Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
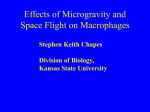
Biochem. J. (2012) 442, 253–262 (Printed in Great Britain) 253 doi:10.1042/BJ20111708 REVIEW ARTICLE Role and function of macrophages in the metabolic syndrome Prerna BHARGAVA and Chih-Hao LEE1 Department of Genetics and Complex Diseases, Department of Nutrition, Division of Biological Sciences, Harvard School of Public Health, 665 Huntington Ave, Boston, MA 02115, U.S.A. Macrophages are key innate immune effector cells best known for their role as professional phagocytes, which also include neutrophils and dendritic cells. Recent evidence indicates that macrophages are also key players in metabolic homoeostasis. Macrophages can be found in many tissues, where they respond to metabolic cues and produce pro- and/or antiinflammatory mediators to modulate metabolite programmes. Certain metabolites, such as fatty acids, ceramides and cholesterol crystals, elicit inflammatory responses through pathogensensing signalling pathways, implicating a maladaptation of macrophages and the innate immune system to elevated metabolic stress associated with overnutrition in modern societies. The outcome of this maladaptation is a feedforward inflammatory response leading to a state of unresolved inflammation and a collection of metabolic pathologies, including insulin resistance, fatty liver, atherosclerosis and dyslipidaemia. The present review summarizes what is known about the contributions of macrophages to metabolic diseases and the signalling pathways that are involved in metabolic stress-induced macrophage activation. Understanding the role of macrophages in these processes will help us to develop therapies against detrimental effects of the metabolic syndrome. INTRODUCTION system, especially macrophages, to respond in a deleterious manner, in which a resolution state could not be achieved [7,8]. At around the same time as these studies were occurring, researchers observed that insulin resistance and hyperglycaemia led to dysregulated immune responses and increased incidences of infection in patients with the metabolic syndrome [9–16]. Together, it has become evident that metabolic pathways are tightly intertwined with inflammatory signalling and immune responses. As environmental sentries, it is not surprising that macrophages sense and regulate metabolism. This link between macrophages and metabolic regulation was strengthened further with the discovery of resident macrophage populations in metabolically active tissues, such as WAT (white adipose tissue) and liver [17,18]. The interplay between resident macrophages and pathologies associated with the metabolic syndrome has been studied extensively since. In the present review, we highlight major contributions of macrophages to the metabolic milieu and describe how the functions of macrophages are altered during states of metabolic dysfunction. We begin with a brief overview of the recruitment of macrophages in various metabolic tissues and the diseases associated with their activation. We then discuss some proposed mechanisms for the inflammatory pathways that lead to pathologies, with an emphasis on insulin resistance/Type 2 diabetes. The innate immune system, which consists of macrophages, dendritic cells and a variety of other effector cells, has evolved as a formidable defence against external threats to the human host. When first described by Élie Metchnikoff in the late 1800s, macrophages were thought to primarily function as phagocytes. In the next several decades, intense effort went into understanding the mechanisms that led to macrophage activation. It was not until about 100 years later that researchers first started to document the innumerable roles that macrophages play [1]. We now know that macrophages are found throughout the body and are involved in tissue homoeostasis, wound healing, general surveillance of host threats and, as was first observed, killing of foreign pathogens. Abundant sources of food that have high energy content and are enriched in saturated fats, coupled with a lack of physical activity, are responsible for the sharp increase in a collection of pathologies, such as obesity, hepatosteatosis, insulin resistance and atherosclerosis, known as the metabolic syndrome. All of these pathologies increase the chance of developing cardiovascular disease, diabetes mellitus and premature death [2]. The observation that anti-inflammatory salicylates could improve insulin sensitivity and glucose responsiveness gave the first indication that metabolic syndrome is associated with lowgrade chronic inflammation [3]. This was followed by reports that inflammatory cytokines, such as TNFα (tumour necrosis factor α), inhibit insulin responsiveness in adipocytes, providing a link between inflammation and metabolic pathways [4–6]. Subsequent studies have suggested that lipid overload triggers the immune Key words: inflammatory signalling, insulin resistance, macrophage activation, metabolic disease, metabolic syndrome, white adipose tissue inflammation. AN ESSENTIAL ROLE FOR MACROPHAGES IN METABOLIC PATHOLOGIES Resident macrophages in different tissues adapt to their local microenvironment and exhibit diverse functional and Abbreviations used: ASC, apoptosis-associated speck-like protein containing a caspase-recruitment domain; ATM, adipose-tissue-resident macrophage; BAT, brown adipose tissue; CCR2, CC chemokine receptor 2; CHOP, C/EBP (CCAAT/enhancer-binding protein)-homologous protein; DHA, docosahexaenoic acid; EPA, eicