, F1 shows four zones of inhibition indicated by the white spots (see arrows)
and representing four different compounds that have been separated from methanol and acetone
extracts of Harpephyllum caffrum. F2 shows five zones of inhibition representing five
compounds that have inhibited Enterococcus faecalis from methanol and acetone extracts of
Harpephyllum caffrum. F3 showed one zone of inhibition but after 10 minutes, another zone
appeared below it as indicated in F4, signifying that there might be other active compounds in
Harpephylum caffrum extracts that can inhibit Candida albicans.
Below is Table 4.11 indicating the R f values of E.faecalis, S.aureus and C.albicans calculated
after visualization of inhibition zones under visible and UV light.
75
Table 4.10: R f values of major zones present in chromatograms of methanol and acetone Harpephyllum
caffrum extracts.
BAND 1
MICROORGANISM
BAND 2
BAND 3
BAND 4
BAND 5
M
A
M
A
M
A
M
A
M
A
E.faecalis
0.28
0.28
0.31
0.31
0.45
0.45
0.66
0.66
0.90
0.90
S.aureus
0.25
0.25
0.30
0.30
0.44
0.44
0.95
0.95
C. albicans
0.25
0.28
0.32
0.34
0.48
0.48
Note: M: Methanol; A: Acetone.
E.faecalis showed five zones of inhibition on TLC plates having the same R f values in methanol
and acetone extracts ranging from 0.28 to 0.90. S.aureus showed four zones of same R f values in
methanol and acetone extracts ranging from 0.25 to 0.95. C.albicans showed three zones, of
which the first and second zones from the bottom had different R f values in their respective
extract solvent. The third zone had same R f value in methanol and acetone extracts. The R f
values of C.albicans ranged from 0.25 to 0.48. The different inhibiton zones show differences in
the chemical composition of plant extracts (figure 4.11). Methanol and acetone extracts of
Hermannia cuneifolia showed a continuous brown and white band appearing faint in other areas.
4.4 The Ames test
The mutagenicity results shown in Table 4.12 below revealed that all the extracts were nonmutagenic towards Salmonella typhimurium strain TA100. A compound is considered a mutagen
if the results show a dose dependent increase in the number of revertants and if the number of
revertants is equal to or greater than two times of the negative control (Bulmer et al., 2007).
Table 4.11: Number of histidine+ revertants in Salmonella typhimurium strain TA100
Plant
Harpephyllum caffrum
Hermannia cuneifolia
Extract
Concentration vs Number of Colonies per plate
600µg/ml
200μg/ml
Methanol
8±3
10 ± 2
Acetone
12 ± 3
12 ± 3
Water
7±2
9±2
Methanol
24 ± 4
22 ± 4
Acetone
23 ± 5
27 ± 4
Water
10 ± 3
10 ± 4
4-nitroquinoline-N-oxide (positive control), 10μg/ml
235 ± 8 colonies
Water (negative control)
25 ± 5 colonies
76
According to the criteria defined in this study, extracts of Harpephyllum caffrum and Hermannia
cuneifolia could be classified as having antimutagenic properties. The extracts of the plants
presented similar results for the absence of mutagenic induction despite the different solvents
used and in the absence of metabolic activation. The average His+ revertants observed ranged
between 7 and 27 for all the extracts at concentrations (200µg/ml and 600μg/ml) of histidine
while 25 revertant colonies grew on the negative control and 235 revertant colonies on the
positive control, 4-nitroquinoline-N-oxide (4-NQO). Therefore, none of the extracts under study
could be regarded as mutagenic.
77
CHAPTER 5: DISCUSSION AND CONCLUSION
The fields of ethnopharmacology, ethnobotany and natural products chemistry, is progressing
steadily in South Africa. Ethnopharmacologists, botanists, microbiologists, and natural-product
chemists are searching the earth for phytochemicals which could be developed for the treatment
of infectious diseases (Tanaka et al., 2006) especially in light of the emergence of drug-resistant
microorganisms and the need to produce more effective antimicrobial agents.
It has been shown that in vitro screening methods could provide the needed preliminary
observations necessary to select crude plant extracts with potentially useful properties for further
chemical and pharmacological investigations (Mathekaga and Meyer, 1998).
This study investigated the antimicrobial activities of Harpephyllum caffrum, Hermannia
cuneifolia, Chironia baccifera, Rhigozum obovatum, Felicia muricata and Pentzia incana. The
plants were tested against six ATCC strains and seventy-three microorganisms isolated from
patients suffering from septicaemia. Three methods were used to determine the antimicrobial
activity of the plants. The methods included the agar diffusion method, microtitre plate method
to determine MIC, TLC fingerprints with the corresponding bioautographic assays and the Ames
test for possible carcinogenicity. Different extracts of the plants were made and it was found that
the water extracts did not perform well in this study. Literature supports this finding as reported
by Meyer and Afolayan (1995) as well as Masika and Afolayan (2002), stating that the choice of
acetone and methanol as solvents for extraction and the exclusion of water extracts in their
analysis was based on their previous observation and other reports that water extracts of plants
generally showed little or no antimicrobial activities. Cragg et al. (1994) also reported great
differences between the activity of aqueous and organic extracts in their anti-HIV screening. It
was however still valuable to test water extracts of these plants as traditionally, plant extracts are
prepared with water as used in infusions, decoctions and poultices. Thring et al. (2007) is of the
opinion that it seems unlikely that the traditional healer will be able to extract those compounds
which are responsible for activity in the acetone and methanol extracts by using traditional
methods. Observations of very weak (+/-) or no activity (+) of aqueous plant extracts on Gramnegative bacteria are well documented (Eloff, 1998b; Madamombe and Afolayan, 2003;
Afolayan, 2003).
78
In this study, the agar diffusion method showed that the methanol extracts of the plants inhibited
a higher percentage of microorganisms when compared to the acetone extracts. Similar
observations were reported by Grierson and Afolayan (1999) on water, methanol and acetone
extracts from some indigenous plants used for the treatment of wounds in the Eastern Cape,
South Africa. They found that the majority of the antibacterial activity observed was in the
methanol extracts. Methanol extracts of Hermannia cuneifolia inhibited 16%, acetone extracts
inhibited 22% and aqueous extracts inhibited 2% of the microorganisms tested. Slight inhibition
was observed with 8% of the methanol extracts, 7% of the acetone extracts and 2% of aqueous
extracts. Pentzia incana showed no antimicrobial activity in aqueous extracts. The methanol
extracts inhibited 7% of microorganisms while acetone extracts inhibited 2%. Slight inhibition
was observed in 8% of the microbes tested in methanol extracts and 10% in acetone extracts. The
methanol extracts of Rhigozum obovatum inhibited 21% of the tested microorganisms, acetone
extracts inhibited 10%, and aqueous extracts inhibited 3% of the bacteria.
Among all microorganisms that grew, 11% were stimulated (had larger colonies than the control
plate) by extracts of Felicia muricata and Rhigozum obovatum. Pentzia incana stimulated 16%
and Hermannia cuneifolia stimulated 2% of the bacteria. However, stimulation of microbial
growth may facilitate illness in patients treated by such herbal medicine as observed in the plants
extracts, while inhibition may suppress the growth and multiplication of the organism hence
curing the disease. Hayes (1947) reported in a study entitled “Survey of higher plants for
presence of antibacterial substances”, that some plant extracts caused increased bacterial growth.
Another observation in the agar diffusion assay was that none of the Gram-negative bacteria
were inhibited by the plants extracts tested. Gram-negative bacteria have an outer phospholipidic
membrane with structural lipopolysaccharide components. This composition makes the cell wall
impermeable to lipophilic solutes, and the porins in the cell wall form a selective barrier to
hydrophilic solutes, with an exclusion limit of about 600 Da (Nikaido and Vaara, 1985; Yao and
Moellering, 1995). Four strains of Bacillus cereus, one strain of Candida albicans, and two
strains of Staphylococcus aureus were inhibited by methanol and acetone extracts of Hermannia
cuneifolia. This may be attributed to the fact that cell wall in Gram-positive bacteria consists of a
single outer peptidoglycan layer which is not an effective permeability barrier (Scherrer and
Gerhardt, 1971).
79
Some medicinal plants are named locally after their effects upon consumption by humans. For
example, the local name for Hermannia cuneifolia is kwaaiman (Van Wyk and Els, 2008) and it
means ‘angry man’ because the infusion that is prepared from a leafy twig burns the throat when
used to treat sore throat. Klebsiella pneumoniae is a respiratory pathogen commonly associated
with colds and flu (Viljoen et al., 2004). The inhibitory property of extracts from H.cuneifolia on
pathogens of respiratory tract might have been the reason for using this plant in the treatment of
sore throat and coughs.
The inhibition of strains of Candida albicans by extracts of Harpephyllum caffrum as indicated
in Table 4.6 may support the use of this plant as a traditional medicine for treating acne and
eczema or as a blood purifier as manifested by pimples on the face. The findings can support the
use of this plant in treating fungal skin infections.
Hence, the antibacterial activity of Hermannia cuneifolia and Harpephyllum caffrum extracts on
these different clinical isolates of bacteria causing septicaemia strengthen scientific evidence of
the effectiveness of medicinal plants in the treatment of various ailments by traditional healers.
The ability of the plants extracts to inhibit the growth of several bacteria and fungi species is an
indication of the antimicrobial potential which makes these plants likely candidates for
bioprospecting for antibiotic drugs.
In this study, when comparing the agar diffusion method to microtitre plate dilution method used
for MIC determination, a discrepancy was found with the activity of methanol extracts as
compared to acetone extracts. Methanol extracts showed more activity in the agar diffusion
method (see Table 4.1 - 4.7) while acetone extracts showed more activity in the microtitre plate
dilution method. For example, the MIC results of extracts from Hermannia cuneifolia showed
one Staphylococcus aureus and one Klebsiella oxytoca inhibited with values of 3.125 and 25.0
mg/ml, respectively, which were not inhibited in acetone extracts. While one strain of MRSE,
one strain of MRSA, two strains of Salmonella species, two strains of Staphylococcus aureus,
one strain of Staphylococcus haemolyticus, one strain of E.coli and one strain of Enterobacter
cloacae were inhibited at values 25.0, 6.25, 6.25, 25.0, 25.0, 12.5 and 12.5mg/ml respectively,
by acetone extracts only (Table 4.10). In contrast, in a study entitled “antimicrobial activity of
extracts from Felicia muricata”, Ashafa et al. (2008) reported that methanol extracts were more
active than acetone and aqueous extracts using the agar dilution method and the microtitre plate
method. This discrepancy may be associated with the presence or absence of soluble phenolic
80
and polyphenolic compounds (Kowalski and Kedzia, 2007). However, it is difficult to compare
results obtained, against the published results in literature especially when dealing with plant
extracts. The reason is that, several variables influence the results, such as the environmental and
climatic conditions under which the plant grew, choice of plant extracts, choice of extraction
method, antimicrobial test method and test microorganisms (Nostro et al., 2000; Hammer et al.,
1999). Furthermore, Rios and Villar (1988) narrated that the variation, which is often observed in
testing crude plant extracts for antibacterial activity can be attributed to a variety of factors.
These include the assay technique, culture medium, strain of bacteria used for testing, age of the
agar plate, plant source and whether it is used fresh or dried, and the quality of extract tested. In
addition, there is no standardized method for expressing the results of antibacterial testing.
In this study, the comparison of methodologies has shown that agar diffusion and MIC methods
used to measure antimicrobial activity do not give parallel results, confusing any assessment of
antimicrobial activity. Similar results were reported by Njenga et al. (2005) and Youssef and
Tawill (1990) who showed that comparison of methodologies has shown that agar diffusion and
serial dilution methods to measure antimicrobial activity do not always give parallel results.
The inclusion of TLC fingerprints in modern pharmaceutical herbal monographs is now standard
practice (Scott et al., 2004). The results obtained in this study demonstrate the utility of TLC to
distinguish with certainty the antimicrobial activity of these herbal plants. Bioautography
combines TLC with a bioassay in situ and, therefore allows the researcher to localize the active
compounds within a sample (Hamburger and Cordell, 1987; Gibbons and Gray, 1998).
Harpephylum caffrum showed the best separation by the solvent system, petroleum ether: ethyl
acetate: chloroform: formic acid (8:7:5:1), which was used. Other researchers have used solvent
systems like 1.75M acetic acid: ethyl-acetate: toluene (1:1:1) (Thring et al., 2007); hexane: ethyl
acetate (3:1) (Yffa et al., 2002), selected empirically using prior personal experience and
literature reports of similar separations as a guide in the mobile phase.
Variation in zone size, zone numbers and colour intensity between the solvent solutions and
plant species examined indicate that some quantitative infraspecific variation was present (Scott
et al., 2004). Compounds that are naturally coloured, such as chloroplast and bile pigments
(Eidam et al., 2001), are viewed directly in daylight or white light with the naked eye.
Compounds with native fluorescence are viewed as bright, coloured zones on a dark background
81
under 366nm or 254nm ultraviolet (UV) light on layers without fluorescent indicator.
Compounds that absorb 254nm UV light, particularly those with aromatic rings and conjugated
double bonds, can be detected on an “F-layer” containing a fluorescent indicator or phosphor.
When irradiated with 254nm UV light, absorbing compounds diminish (quench) the uniform
layer fluorescence and can be viewed as dark violet spots on a green or pale-blue background
(Sherma and Fried, 2005). Hence, the compounds observed in the study were possibly
chloroplasts since the zones were viewed directly in daylight with the naked eye as well as under
300nm UV light.
The Ames test was used because it is reliable, quick and easy. The absence of mutagenic
response suggests that Harpephyllum caffrum and Hermannia cuneifolia plant extracts upon
exposure to Salmonella typhimurium bacterial strain in the Ames assay are probably safe for use
in traditional medicine or is the first step forward in determining the safe use of these plants,
though further safety testing may be appropriate. In support of these findings, the Ames test
conducted by Elgorashi et al. (2003) on the extracts from the leaves of Harpephyllum caffrum
showed negative results in 90% of methanol extracts tested by Salmonella typhimurium strain
TA98 and TA100 with and without S9. Hence, the results reported here might be considered
sufficient for further studies aimed at isolating and identifying the active compounds.
The determination of toxicity of South African plants is particularly necessary as the use of some
traditional medicines has resulted in several cases of acute toxicity, leading to increased
morbidity and mortality (Reid et al., 2006). Popat et al. (2001) refers to three case studies in
South Africa indicating a high rate of acute toxicity resulting from the use of traditional
medicines. Screening is required to identify and eradicate the use of all mutagenic plants as
numerous studies have shown that the proportion of carcinogens identified as mutagens by the
Ames test ranges from about 50% to 90% (Zeiger, 2001). The occurrence rate of cancer is
increasing worldwide and the determination of chemoprevention or chemoprophylaxis
compounds is important in an effort to reduce the risk of cancer (Kundu et al., 2004).
Differences in antimicrobial activity of medicinal plants are obviously related to differences in
their contents of active compounds (Boakye-Yiadom and Konning, 1975). Available reports tend
to show that alkaloids and flavonoids are the responsible compounds for the antimicrobial
activities in higher plants (Cordell et al., 2001). Moreover, it is also claimed that secondary
metabolites such as tannins and other compounds of phenolic nature are classified as active
82
antimicrobial compounds (Mitscher et al., 1972; Rojas et al., 1992). A study by Springfield et al.
(2005) of Chironia baccifera on the microchemical tests in their laboratories indicated the
presence of tannins and saponins but the absence for alkaloids and cardiac-, cyanogenic- and
anthraquinone glycosides. The presence of these active compound plus those explained by
Wolfender (1993) under 2.6.1.1 active ingredients, supports the antimicrobial activities of
Chironia baccifera as observed in this study.
Today, there is increased sensitivity towards traditional healers’ issues. Along with the rest of the
world, the South African Department of Health is looking at improving conditions for traditional
healers’ associations. In addition, the National Indigenous Knowledge Systems Program is
working towards registration with the objective that it will lead to the protection of intellectual
property rights, equitable compensation, promotion, and the improvement of traditional healing
systems (Kubukeli, 2000).
Owing to the fact that millions of South Africans rely on traditional medicines for their primary
healthy care needs, there is insufficient pragmatic information regarding the pharmacology and
toxicology of commonly used herbal remedies. This information should be available to health
care workers such as doctors, pharmacists, nurses, and social workers (Rodriguez-Fragoso et al.,
2008).
In the rural communities where there is limited access to medical facilities, people should be
empowered through education on proper use of medicinal plants as first aid remedies (Bodeker,
2001; Rabe and Van Staden, 1997). Establishing the antibacterial activity of these plants will
contribute to the systematic scientific investigation of indigenous South African medicinal
plants.
In the future, integrated research projects among scientists, clinical researchers, and industries
will be needed to concentrate all efforts toward innovative therapies for sepsis (Tetta et al.,
2003b). As technology offers devices to implement traditional or new modalities, the application
of a rigorous analysis derived from basic and clinical sciences in sepsis might lead to major
advances provided that randomized, controlled studies are performed. As the sepsis story
continues to unravel with the ongoing discovery of more malignant inflammatory mediators, the
development and use of extracorporeal blood purification therapies seems a logical, feasible and
exciting challenge. Continuous renal replacement therapy (CRRT), plasmafiltration, and coupled
83
plasma filtration adsorption (CPFA) demonstrate exciting potential for improving outcome in
critically ill septic subjects (Tetta et al., 2003a).
It is thus concluded that Harpephyllum caffrum, Hermannia cuneifolia and Chironia baccifera
do possess antimicrobial properties for at least certain microbes and that this activity is largely
dependent on the extract used. However, further studies are required in order to gain more clarity
as to the specificity and biochemical mechanisms responsible for the antimicrobial properties of
these three plants. The possible loss of volatile components present in the extracts during drying
and evaporation might have produced results different from those obtained in studies where other
methods of extract drying were employed.
The bioactive compounds responsible for antimicrobial activities of the three plants need to be
identified and isolated, and it should be taken into account that it might possibly be the
synergistic activity of two or more compounds that is responsible for the medicinal properties of
the three plants. It should also be taken into account that results obtained from in vitro assays
may not necessarily be reproducible in vivo due to the metabolic processes of the test subjects. It
is therefore, suggested that the extracts which showed antimicrobial activity during this study be
tested in vivo, and that their toxicity patterns and mutation-inducing capacities be established
further.
From the findings of antimicrobial activities of the plants under study, further work needs to be
done on the isolation, purification and structural elucidation of the bioactive compounds in these
plants. The ethnomedicinal study of plants is important for modern day medicine but its
usefulness cannot be over-emphasized if methods are not standardized to obtain comparable and
reproducible results. Other pharmacological studies like potentials for combination antimicrobial
chemotherapy and mechanisms of action are important additional tests to fully assess
antimicrobial activity of plant extracts, and these are subjects of intensive investigation in
research laboratories.
Ethnopharmacological research could play an important role in the worldwide HIV/AIDS
pandemic and associated opportunistic infections, such as tuberculosis and oral thrush.
Successful research in ethnopharmacology encompasses various disciplines which need to be
84
intergrated. Through scientific validation of effective remedies, coupled with training of
healthcare practitioners, it may be possible to bring traditional medicine to a level of efficiency
and safety where it can be regarded as an acceptable alternative to western healthcare systems.
85
REFERENCES
Abbu, R., Pillay, A.E., & Moodley, K.G. (2000). The use of ICP-AES and anodic stripping
voltammetry (ASV) to determine the levels of cadmium and lead in river water samples
from KwaZulu-Natal (KZN), South Africa. Journal of Trace and Microprobe Techniques
18: 83-97.
Abdulla, S., Abuzarqa, M., Afifi, F., Al-Khalil, S., Mahasneh, A., & Sabri, S. (1989). Effects of
3,3-di-0-methyl quercetin on guinea-pig isolated smooth muscle. Journal of Pharmacy
and Pharmacology 41: 138-141.
Acocks, J.P.H. (1975). Veld types of South Africa. Memoirs of Botanical Survey of South Africa
Botanical Research Institute. Pretoria: Department of Agriculture and Water Supply, p.
57.
Adhikarla, S. (1984). Root flavanoids. Bot Rev 56: 29-37. In: Masika, P.J.& Afolayan, A.J.
(2003). An ethnobotanical study of plants used for the treatment of livestock diseases in
the eastern cape province, South Africa. Pharmaceutical Biology 41: 16-21.
Afolayan, A.J. (2003). Extracts from the shoot of Arctotis arctotoides inhibits the growth of
bacteria and fungi. Pharmaceutical Biology 41: 22-25.
Afolayan, A.J., Grierson, D.S., Kambizi, L., Madamombe, I., & Masika, P. (2002). In vitro
antifungal activity of some South African medicinal plants. South African Journal of
Botany 68: 72-76.
Afolayan, A.J. & Meyer, J.J.M. (1997). The antimicrobial activity of 3,5,7-trihydroxyflavone
isolated from the shoots of Helichrysum aureonitens. Journal of Ethnopharmacology 57:
177-181.
Afsari, M., Beasley, S.W., Maoate, K., & Heckert, K. (2002). Attitudes of pacific parents to
circumcision of boys. Pacific Health Dialogue 9: 29-33.
Ahmad, I., Mehmood, Z., & Mohammad, F. (1998). Screening of some Indian medicinal plants
for their antimicrobial properties. Journal of Ethnopharmacology 62: 183-193.
86
Akerele, O. (1993). Nature’s medicinal bounty: don’t throw it away. World Health Forum 14:
390-395.
Ali-Shtayeh, M.S., & Abu Ghdeib, S.I. (1999). Antifungal activity of plant extracts against
dermatophytes. Mycoses 42: 665-672.
Alkofahi, A., Batshoun, R., Owais, W., & Najib, N. (1997). Biological activity of some
Jordanian medicinal plant extracts. Part II. Fitoterapia 68: 163-168.
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference:
definitions for sepsis and organ failure and guidelines for the use of innovative therapies
in sepsis. (1992).Critical Care Medicine 20: 864-74. In: Dombrovskiy, V., Martin, A.,
Sunderram, J., & Paz, H. (2006). Use of drotrecogin alfa (activated) for severe sepsis in
New Jersey acute care hospitals. American Society of Health-System Pharmacists. Vol.
63, p. 1151-56.
American College of Emergency Physicians, (2003). Clinical policy for children younger than
three years presenting to the emergency department with fever. Annal Emergency
Medicine 42: 530-45. In: Robinson, D.T., Kumar, P., & Cadichon, S.B. (2008). Neonatal
Sepsis in the Emergency Department. Clinical Pediatric Emergency Medicine 9: 160168.
Andrews, J.M. (2001). Determination of Minimum Inhibitory Concentrations. Journal of
Antimicrobial Chemotherapy 48, Suppl. S1: 5-16. Retrieved on March 17, 2008 from
http://atoz.ebsco.com/titles.asp?Id=zruopel&sid=96235339&TabID=20
Anonymous, (1992). Herbal remedies. Pharmaceutical Marketing 4: 24.
Anonymous, (1995). The World Health Report: Bridging the gaps. Geneva, Switzerland: WHO.
Anonymous, (1997). Natural peptides offer safe alternative to agricultural fungicides.
Biotechnology Lab. International 2 (5): 1.
Ashafa, A.O.T., Grierson, D.S., & Afolayan, A.J. (2008). Antimicrobial activity of extracts from
Felicia muricata thunb. Journal of Biological Sciences 8(6): 1062-1066.
87
Bagghi, A.K. (2000). Alternative medicine- Old wine in a new bottle. Indian Medicine
Association 98: 332-333.
Balandrin, M.F., Kinghorn, A.D., & Farnsworth, N.R. (1993). Plant derived natural products in
drug discovery and development: an overview in Human medicinal agents from plants.
Kinghorn, A.D. and Balandrin, M.F. (Eds). Washington DC, USA. p. 2-12.
Balandrin, M.F., Klocke, J.A., Wurtele, E.S., & Bollinger, W.H. (1985). Natural plant chemicals:
Sources of industrial and medicinal materials. Science 228: 1154-1160.
Balunas, M.J., & Kinghorn, A.D. (2005). Drug discovery from medicinal plants. Life Sciences
78: 431-441.
Baue, A.E., Durham, R., & Faist, E. (1998). Systemic inflammatory response syndrome (SIRS),
Multiple Organ Dysfunction Syndrome (MODS), Multiple Organ Failure (MOF): are we
winning the battle? Shock 10(2): 79-89. In: Tetta, C., Bellomo, R., & Ronco, C. (2003).
Artificial Organ Treatment for Multiple Organ Failure, Acute Renal Failure, and Sepsis:
Recent New Trends. International Society for Artificial Organs. Vol. 27 (3): 202-213.
Bauman, R. (2007). Microbiology with Diseases by Taxonomy. (2nd ed.). San Francisco: Pearson
Benjamin Cummings.
Beal, A.L., & Cerra, F.B. (1994). Multiple organ failure symdrome in the 1990s. Systemic
inflammatory response and organ dysfunction. JAMA 271(3):226-33. In: Tetta, C.,
Bellomo, R., & Ronco, C. (2003). Artificial Organ Treatment for Multiple Organ Failure,
Acute Renal Failure, and Sepsis: Recent New Trends. International Society for Artificial
Organs. Vol. 27 (3): 202-213.
Ben Chaim, J., Livne, P.M., Binyamini, J., Hardak, B., Ben-Meir, D., & Mor, Y. (2005).
Complications of circumcision in Israel: a one year multicenter survey. Israel Medical
Association Journal 7: 368-70.
Benzi, G., & Ceci, A. (1997). Herbal medicines in European regulation. Pharmacology Research
35: 355-362.
88
Bergeron, C., Marston, A., Gauthier, R., & Hostettmann, K. (1996). Screening of plants used by
North American Indians for antifungal, bactericidal, larvicidal, and molluscicidal
activities. International Journal of Pharmacognosy 34: 233-242.
Bhanumathi, N., Paulsen, B.S, & Pushpangadan, P. (1999). An Ethnopharmacological Study
from the Coimbatore District, Tamil Nadu, India: Traditional Knowledge compared with
Modern Biological Science. Pharmaceutical Biology, Vol. 37, No. 5, p. 387.
Binning, K., & Baird, D. (2001). Survey of heavy metals in the sediments of the Swartkops River
Estuary. Port Elizabeth [South Africa]. Water SA 27: 461-466.
Boakye-Yiadom, K., & Konning, G.H. (1975). Incidence of antibacterial activity in the
Connaraceae. Planta Medicina 28: 397-400.
Bodeker, G. (2001). A framework for cost benefits analysis of traditional medicine &
conventional medicine. In: Chaudhury, Ranjit Roy. Traditional Medicine. WHO:
SEARO.
Bodeker, G.C. (1994). Traditional health knowledge and public policy. Nature and Resources
30: 5-16.
Boily, Y., & Van Puyvelde, L. (1986). Screening of medicinal plants of Rwanda (Central Africa)
for antimicrobial activity. Journal of Ethonpharmacology 16: 1-16.
Bombardelli, E. (1996). New perspectives in botanicals. Presented at the Workshop ‘From Acts
to Actions when dealing with Botanicals’. Milan [Indena], September 10.
Bopana, N., & Saxena, S. (2007). Asparagus racemosus-ethnopharmacological evaluation and
conservation needs. Journal of ethnopharmacology 110: 1-15.
Botha, J.P. (1939). South African Department Agriculture Forest Representative 54. In: Watt,
J.M., & Breyer-Brandwijk, M.G. (1962). The medicinal and poisonous plants of Southern
and Eastern Africa. (2nd ed.). London: Livingstone.
Brandt, H.D., Osuch, E., Mathibe, L., & Tsipa, P. (1995). Plants associated with accidental
poisoned patients presenting at Ga-Rankuwa Hospital. Pretoria: Suid-Afrikaanse Tyskrif
vir wetenskap 9: 57-59.
89
Brantner, A., Males, Z., Pepeljnjak, S., & Antolic, A. (1996). Antimicrobial activity of Paliurus
spina-christi Mill. (Christhorn). Journal of Ethnopharmacology 52: 119-122.
Brown, D.L. (1969). A study of the animal and crop production systems and potential of the
Bantu Ciskeian territories. DSc (Agric.) thesis.
Bruneton, J. (1995). Pharmacognosy, phytochemistry, medicinal plants. Intercept, Hampshire.
In: Van Wyk, B.E., Van Oudtshoorn, B., Gericke, N. (1997). Medicinal Plants of South
Africa. (1st ed). Pretoria: Briza Publications.
Bryce, K. (1992). The fifth kingdom. Ontario: Mycologic Publication.
Bulmer, A.C., Ried, K., Coombes, J.S., Blanchfield, J.T., Toth, I., & Wagner, K.H. (2007). The
anti-mutagenic and antioxidant effects of bile pigments in the Ames Salmonella test.
Mutation Research 629: 122-132.
Burtt, D. J. (1912). Rep. Veterinary Res. South Africa 2: 181. In: Watt, J.M., & BreyerBrandwijk, M.G. (1962). The Medicinal and Poisonous Plants of Southern and Eastern
Africa. (2nd ed). Edinburgh & London: E. & S. Livingstone Ltd, p. 254.
Buwa, L.V., & Van Staden, J. (2007). Effects of collection time on the antimicrobial activities of
Harpephyllum caffrum bark. South African Journal of Botany 73: 242-247.
Cardoso, C.R.P., de Syllos Cólus, I.M., Bernardi, C.C., Sannomiya, M., Vilegas, W., & Varanda,
E.A. (2006). Mutagenic activity promoted by amentoflavone and methanolic extract of
Byrsonima crassa Niedenzu. Toxicology 225: 55-63.
Cavalcanti, B.C., Costa-lotufo, L.V., Moraes, M.O., Burbano, R.R., Silveira, E.R., Cunha,
K.M.A., Rao, V.S.N., Moura, D.J., Rosa, R.M., Henriques, J.A.P., & Pessoa, C. (2006).
Genotoxicity evaluation of kaurenoic acid, a bioactive diterpenoid present in Copaiba oil.
Food and Chemical Toxicology 44: 388-392.
Chan, K. (2003). Some aspects of toxic contaminants in herbal medicines. Chemosphere 52:
1361-1371.
Chen, S.B., Liu, H.P., Tian, R.T., Yang, D.j., Chen, S.L., Xu, H.X., Chan, A.S.C., & Xie, P.S.
(2006). Journal of Chromatography A. 1121:114. In: Cieśla, L., & Waksmundzka90
Hajnos, M. (2009). Two-dimensional thin-layer chromatography in the analysis of
secondary plant metabolites. Journal of Chromatography A. 1216: 1035-1052.
Chironia bacifera (Plant name), by Carolus, B. (2004). Harold Porter NBG. Retrieved on: 31st
July, 2009 from www.plantzafrica.com/plantcd/chironbac.htm.
Cieśla, L., & Waksmundzka-Hajnos, M. (2009). Two-dimensional thin-layer chromatography in
the analysis of secondary plant metabolites. Journal of Chromatography A. 1216: 10351052.
Coetzee, E. (2000). The magic of muti plants. Farmers’s Weekly 14: 26-29.
Coghlan, A. (1996). Focus: A plateful of medicine. New Scientist. Nov. p.12-13.
Committee of National Pharmacopoeia. (2005). Pharmacopoeia of P.R. China, Press of
Chemical Industry: Beijing, China. In: Gu, M., Su, Z., & Ouyang, F. (2006).
Fingerprinting of Salvia miltiorrhiza Bunge by Thin-Layer Chromatography Scan
Compared with High Speed Countercurrent Chromatography. Journal of Liquid
Chromatography & Related Technologies 29: 1503-1514.
Cordell, G.A., Quinn-Beattie, M.L., & Farnsworth, N.R. (2001). The potential of alkaloids in
drug discovery. Phytotherapy Research 15: 183-205.
Cotton, C.M. (1996). Ethnobotany: Principles and Applications. Chichester: Willey.
Cowan, M.M. (1999). Plant products as antimicrobial agents. Clinical Microbiological Reviews
Oct. 564-582.
Cox, P.A. & Balick, M.J. (1994). The ethnobotanical approach to drug discovery. Scientific
American 270: 60-65.
Cragg, G.M., Boyd, M.R., Cardellina, I., Newman, D.J., Snader, K.M., & McCloud, T.G. (1994).
Ethnobotany and Drug Discovery: Experience of the US National Cancer Institute.
Chadwick and March Press: Chichester, p.40-47.
Cragg, G.M., Boyd, M.R., Cardellina, J.H., Grever, M.R., Schepartz, S.A., Snader, K.M. &
Surfhess, M. (1993). Role of plants in the National Cancer Institute intramural research
91
on human immunodeficiency virus inhibitory and antitumour plant natural products. In:
Kinghorn, A.D. & Balandrin, M.E. (Eds).
Human medicinal agents from plants.
American Chemical Society. USA: Washington DC, p. 80-95.
Cunningham, A.B. (1993). African Medicinal Plants: Setting Priorities at the Interface between
Conservation and Primary Health Care. People and Plants Working Paper 1. UNESCO:
Paris.
Cunningham, A.B. (1991). Development of a conservation Policy on commercially exploited
medicinal plants: a case study from Southern Africa, p. 337-358. In: Akerele, O.,
Heywood, V., & Synge, H. (Eds). Conservation of Medicinal Plants. Cambridge
University Press.
Dantra,
Retrieved
22nd
on
March,
2008.
(http://www.who.int/mediacentre/factsheet/fs134/en/print.html)
Dawid, B. pers. comm. In: Van Wyk, B., & Gericke, N. (2000). People’s plants – A Guide to
Useful Plant s of Southern Africa. (1st ed). Pretoria, [South Africa]: Briza Publications, p.
182.
Déciga-Campos, M., Rivero-Cruz, I., Arriaga-Alba, M., Castañeda-Corral, G., Angeles-López,
G.E., Navarrete, A., & Mata, R. (2007). Acute toxicity and mutagenic activity of
Mexican plants used in traditional medicine. Journal of Ethnopharmacology 110: 334342.
De Sá Ferreira, I.C.F., & Ferrão Vargas, V.M. (1999). Mutagenicity of medicinal plant extracts
in Salmonella/microsome assay. Phytotherapy Research 13: 397-400.
De Smet, P.A.G.M. (2005). Herbal Medicine in Europe — Relaxing Regulatory Standards. New
England Journal of Medicine, Vol 352(12): 1176-1178.
Dictionary of Natural Products on CD-ROM, (1996). Release 4:2, London: Chapman & Hall. In:
Van Wyk, B.E., Van Oudtshoorn, B., Gericke, N. (1997). Medicinal Plants of South
Africa. (1st ed). Pretoria: Briza Publications.
92
Diekema, D.J., Beekmann, S.E., Chapin, K.C., Morel, K.A., Munson, E., & Doern, G.V. (2003).
Epidemiology and outcome of nosocomial and community-onset bloodstream infection.
Journal of Clinical Microbiology 41(8): 3655-60.
Dilika, F., Afolayan, A.J., & Meyer, J.J.M. (1997). Comparative antibacterial activity of two
Helichrysum species used in male circumcision in South Africa. South African Journal of
Botany 63: 158-159.
Dold, A.P., & Cocks, M.L. (2002). The trade in medicinal plants in the Eastern Cape Province,
South Africa. South African Journal of Science 98: 589-597.
Dombrovskiy, V., Martin, A., Sunderram, J., & Paz, H. (2006). Use of drotrecogin alfa
(activated) for severe sepsis in New Jersey acute care hospitals. American Society of
Health-System Pharmacists. Vol. 63, 1151-56.
Drouhent, E., & Dupont, B. (1989). Fluconazole for the treatment of fungal diseases in
immunosuppressed patients. Annals New York Academy of Science 544: 564-570.
Dube, M.G., & Mutloane, M. (2001). Health sector under stress. Enterprise 156: 24-25.
Eidam, P.M., Schariter, J.A., Fried, B., & Sherma, J. (2001). HPTLC analysis of tissue and blood
of Biomphalaria glabrata snails to assess the effects of a diet of Romaine lettuce leaf
versus midrib on the concentrations of lipids, pigments, and carbohydrates. Journal of
Liquid Chromatography and Related Technologies 24: 1467-1478. In: Sherma, J., &
Fried, B. (2005). Thin Layer Chromatographic Analysis of Biological Samples. A
Review. Journal of Liquid Chromatography and Related Technologies. Taylor & Francis,
Inc. 28: 2297-2314.
Eisenberg, D.M., Kessler, R.C., Foster, C., Norlock, E.E., Calkins, D.R., & Delbanco, T.L.
(1993). Unconventional medicines in the United States – prevalence, costs and patterns of
use. New England Journal of Medicine 328: 246-252.
Elgorashi, E.E., Taylor, J.L.S., Maes, A., De Kimpe, N., Van Staden, J., & Verschaeve, L.
(2002). The use of plants in traditional medicine: potential genotoxic risks. South African
Journal of Botany 68: 408-410.
93
Elgorashi, E.E., Taylor, J.L.S., Maes, A., Van Staden, J., De Kimpe, N., & Verschaeve, L.
(2003). Screening of medicinal plants used in South African traditional medicine for
genotoxic effects. Toxicology Letters 143: 195-207.
Elmi, A.S., Svensen, A.B., Scheffer, J.J.C., & Verpoorte, R. (1986). Screening of some Somalian
medicinal plants for antibacterial activity. Journal of Ethnopharmacology 17: 283-288.
Eloff, J.N. (1998a). A sensitive and quick microtitre plate method to determine the minimum
inhibitory concentration of plant extracts for bacteria. Planta Medica 64: 711-713.
Eloff, J.N. (1998b). Which extracts should be used for screening and isolation of antimicrobial
components from plants? Journal of Ethnopharmacology 60: 1-8.
Eloff, J.N. (1999). It is possible to use herbarium specimens to screen for anti-bacterial
components in some plants. Journal of Ethnopharmacology 67: 355-360.
Eloff, J.N. (2000). On expressing the antibacterial activity of plant extracts – a small first step in
applying scientific knowledge to rural primary health care. South African journal of
Science 96: 116-118.
El Sherbeiny, A.E.A., & El Ansari, M.A. (1976). The polyphenolics and flavonoids of
Harpephyllum caffrum. Planta Med. 29: 129-132. In: Van Wyk, B.E., Van Oudtshoorn,
B., Gericke, N. (1997). Medicinal Plants of South Africa. (1st ed). Pretoria: Briza
Publications.
El Sohly, M.A., Gul, W., & Murphy, T.P. (2004). Analysis of the anthraquinones aloemodin and
aloin by gas chromatography/mass spectrometry. International Immunopharmacology 4:
1739-1744.
Elvin-Lewis, M. (2001). Should we be concerned about herbal remedies? Journal of
Ethnopharmacology 75: 141-164.
Fabricant, D.S., & Farnsworth, N.R. (2001). The value of plants used in traditional medicine for
drug discovery. Environmental Health Perspectives 109: 69-75.
Fanaroff, A., & Martin, R.J. (2006). Neonatal-perinatal medicine, disease of the fetus and infant.
(8th ed). St Louis: Mosby. In:
Robinson, D.T., Kumar, P., Cadichon, S.B. (2008).
94
Neonatal Sepsis in the Emergency Department. Clinical Pediatric Emergency Medicine
9: 160-168.
Fan-Havard, P., Capano, D., Smith, S.M., Mangia, A., & Eng, R.H.K. (1991). Development of
resistance in Candida isolates from patients receiving prolonged antifungal therapy.
Antimicrobial Agents and Chemotherapy 35: 2302-2305.
Farnsworth, N.R., (1984a). Economic Botany 38: 4-13.
Farnsworth, N.R. (1984b). The role of medicinal plants in drug development. In: KrogsgaardLarsen, P., Christensen, S.B., & Kofod H, (Eds)., Natural Products and Drug
Development. Balliere, London: Tindall and Cox, p. 8-98.
Farnsworth, N.R., & Soejarto, D.D. (1991). Potential consequences of plant extinction in the
United States in the current and future availability of prescription drugs. Economic
Botany 39: 231-240.
Farnsworth, N.R. (1994). Ethnopharmacology and drug development. Ciba Foundation
Symposium 185: 42-59.
Felhaber, T. (1999). South African Primary Health Care Handbook: Combining Western and
Traditional Practices. Cape Town: Kagiso Publishers, pages: 21-43; 129-134; 139-141.
Felicia muricata (Plant name), by Hyde, M.A., & Wursten, B. (2009). Flora of Zimbabwe.
Retrieved
on:
19th
August,
2009
from
www.zimbabweflora.co.zw/speciesdata/species.php?species_id=158820.
Fennell, C.W., Light, M.E., Sparg, S.G., Stafford, G.I., & Van Staden, J. (2004). Assessing
African medicinal plants for efficacy and safety: agricultural and storage practices.
Journal of Ethnopharmacology 95: 113-121.
Fishman, J.A., & Rubin, R.H. (1998). Infection in organ transplant recipients. New England
Journal of Medicine 338: 1741.
Fleming, R.V., Walsh, T.J., & Anaissie, E.J. (2002). Emerging and less common fungal
pathogens. Infectious Disease Clinics of North America 16: 915-933.
95
Fourie, T.G., Swart, I., & Snyckers, F.O. (1992). Folk medicine: a viable starting point for
pharmaceutical research. South African Journal of Science 88:190-192.
Fuzzati, N. (2004). Analysis methods of ginsenosides. Journal of Chromatography B. 812: 119133. In: Gu, M., Su, Z., & Ouyang, F. (2006). Fingerprinting of Salvia miltiorrhiza Bunge
by Thin-Layer Chromatography Scan Compared with High Speed Countercurrent
Chromatography. Journal of Liquid Chromatography & Related Technologies 29: 15031514.
Garbino, J., Kolarova, L., Lew, D., Hirschel, B., & Rohner, P. (2001). Fungemia in HIV-infected
patients: a 12-year study in a tertiary care hospital. AIDS Patient Care STDs 15: 407-410.
George, J., Laing, M., & Drewes, S.E. (2001). Phytochemical research in South Africa. South
African Journal of Science 97(3/4): 93-106.
George, J., & Van Staden, J. (2000). Intellectual property rights: Plants and Phytomedicinals –
Past history, Present scenario and Future prospects in South Africa. South African
Journal of Science 96: 433-442.
Ghazal, S.A., Abuzarqa, M., & Mahasneh, A.M. (1992). Antimicrobial activity of Polygonum
equisetiforme extracts and flavonoids. Phytotherapy Research 6: 265-269.
Goldring, J. (1996). A Plant Red Data list for Southern Africa. SABONET News, 4: 111-118.
Gould, M., & Mackenzie, F.M. (2002). Antibiotic exposure as a risk factor for emergence of
resistance: the influence of concentration. Journal of Applied Microbiology Symposium
Supplement, 92: 78-84.
Gibbons, S., & Gray, A.I. (1998). Isolation by planar chromatography. In: Cannell, R.J.P. (Ed.).
Methods in Biotechnology. Natural Products Isolation, Vol 4. Totowa: Humana Press
Inc.
Gibbons, S. (2003). An overview of plant extracts as potential therapeutics. Expert Opinion
Therapy Pat. 13(4): 489-497.
Gogtay, N.J., Bhatt, H.A., Dalvi, S.S. & Kshirsagar, N.A. (2002). The use and safety of nonallopathic Indian medicines. Drug safety 25: 1005-1019.
96
Govender, S., Du Plessis-Stoman, D., Downing, T.G., & Van de Venter, M. (2006). Traditional
herbal medicines: microbial contamination, consumer safety and the need for standards.
South African Journal of Science 102: 253-255.
Green, R.J. (2004). Antioxidant Activity of Peanut Plant Tissues. Masters Thesis. North Carolina
State University. USA.
Grierson, D.S., & Afolayan, A.J. (1999). Antibacterial activity of some indigenous plants used
for the treatment of wounds in the Eastern Cape, South Africa. Journal of
Ethnopharmacology 66: 103-106.
Gurib-Fakim, A. (2006). Medicinal plants: Traditions of yesterday and drugs of tomorrow.
Molecular aspects of medicine 27: 1-93. In: van Vuuren, S.F. (2008). Antimicrobial
activity of South African medicinal plants. Journal of Ethnopharmacology.
doi:10.1016/j.jep.2008.05.038
Hamburger, M.O., & Cordell, G.A. (1987). A direct bioautographic TLC assay for compounds
possessing anti-bacterial activity. Journal of Natural Products 50: 19-22. In: Fennell,
C.W., Lindsey, K.L., McGaw, L.J., Sparg, S.G., Stafford, G.I., Elgorashi, E.E., Grace,
O.M., & van Staden, J. (2004). Assessing African medicinal plants for efficacy and
safety: pharmacological screening and toxicology. Journal of Ethnopharmacology 94:
205-217.
Hammer, K.A., Carson, C.F., & Riley, T.V. (1999). Antimicrobial activity of essential oils and
other plant extracts. Journal of Applied Microbiology 86(6): 985. In: Ncube, N.S.,
Afolayan, A.J., & Okoh, A.I. (2008). Assessment techniques of antimicrobial properties
of natural compounds of plant origin: current methods and future trends. African Journal
of Biotechnology 7(12): 1797-1806.
Harborne, J.B. (1998). Phytochemical methods: A guide to modern techniques of plant analysis.
London: Chapman & Hall.
Harpephyllum caffrum (Plant name), by Mhlonishwa, D.D. (2004). Water Sisulu National
Botanical
Garden.
Retrieved
on
www.plantzafrica.com/planthij/harpephylcaf.htm.
97
31st
July,
2009
from
Hayes, L.E. (1947). Survey of higher plants for presence of antibacterial substances. Botanical
Gazette
108(3):
408-414.
Retrieved
on
16th
November,
2009
from
http://www.jstor.org/stable/2472718?seq=4.
Hawksworth, D.L. (1974). Mycologist’s Handbook. Kew: CAB International. Retrieved on 23rd
March, 2008 from http://en.Wikipedia.org/wiki/Mycology#References.
Helwig, D. (2000). Traditional African Medicine. The Gale Encyclopedia of Alternative
Medicine. Krapp, K., & Longe, J.L. (Eds). Farmington Hills, Mich: Gale group.
Henrici, M. (1952). Ouderstepoort. Journal of Veternary Science 25: 45. In: Watt, J.M., &
Breyer-Brandwijk, M.G. (1962). The Medicinal and Poisonous Plants of Southern and
Eastern Africa. (2nd ed). Edinburgh & London: E. & S. Livingstone Ltd, p. 254.
Hermannia cuinefolia (Plant name), by Sachse, B. (2007). National Herbarium, Pretoria.
Retrieved on 31st July, 2009 from www.plantzafrica.com/planthij/hermannia.htm.
Heron, M. (2007). Deaths: leading causes for 2004. Natal Vital Statistical Representative 56: 195. In: Robinson, D.T., Kumar, P., & Cadichon, S.B. (2008). Neonatal Sepsis in the
Emergency Department. Clinical Pediatric Emergency Medicine 9: 160-168.
Hewson, M.G. (1998). Traditional Healers in Southern Africa. Annals of Internal Medicine
128(12): 1029-1034.
Hoareau, L., & Dasilva, E.J. (1999). Medicinal plants: A re-emerging health aid. Plant
Biotechnology 2:1-6.
Hostettmann, K. (1999). Strategy for the biological and chemical evaluation of plant extracts.
Pure Applied Chemistry 70: 1-9.
Hostettmann, K., Wolfender, J., & Terreaux, C. (2001). Modern screening techniques for plant
extracts. Pharmaceutical Biology 39: 18-32.
Hughes, I. (2002). Science in Africa Magazine. Issue 56.
Hugo, W.B. (1992). Pharmaceutical Microbiology. Hugo, W.B., & Russell, A.D., (Eds.). (5th
ed.). Blackwell Scientific Publications.
98
Hutchings, A., Scott, A.H., Lewis, G., & Cunningham, A.B. (1996). Zulu Medicinal Plants. An
inventory. Pietermaritzburg: University of Natal Press.
Hutchings, A. (1989a). A survey and analysis of traditional medicinal plants as used by the Zulu,
Xhosa and Sotho. Bothalia 19:111-123.
Hutchings, A. (1989b). Observations on plant usage in Xhosa and Zulu medicine. Bothalia
19:225-235.
Hutchings, A., & Van Staden, J. (1994). Plants used for stress related ailments in traditional
Zulu, Xhosa and Sotho medicine. Part 1: Plants used for headaches. Journal of
Ethnopharmacology 52: 89-124.
Ison, C.A., Dillon, J.R., & Tapsall, J.W. (1998). The epidemiology of global antibiotic resistance
among Neisseria gonorrhoeae and Haemophilus ducreyi. Lancet 351(Suppl. 3): 811.
Jain, S.K. (1994). Ethnobotany and research on medicinal plants in India. Ciba Found
Symposium 185: 153-164.
Johannes, (Rev.). (1915). Native medicine. South African Journal of Science 11: 404-405.
Jones, N.P., Arnason, J.T., Abou-Zaid, M., Akpagana, K., Sanchez-Vinda, P., & Smith, M.L.
(2000). Antifungal activity of extracts from medicinal plants used by First Nations
Peoples of eastern Canada. Journal of Ethnopharmacology 73: 191-198.
Jordan, A., & Kruger, H. (1993). Pollen wall ontogeny of Felicia muricata (Asteraceae). Annals
of Botany 71: 97-105. In: Ashafa, A.O.T., Grierson, D.S., & Afolayan, A.J. (2008).
Antimicrobial activity of extracts from Felicia muricata thunb. Journal of Biological
Sciences 8(6): 1062-1066.
Keasah, C., Odugbmi, T., Ben Redjeb, S., Boye, C.S., Dosso, M. and the members of Palm
Project, (1998). Prevalence of MRSA in eight African hospitals and Malta. Poster E.093,
38th ICAAC, San Diego: September 24-28.
Kelbergh, B.J. (1997). Trends in immunotherapy of fungal infections. European Journal of
Clinical Microbiology Infectious Diseases 16: 51-55.
99
Kelmanson, J.E., Jäger, A.K., & Van Staden, J. (2000). Zulu medicinal plants with antibacterial
activity. Journal of Ethnopharmacology 69: 241-246.
Khafagi, I.K., & Dewedar, A. (2000). The efficiency of random versus ethno-directed research in
the evaluation of Sinai medicinal plants for bioactive compounds. Journal of
Ethnopharmacology 71: 365-376.
Khan, M.R., Mutasa, S.L., Ndaalio, G., & Wevers, H. (1978). Antibiotic action of constituents of
the roots of Euclea natalensis A.D.C. Pakistan Journal of Scientific and Industrial
Research 21: 197-199.
Kinghorn, A.D., & Balandrin, M.F. (1993). Human medicinal agents from plants. ACS
Symposium Series 534, American Chemical Society, Washington. In: Van Wyk, B.-E.,
Van Oudtshoorn, B., & Gericke, N. (1997). Medicinal Plants of South Africa. Pretoria:
Briza Publications.
Kling, H. (1923). Die Sieketrooster. Cape Town: Van de Sandt de Villiers. In : Watt, J.M., &
Breyer-Brandwijk, M.G. (1962). The Medicinal and Poisonous Plants of Southern and
Eastern Africa. (2nd ed). Edinburgh & London: E. & S. Livingstone Ltd, p. 45.
Koduru S., Grierson D.S., & Afolayani A.J. (2006). Antimicrobial activity of Solanum
aculeastrum. Pharmacology Biology 44(4):283-286.
Kokoska, L., Polesny, Z., Rada, V., Nepovim, A., & Vanek, T. (2002). Screening of some
Siberian medicinal plants for antimicrobial activity. Journal of Ethnopharmacology 82:
51-53.
Kong, J.M., Goh, N.K., Chia, L.S., & Chia, T.F. (2003). Recent advances in traditional plant
drugs and orchids. Acta Pharmacologica Sinica 24(1): 7-21.
Koo, B., & Wright, B.D. (1999). The role of biodiversity products as incentives for conserving
biological diversity: some instructive examples. The Science of The Total Environment
240: 21-30.
Kowalski, R., & Kedzia, B. (2007). Antibacterial activity of Silphium perfoliatum extracts.
Pharmacological Biology 44: 494-500. In: Ashafa, A.O.T., Grierson, D.S., & Afolayan,
100
A.J. (2008). Antimicrobial activity of extracts from Felicia muricata thunb. Journal of
Biological Sciences 8(6): 1062-1066.
Kubukeli, P.S. (2000). Traditional healing practice using medicinal herbs. Present and Future.
Cape Town: The Lancet, siv24.
Kundu, J.K., Mossanda, K.S., Na, H.-K., Surh, Y.-J. (2004). Inhibitory effects of the extracts of
Sutherlandia frutescens (L.) R. Br. and Harpagophytum procumbens DC. on phorbol
ester-induced COX-2 expression in mouse skin: AP-1 and CREB as potential upstream
targets. Cancer Letters 218: 21-31. In: Reid, K.A., Maes, A., Van Staden, J., De Kimpe,
N., Mulholland, D.A., & Verschaeve, L., (2006). Evaluation of the mutagenic and
antimutagenic effects of South African plants. Journal of Ethnopharmacology 106: 4450.
Lall, N., & Meyer, J.J.M. (2000). Antibacterial activity of water and acetone extracts of the roots
of Euclea natalensis. Journal of Ethnopharmacology 72: 313-316.
Lall, N. (2000). Isolation and identification of naphthoquinones from Euclea natalensis with
activity against Mycobacterium tuberculosis, other pathogenic bacteria and Herpes
Simplex Virus. Ph.D. dissertation, Department of Botany, University of Pretoria, South
Africa.
Lampinen, J. (2005). Continuous Antimicrobial Susceptibility Testing in drug discovery. Drug
Plus International. Retrieved on 24th August, 2009 from http://www.thermo-readingroom.com/files/application_pdfs/File_30585.pdf.
Lerman, J. (2005). Herbal Medicine in Children: Caveat Medicus. Pediatric Anesthesia, Vol.
15(6): 443-445.
Li Chaojin, (1987). Management of Chinese traditional drugs. The American Journal of Chinese
Medicine, Supplement No.1.
Light, M.E., Sparg, S.G., Stafford, G.I., & Van Staden, J. (2005). Riding the wave: South
Africa’s contribution to ethnopharmacological research over the last 25 years. Journal of
Ethnopharmacology 100: 127-130.
101
Li, H.B., Jiang, Y., & Chen, F. (2004). Separation methods used for Scutellaria baicalensis
active components. Journal of Chromatography B. 812: 277-290. In: Gu, M., Su, Z., &
Ouyang, F. (2006). Fingerprinting of Salvia miltiorrhiza Bunge by Thin-Layer
Chromatography Scan Compared with High Speed Countercurrent Chromatography.
Journal of Liquid Chromatography & Related Technologies 29: 1503-1514.
Lin, J., Opoku, A.R., Geheeb-Keller, M., Hutchings, A.D., Terblanche, S.E., Jäger, A.K., & Van
Staden, J. (1999). Preliminary screening of some traditional Zulu medicinal plants for
anti-inflammatory and anti-microbial activities. Journal of Ethnopharmacology 68: 267274.
Longe, L.J., & Frey, P.F. (2006). Septicemia – Blood poisoning, Encyclopedia of alternative
medicine,
(2nd
ed.).
Retrieved
on
10th
March,
2008.
(http://www.answers.com/topic/blood-poisoning?cat=health)
Lovkova, M.Y., Buzuk, G.N., Sokolova, S.M., & Kliment’eva, N.I. (2001). Chemical features of
medicinal plants (review). Applied Biochemistry and Microbiology 37(3): 229-237.
Madamombe, I.T., & Afolayan, A.J. (2003). Evaluation of antimicrobial activity of extracts from
South African Usnea barbata. Pharmaceutical Biology 41: 199-202.
Magoha, G.A. (1999). Circumcision in various Nigerian and Kenyan hospitals. East African
Medicine Journal. 76: 583-86. In: Peltzer, K., Nqeketo, A., Petros, G., & Kanta, X.
(2008). Traditional circumcision during manhood initiation rituals in the Eastern Cape,
South Africa: a pre-post intervention evaluation. BioMed Central Public Health. 8: 64.
(http://www.biomedcentral.com/1471-2458/8/64)
Mahasneh, A.M., & El-Oqlah, A.A. (1999). Antimicrobial activity of extracts of herbal plants
used in the traditional medicine in Jordan. Journal of Ethnopharmacology 64: 271-276.
Maher, P. (1999). A review of traditional aboriginal health beliefs. Australian Journal of Rural
Health, 7: 229-236.
Makunga, N.P., Jäger, A.K., & Van Staden, J. (2008). Contribution of South African plants to
medicinal plant biotechnology. SAAB Annual Meeting Abstracts, p.372.
102
Mammem, M., & Cloete, E. (1996). Bridging the gap between traditional and ‘modern’
medicine. Veld and Flora 82: 2.
Mander, M., & Le Breton, G. (2006). Overview of the medicinal plants industry in Southern
Africa. In: Diederichs, N. (Ed.). Commercialising Medicinal Plants-A Southern African
Guide. Stellenbosch: Sun Press, 1-8.
Mander, M. (1998). Marketing of indigenous medicinal plants in South Africa. A case study in
Kwa-Zulu Natal. FAO, Rome.
Manji, K.P. (2000). Circumcision of the young infant in a developing country using the
Plastibell. Annal Tropical Paediatric 20:101-4.
Marimoto, K., & Fujimoto, M. (1999). Report of questionnaire survey for MRSA and Penicillin
resistant Streptococcus pneumoniae in the Kinki district. Kansenshogaku Zasshi 73: 584592.
Marloth, R. (1913-32). The Flora of South Africa. London: Wesley. In: Watt, J.M., & BreyerBrandwijk, M.G. (1962). The Medicinal and Poisonous Plants of Southern and Eastern
Africa. (2nd ed). Edinburgh & London: E. & S. Livingstone Ltd, p. 254.
Maron, D.M., & Ames, B.N. (1983). Mutation Research 113: 173.
Masika, P.J., & Afolayan, A.J. (2002). Antimicrobial activity of some plants used for the
treatment of livestock disease in the Eastern Cape, South Africa. Journal of
Ethnopharmacology 83: 129-134.
Masika, P.J., Sonandi, A., & Van Averbeke, W. (1997). Perceived causes, diagnosis and
treatment of babesiosis and anaplasmosis in cattle by livestock farmers in communal
areas of the central Eastern Cape Province, South Africa. Journal of South African
Veterinary Association 68: 40-44.
Masika, P.J., Van Averbeke, W., & Sonandi, A. (2000). Use of herbal remedies by small-scale
farmers to treat livestock diseases in central Eastern Cape Province, South Africa.
Journal of the South African Veterinary Association 71(2): 87-91.
103
Mathekaga, A.D.M., & Meyer, J.J.M. (1998). Antibacterial activity of South African
Helichrysum species. South African Journal of Botany 64: 293-295.
Mathews, H.B., Lucier, W.G., & Fisher, K.D. (1999). Medicinal herbs in the United States:
Research needs. Environmental Health Perspective 107: 773-778.
Mayatula, V., & Mavundla, T.R. (1997). A review on male circumcision procedures among
South African blacks. Curations. 20: 16-20.
McCutcheon, A.R., Ellis, S.M., Hancock, R.E.W., & Towers, G.H.N. (1994). Antifungal
screening of medicinal plants of British Columbia native peoples. Journal of
Ethnopharmacology 44, 157-169.
McFarland, J. (1907). The nephelometer: an instrument for estimating the number of bacteria in
suspensions for calculating the opsonic index and vaccines. Journal of the American
Medical Association 49: 1176.
McGaw, L.J., Jäger, A.K., Grace, O., Fennell, C., & Van Staden, J. (2005). Medicinal plants. In:
Van Niekerk, A. (Ed.), Ethics in Agriculture-Annal African Perspective. Springer,
Dordrecht, The Netherlands, 67-83.
McGaw, L.J., Jäger, A.K., & Van Staden, J. (1997). Prostaglandin inhibitory activity in Zulu,
Xhosa and Sotho medicinal plants. Phytotherapy Research 11: 113-117. In: Ashafa,
A.O.T., Grierson, D.S., & Afolayan, A.J. (2008). Antimicrobial activity of extracts from
Felicia muricata thunb. Journal of Biological Sciences 8(6): 1062-1066.
McGaw, L.J., Jäger, A.K., & Van Staden, J. (2000). Anti-bacterial, antihelmintic and antiamoebic activity in South African medicinal plants. Journal of Ethnopharmacology 72:
247-263.
McKenna, J. (1996). Alternatives to antibiotics. Cape Town: Stuik Publishers (Pty) Ltd, p.31 &
65-67.
McMillan, J., DeAngelis, C.D., & Feigin, R.D. et al., (Eds). (1999). Oski’s pediatrics: principles
and practice. (3rd ed). Philadelpia, P.A: Lippincott, Williams and Wilkins. In: Robinson,
104
D.T., Kumar, P., & Cadichon, S.B. (2008). Neonatal Sepsis in the Emergency
Department. Clinical Pediatric Emergency Medicine 9: 160-168.
Meissner, O. & Buso, D.L. (2007). Traditional male circumcision in the Eastern Cape – Scourge
or blessing? South African Medical Journal 97: 371-373.
Meurer-Grimes, B., Mcbeth D.L., Hallihan B., & Delph S. (1996). Antimicrobial activity in
medicinal plants of the Scrophulariaceae and Acanthaceae. International journal
pharmacognosy 34: 243-248.
Meyer, J.J.M., & Afolayan, A.J. (1995). Antibacterial activity of Helichrysum aureonitens
(Asteraceae). Journal of Ethnopharmacology 47: 109-111.
Meyer, J.M., Afolayan, A.J., Taylor, M.B., & Engelbrecht, L. (1996). Inhibition of Herpes
simplex virus type 1 by aqueous extracts from shoots of Helichrysum aureonites
(Asteraceae). Journal of Ethnopharmacology 52: 41-43.
Meyer, J.J.M., & Dilika, F. (1996). Antibacterial activity of Helichrysum pendunculatum used in
circumcision rites. Journal of Ethnopharmacology 53: 51-54.
Mitscher, L.A., Leu, R.P., Bathala, M.S., Wu, W.N., & Beal, J.L. (1972). Antimicrobial agents
from higher plants. Introduction, rationale and methodology. Lloydia 35: 157-166.
Mogotlane, S.M., Ntlangulela, J.T., & Ogunbanjo, B.G. (2004). Mortality and morbidity among
traditionally circumcised Xhosa boys in the Eastern Cape Province, South Africa.
Curations 27: 57-62.
Moolman, A.A. (1984). Die Gebruik van Inheemse Plante vir Medisinale doeleindes in
Somerset-Oos en Distrik. The Author, Pretoria.
Mortelmans, K., & Zeiger, E. (2000). The Ames Salmonella/microsome mutagenicity assay.
Mutation Research 455: 29-60.
Motsei, M.L., Lindsey, K.L., Van Staden, J., & Jager, A.K. (2003). Screening of traditionally
used South African plants for antifungal activity against Candida albicans. Journal of
Ethnopharmacology 86: 235-241.
105
Mozersky, R.P. (1999). Herbal products and supplemental nutrients used in the management of
diabetes. The Journal of the American Osteopathic Association 99: S4-S9.
Mukhtar, H., & Ahmad, N. (2000). Tea polyphenols: prevention of cancer and optimizing health.
The American Journal of Clinical Nutrition 71:1698S-1704S.
Mulholland, D.A. (2005). The future of ethnopharmacology: a Southern African perspective.
Journal of Ethnopharmacology 100: 124-126. In: Van Vuuren, S.F. (2008).
Antimicrobial activity of South African medicinal plants. Journal of Ethnopharmacology.
doi:10.1016/j.jep.2008.05.038
Munguti, K. (1997). Indigenous knowledge in the management of malaria and visceral
leishmaniasis among the Tugen of Kenya. Indigenous Knowledge and Development
Monitor 5: 10-12.
Naicker, K., Cukrowska, E., & McCarthy, T.S. (2003). Acid mine drainage arising from gold
mining activity in Johannesburg, South Africa and environs. Environmental Pollution
122, 29-40.
Nascimento, G.G.F., Locatelli, J., Freitas, P.C., & Silva, G.L. (2000). Antibacterial activity of
plant extracts and phytochemicals on antibiotic-resistant bacteria. Brazilian Journal
Microbiology 31: 247-256.
Naude, J.H. (2002). Reconstructive urology in the tropical and developing world: a personal
perspective. Brazilian Journal U int. 89: 31-6.
Navarro, V., Villarreal, M.L., Rojas, G., & Lozoya, X. (1996). Antimicrobial evaluation of some
plants used in Mexican traditional medicine for the treatment of infectious diseases.
Journal of Ethnopharmacology 53: 143-147.
Ndhlala, A.R., Amoo, S.O., Stafford, G.I., Finnie, J.F., & Van Staden, J. (2009). Antimicrobial,
anti-inflammatory and mutagenic investigation of the South African tree aloe (Aloe
barberae). Journal of Ethnopharmacology 124: 404-408.
Ndukwe, K.C., Lamikanra, A., & Okeke, I.N. (2004). Antibacterial activity of plants used as
chewing sticks in Africa. Drugs of the future 29: 1221-1233.
106
Newall, C.A., Anderson, L.A., & Phillipson, J.D. (1996). Herbal medicines: a guide for health
care professionals. London: The Pharmaceutical Press, p.1-296.
Nikaido, H., & Vaara, M. (1985). Molecular basis of bacterial outer membrane permeability.
Microbiological Reviews 49: 1-32.
Nishino, C., Enoki, N., Tawata, S., Morik, A., Kobayashi, K., & Fukushima, M. (1987).
Antibacterial activity of flavonoids against Staphylococcus epidermidis a skin bacterium.
Agric Biological Chemistry 51: 139-143.
Njenga, E., Van Vuuren, S.F., & Viljoen, A.M. (2005). Antimicrobial activity of Eriocephalus
species. South African Journal of Botany 71: 81-87.
Nostro, A., Germano, M.P., d’Angelo, V., Marino, A., & Cannatelli, M.A. (2000). Extraction
methods and bioautography for evaluation of medicinal plant activity. Letters in Applied
Microbiology 30: 379-384. In: Ncube, N.S., Afolayan, A.J., & Okoh, A.I. (2008).
Assessment techniques of antimicrobial properties of natural compounds of plant origin:
current methods and future trends. African Journal of Biotechnology 7(12): 1797-1806.
O’Brien, T.R., Calle, E.E., & Poole, W.K. (1995). Incidence of neonatal circumcision in Atlanta,
1985-1986. South Medicine Journal 88: 411-15.
Okoli, C.O., & Akah, P.A. (2004). Mechanisms of tha anti-inflammatory activity of the leaf
extracts of Culcasia scandens P. Beauv (Araceae). Pharmacology Biochemistry
Behaviour 79: 473-481. In: Ashafa, A.O.T., Grierson, D.S., & Afolayan, A.J. (2008).
Antimicrobial activity of extracts from Felicia muricata thunb. Journal of Biological
Sciences 8(6): 1062-1066.
Okonkwo, J.O., & Mothiba, M. (2005). Physico-chemical characteristics and pollution levels of
heavy metals in the rivers in Thohoyandou, South Africa. Journal of Hydrology 308:
122-127.
Osborn, E.M. (1943). Brit. J. Exp. Path. 24: 227, app.1-45. In: Watt, J.M., & Breyer-Brandwijk,
M.G. (1962). The Medicinal and Poisonous Plants of Southern and Eastern Africa. (2nd
ed). Edinburgh & London: E. & S. Livingstone Ltd, p. 45.
107
Otshudi, A.L., Vercruysee, A., & Foriers, A. (2000). Contribution to the ethnobotanical,
phytochemical and pharmacological studies of traditionally used medicinal plants in the
treatment of dysentery and diarrhoea in Lomela area, Democratic Republic of Congo
(DRC). Journal of Ethnopharmacology 71: 411-423.
Palmer, E., & Pitman, J. (1972). Trees of Southern Africa. Balkema, Cape Town.
Peltzer, K., Nqeketo, A., Petros, G., & Kanta, X. (2008). Traditional circumcision during
manhood initiation rituals in the Eastern Cape, South Africa: a pre-post intervention
evaluation. BioMed Central Public Health. 8: 64. (http://www.biomedcentral.com/14712458/8/64)
Penso, G. (1983). Index plantarum medicinalium totius mundi eurumque synonymorum.
Pentzia
incana
(Plant
name),
Retrieved
on:
31st
July,
2009
from
(www.fs.fed.us/.../weeds/iw_karoo_bush.shtml)
Phillipson, J.D. (1994). Natural products as drugs. Trans Royal Society Tropical Medicine
Hygiene 88:17-19.
Popat, A., Shear, N.H., Malkiewicz, I., Stewart, M.J., Steenkamp, V., Thomson, S., & Newman,
M.G. (2001). The toxicity of Callilepis laureola, a South African traditional herbal
medicine. Clinical Biochemistry 34: 229-236.
Puig, S. C., Garcia-Algar, O., & Vall, C. O. (2003). Childhood circumcision: review of the
evidence. Annal Paediatric (Barc) 59: 448-53.
Pujol, J. (1990). Naturafrica – The Herbalist Handbook. Natural Healers’ Foundation, Durban.
Pvt. Daniels, pers. comm. In: Van Wyk, B., & Gericke, N. (2000). People’s plants – A Guide to
Useful Plants of Southern Africa. (1st ed). Pretoria, [South Africa]: Briza Publications, p.
182.
Qin, G.W., & Xu, R.S. (1998). Recent advances on bioactive natural products from Chinese
medicinal plants. Medicine Res. Rev 6: 375-382.
108
Rabe, T., & Van Staden, J. (1997). Anti-bacterial activity of South African plants used for
medicinal purposes. Journal of Ethnopharmacology 56: 81-87.
Ramakrishnappa, K. (2002). Impact of cultivation and gathering of medicinal plants on
biodiversity: case studies from India. In: FAO (Ed.), Biodiversity and the Ecosystem
Approach in Agriculture, Forestry and Fisheries. Satellite Event on the Occasion of the
Ninth Regular Session of the Commission on Genetic Resources for food and
Agriculture, Rome.
Rasoanaivo, P., & Ratsimamanga-Urverg, S. (1993). Biological evaluation of plants with
reference to Malagasy flora. Monograph for the IFS-NAPRECA workshop on bioassays.
Antananarivo, Napreca, Madagascar.
Reich, E., & Schibli, A. (2006). High-Performance Thin-Layer Chromatography for the Analysis
of Medicinal Plants, Thieme, New York. In: Cieśla, L., & Waksmundzka-Hajnos, M.
(2009). Two-dimensional thin-layer chromatography in the analysis of secondary plant
metabolites. Journal of Chromatography A. 1216: 1035-1052.
Reid, K.A., Maes, A., Van Staden, J., De Kimpe, N., Mulholland, D.A., & Verschaeve, L.
(2006). Evaluation of the mutagenic and antimutagenic effects of South African plants.
Journal of Ethnopharmacology 106: 44-50.
Reid, R., & Robert, F. (2005). Pathology Illustrated. (6th ed.) Edinburgh: Elsevier Limited.
Reynecke, J.L. (1971). Towery by die Tswana met besondere verwysing na die KgatlaBagakgafela. PhD. Thesis University of Pretoria, South Africa.
Rhigozum obovatum (Plant name), by Harris, S. (2003). Frees State National Botanical Gardens.
Retrieved on 31st July, 2009 from www.plantzafrica.com/plantqrs/rhigozumob.htm.
Rios, J.L. & Villar, A. (1988). Screening methods for natural products with antimicrobial
activity: a review of the literature. Journal of Ethnopharmacology 23: 127-149. In:
Fennell, C.W., Lindsey, K.L., McGaw, L.J., Sparg, S.G., Stafford, G.I., Elgorashi, E.E.,
Grace, O.M., & van Staden, J. (2004). Assessing African medicinal plants for efficacy
and safety: pharmacological screening and toxicology. Journal of Ethnopharmacology
94: 205-217.
109
Roberts, M. (1990). Indigenous healing plants. (1st ed.). Halfway House, South Africa: Southern
Book Publishers.
Robinson, D.T., Kumar, P., & Cadichon, S.B. (2008). Neonatal Sepsis in the Emergency
Department. Clinical Pediatric Emergency Medicine 9: 160-168.
Rodriguez-Fragoso, L., Reyes-Esparza, J., Burchiel, S.W., Herrera-Ruiz, D., & Torres, E.
(2008). Risks and benefits of commonly used herbal medicines in Mexico. Toxicology
and Applied Pharmacology 227: 125-135.
Rojas, A., Hernandez, L., Pereda-Miranda, R., & Mata, R. (1992). Screening for antimicrobial
activity of crude drug extracts and pure natural products from Mexican medicinal plants.
Journal of Ethnopharmacology 35: 275-283.
Rojas, G., Lévaro, J., Tortoriello, J., & Navarro, V. (2001). Antimicrobial evaluation of certain
plants used in Mexican traditional medicine for the treatment of respiratory diseases.
Journal of Ethnopharmacology 74: 97-10.
Roychoudhury, A.N., & Starke, M.F. (2006). Partitioning and mobility of trace metals in the
Blesbokspruit: impact assessment of dewatering of mine waters in the East Rand, South
Africa. Applied Geochemistry 21: 1044-1063.
Rubin, R.H., Wolfson, J.S., Cosimi, A.B., & Tolkoff-Rubin, N.E. (1981). Infection in the renal
transplant recipient. The American Journal of Medicine 70: 405-411.
Samaranayake, L.P. (2000). Essential Microbiology for Dentistry; with a Contribution by B.M.
Jones; Foreword by Crispian Scully Edinburgh. Churchill Livingstone, New York.
Sanne, I. (2001). Treating HIV/AIDS. Archimedes 43: 32-34.
SATMERG,
(1999).
Retrieved
on
8th
March,
2008.
(http://www.sahealthinfo.org/traditionalmeds/aboutuwc.htm)
Scherrer, R., & Gerhardt, P. (1971). Molecular sieving by the Bacillus megaterium cell wall and
protoplast. Journal of Bacteriology 107: 718-735.
Schneider, A. (2002). Wild medicinal plants. (1st ed.). Toronto: Stackpole Books.
110
Scott, G., Springfield, E.P., & Coldrey, N. (2004). A Pharmacognostical study of 26 South
African plant species used as traditional medicines. Pharmaceutical Biology.42: 186-213.
Shale, T.L., Stirk, W.A., & Van Staden, J. (1999). Screening of medicinal plants used in Lesotho
for antibacterial and anti-inflammatory activity. Journal of Ethnopharmacology 67: 347354.
Shale, T.L., Stirk, W.A., & Van Staden, J. (2005). Variation in antibacterial and antiinflammatory activity of different growth forms of Malva parviflora and evidence for
synergism of the anti-inflammatory compounds. Journal of Ethnopharmacology 96: 325330.
Sherma, J., & Fried, B. (2005). Thin Layer Chromatographic Analysis of Biological Samples. A
Review. Journal of Liquid Chromatography and Related Technologies. Taylor & Francis,
Inc. 28: 2297-2314.
Silva, M.V., Costa, T.R., Costa, M.R., Ferrera, E.C., Fernandes, O.F.L., Santos, S.C., Liao, L.M.,
Ferri, P.H., Paula, J.R., Ferriera, H.D., & Silva, M.R.R. (2001). Growth inhibition effect
of Brazilian Cerrado plant extracts on Candida species. Pharmaceutical Biology 39: 138141.
Sim, T.R. (1907). The Forests and Forest Flora of the Cape of Good Hope. Aberdeen: Taylor &
Henderson. In: Watt, J.M., & Breyer-Brandwijk, M.G. (1962). The Medicinal and
Poisonous Plants of Southern and Eastern Africa. (2nd ed). Edinburgh & London: E. & S.
Livingstone Ltd, p. 254.
Sindambiwe, J.B., Calomme, M., Cos, P., Totté, J., Pieters, L., Vlietinck, A., & Vanden Berghe,
D. (1999). Screening of seven selected Rwandan medicinal plants for antimicrobial and
antiviral activities. Journal of Ethnopharmacology 65: 71-77.
Sindiga, I. (1994). Indigenous (medical) knowledge of the Maasai. Indigenous Knowledge and
Development Monitor 2: 16-18.
Skopek, T.R., Liber, H.L., Krolewski, J.J., & Thilly, W.G. (1978). Proc. National Academy
Science USA 75, 410.
111
Slusarenko, A.J., Longland, A.C., & Whitehead, I.M. (1989). A convenient, sensitive and rapid
assay for antibacterial activity of phytoalexins. Botanica Helychrysum 99: 203-207.
Snyman, T., Stewart, M.J., Grove, A., & Steenkamp, V. (2005). Adulteration of South African
traditional herbal remedies. Therapeutic Drug Monitoring 27: 86-89.
Sofowora, E.A. (1984). Medicinal Plants and Traditional Medicine in Africa. London: Willey.
Sokmen, A., Jones, B.M., & Erturk, M. (1999). The in vitro antibacterial activity of Turkish
medicinal plants. Journal of Ethnopharmacology 67: 79-86.
Springfield, E.P., Eagles, P.K.F., & Scott, G. (2005). Quality assessment of South African herbal
medicines by means of HPLC fingerprinting. Journal of Ethnopharmacology 101: 75-83.
Srinivasan, D., Nathan, S., Suresh, T., & Perumalsamy, P.L. (2001). Antimicrobial activity of
certain
Indian
medicinal
plants
used
in
folkloric
medicine.
Journal
of
Ethnopharmacology 74: 217-220.
Stafford, G.I., Jäger, A.K., & Van Staden, J. (2005). Effect of storage on the chemical
composition and biological activity of several popular South Afrcian Medicinal plants.
Journal of Ethnopharmacology 97: 107-115.
Steenkamp, V., Stewart, M., Curowska, E., & Zuckerman, M. (2002). A severe case of multiple
metal poisoning in a child treated with a traditional medicine. Forensic Science
International 128: 123-126.
Stermitz, F.R., Lorenz, P., Tawara, J.N., Zenewicz, L.A., & Lewis, K. (2000). Synergy in a
medicinal
plant:
Antimicrobial
action
of
berberine
potentiated
by
5’-
methoxyhydnocarpin, a multidrug pump inhibitor. Proc. National Academy Science
USA. 97(4): 1433-1437. In: Ncube, N.S., Afolayan, A.J., & Okoh, A.I. (2008).
Assessment techniques of antimicrobial properties of natural compounds of plant origin:
current methods and future trends. African Journal of Biotechnology 7: 1797-1806.
Stewart, M.J., Steenkamp, V., & Zuckerman, M. (1998). The toxicology of African herbal
medicines. Therapeutic Drug Monitoring 20: 510-516.
112
Stewart, M.J., Moar, J.J., Steenkamp, V., & Kokot, M. (1999). Findings in fatal cases of
poisoning attributed to traditional remedies in South Africa. Forensic Science
International 101: 177-183.
Tadmor, Y., Jefthas, E., Goliath, J., Smith, M., Langenhoven, P., Acquaye, D., Juliani, R.,
Letchamo, W., Renaud, E., Zimba, N., Raskin, I., Brown, J., & Simon, J.E. (2002).
Quality assurance and quality control for African natural plant products from the ground
up. In: Janick, J., Whipkey, A.(Eds.), Trends in New Crops and New Uses. ASHS Press,
Alexandria, VA, p.93-97.
Talaro, K., & Talaro, A. (1996). Foundations in Microbiology. Basic Principles.(1st ed.) Wm. C.
Brown Publishers.
Tanaka, J.C.A., da Silva, C.C., de Oliveira, A.J.B., Nakamura, C.V., & Dias Filho, B.P. (2006).
Antibacterial activity of indole alkaloids from Aspidosperma ramiflorum. Brazilian
Journal of Medical Biology Research 39(3): 387-391.
Taylor, J.L.S., Rabe, T., McGaw, L.J., Jäger, A.K., & Van Staden, J. (2001). Towards the
scientific validation of traditional medicinal plants. Plant Growth Regulation 34: 23-37.
In: Ncube, N.S., Afolayan, A.J., & Okoh, A.I. (2008). Assessment techniques of
antimicrobial properties of natural compounds of plant origin: current methods and future
trends. African Journal of Biotechnology 7: 1797-1806.
Taylor, J.L.S., & Van Staden, J. (2001). The effect of age, season and growth conditions on antiinflammatory activity in Eucomis autumnalis (Mill) Chitt. Plant extracts. Plant Growth
Regulation 34: 39-47.
Tetta, C., Bellomo, R., & Ronco, C. (2003a). Artificial Organ Treatment for Multiple Organ
Failure, Acute Renal Failure, and Sepsis: Recent New Trends. International Society for
Artificial Organs. Vol. 27 (3): 202.
Tetta, C., Bellomo, R., D’Intini, V., De Nitti, C., Inguaggiato, P., Brendolan, A., & Ronco, C.
(2003b). Do circulating cytokines really matter in sepsis? International Society of
Nephrology [Kidney International], 63, Supplement 84, 69-71.
113
Thring, T.S.A., Springfield, E.P., & Weitz, F.M. (2007). Antimicrobial activities of four plant
species from the Southern Overberg region of South Africa. African Journal of
Biotechnology 6(15): 1779-1784.
Tortora, G.F., Funke, B.R., & Case, C.L. (1994). Microbiology. An introduction . (1st ed.) The
Benjamin/Cummings Publishing Company, Inc.
Trankina, M.L. (1998). Drugs that grow on trees. World and I 13(8): 158-166.
Tsao, R., Romanchuck, F.E., Peterson, C.J., & Coats, J.R. (2002). Plant growth regulatory effect
and insecticidal activity of the extracts of the Tree of Heaven (Ailanthus altissima L.).
Biomedical Central Ltd. Available: http://www.biomedcentral.com/1472-6785/2/1.
Retrieved on 31st July, 2009.
Valsaraj, R., Pushpangadan, P., Smitt, U.W., Adsersen, A., & Nyman, U. (1997). Antimicrobial
screening of selected medicinal plants from India. Journal of Ethnopharmacology 58: 7583.
Van Vuuren, S.F. (2008). Antimicrobial activity of South African medicinal plants. Journal of
Ethnopharmacology. doi:10.1016/j.jep.2008.05.038.
Van Wyk, B.-E., Van Oudtshoorn, B., & Gericke, N. (1997). Medicinal Plants of South Africa.
Pretoria: Briza Publications.
Van Wyk, B.E., & Gericke, N. (2000). People’s plants: A guide to useful plants of Southern
Africa. (1st ed.). Pretoria, South Africa: Briza Publications.
Van Wyk, L., & Els, I. (2008). Neonatal cholinergic syndrome-organophosphate poisoning or
herbal medicine intoxication? South African Journal of Child Health 2: 26-27.
Verschaeve, L., Kestens, V., Taylor, J.L.S., Elgorashi, E.E., Maes, A., Van Puyvelde, L., De
Kimpe, N., & Van Staden, J. (2004). Investigation of the antimutagenic effects of
selected South African medicinal plant extracts. Toxicology in vitro 18: 29-35.
Verschaeve, L., & Van Staden, J. (2008). Mutagenic and antimutagenic properties of extracts
from South African traditional medicinal plants. Journal of Ethnopharmacology 119:
575-587.
114
Verster, E., Du Plessis, W., Schloms, B.H.A., & Fuggle, R.F. (1992). Soil. In: Fuggle, R.F.,
Rabie, M.A.(Eds.). Environmental Management in South Africa. Cape Town: Juta & Co.
Ltd., p. 181-211.
Viljoen, A.M., Subramoney, S., Van Vuuren, S.F., Baser, K.H.C., & Demirci, B. (2004). The
composition, geographical variation and antimicrobial activity of Lippia javanica
(Verbenaceae) leaf essential oils. Journal of Ethnopharmacology 96: 271-277.
Voet, D., & Voet, J.G. (1995). Biochemistry. (2nd ed). Somerset: John Willey and Sons, INC.
Voet, D., & Voet, J.G. (2004). Biochemistry. (3rd ed). United States of America: John Willey and
Sons, INC.
Von Ahlefeldt, D., Crouch, N.R., Nicholas, G., Symonds, R., Mckean, S., Sibiya, H., & Cele,
M.P. (2003). Medicinal Plants traded on South Africa’s Eastern Seaboard. Durban:
Porcupine Press.
Wallace, J.R. (2004). Antimicrobial properties of plant secondary metabolites. Proc. Nutritional
Society 63: 621-629.
Wall, M.E., Wani, M.C., Hughes, T.J., & Taylor, H.J. (1988). Natural Products 51: 866.
Walsh, G. (1998). Biopharmaceuticals: Biochemistry and Biotechnology. Chichester, England:
John Willey and Sons Ltd.
Walsh, T.J., & Groll, A.H. (1999). Emerging fungal pathogens: evolving challenges to
immunocompromised patients for the twenty-first century. Transplant Infectious Disease
1: 247-261.
Watt, J.M., & Breyer-Brandwijk, M.G. (1962). The medicinal and poisonous plants of Southern
and Eastern Africa. (2nd ed.). London: Livingstone.
Wayne, B.J. (1998). Alternative medicines- Learning from the past, examining the present,
advancing to the future. Journal of American Medicine Association 280: 1616-1618.
Wenzel, R.P. (2002). Treating sepsis. New England Journal of Medicine 347: 966-968. In:
Tetta, C., Bellomo, R., D’Intini, V., De Nitti, C., Inguaggiato, P., Brendolan, A., &
115
Ronco, C. (2003). Do circulating cytokines really matter in sepsis? International Society
of Nephrology [Kidney International], Vol. 63, Supplement 84, 69-71.
White, L.B., & Foster, S. (2000). Kruie in die Apteek, pp. Jacklin Uitgewers, Parklands.
Whitten, G. (1997). Herbal Harvest-Commercial Organic Production of Quality and Dried herbs,
(2nd ed). Australia: Bloomingham Books.
WHO, (1998). Regulatory Situation of Herbal Medicines: A Worldwide Review. World Health
Organization, Geneva.
WHO, (2003). Guidelines on Good Agricultural and Collection Practices (GACP) for Medicinal
Plants, Geneva.
WHO,
(2006).
Traditional
Medicine.
Retrieved
on
18th
August,
2009
from
on
18th
August,
2009
from
www.who.int/mediacentre/factsheets/fs134/en/.
WHO,
(2008).
Traditional
medicine.
Retrieved
www.who.int/mediacentre/factsheets/fs134/en/.
WHO, (2009). WHO launches the first global strategy on traditional and alternative medicine.
Retrieved
on
18th
August,
2009
from
www.who.int/mediacentre/news/releases/release38/en/
Wilkinson, G.B. (1997). Circumcision: one of the oldest known surgical procedures. Urol Nurs
17: 125-6.
Williams, C.O. (1930). Un. South African Department Agricultural Science Bull. 74. In: Watt,
J.M., & Breyer-Brandwijk, M.G. (1962). The Medicinal and Poisonous Plants of
Southern and Eastern Africa. (2nd ed). Edinburgh & London: E. & S. Livingstone Ltd, p.
45.
Winston, D.J., Emmanouilides, C., & Busuttil, R.W. (1995). Infection in liver transplant
recipients. Clinical Infectious Diseases 21: 1077.
Wiswell, T.E., & Geschke, D.W. (1989). Risks from circumcision during the first month of life
compared with those of uncircumcised boys. Pediatrics 83: 1011-15.
116
Wohlmuth, H., Oliver, C., & Nathan, P. (2003). Australian Sales of Herbal Medicine. Journal of
Herbal Pharmacotherapy, Vol. 2(2): 33-46.
Wolfender, J.L. (1993). Search for bitter principles in chironia species by LC-MS and isolation
of a new secoiridoid diglycoside from Chironia krebsii. Journal of National Product 56:
682-689. In: Van Wyk, B.E., Van Oudtshoorn, B., & Gericke, N. (1997). Medicinal
Plants of South Africa. (1st ed). Pretoria: Briza Publications.
Xu, H.X., & Lee, S. (2001). Activity of plant flavonoids against antibiotics resistant bacteria.
Phytotherapy Research 15: 39-43.
Yao, J., & Moellering, R. (1995). Antibacterial agents: Manual of Clinical Microbiology. ASM:
Washington DC, p.1281-1290.
Yee, S.-K., Chu, S.S., Xu, Y,-M., & Choo, P.L. (2005). Regulatory control of Chinese
proprietary medicines in Singapore. Health Policy 71: 133-149.
Yffa, B.T.S., Lindsey, K.L., Taylor, M.B., Erasmus, D.G., & Jäger, A.K. (2002). The
pharmacological screening of Pentanisia prunelloides and the isolation of the
antibacterial compounds palmitic acid. Journal of Ethnopharmacology 79: 101-107.
Yousef, P. & Tawill, G. (1990). Antimicrobial activity of volatile oils. Pharmazie 35: 698-701.
Zeiger, E. (2001). Mutagens that are not carcinogenic: faulty theory or faulty tests? Mutation
Research 492: 29-38.
Zhang, X. (1996). Regulation and registration of herbal medicines. Presented at the 32nd annual
meeting, self-medication in Europe --enlarging the horizon. European proprietary.
Zschocke, S., & Van Staden, J. (2000). Cryptocarya species-substitute plants for Ocotea bullata?
A pharmacological investigation in terms of cyclooxygenase-1 and -2 inhibition. Journal
of Ethnopharmacology 71: 473-478.
117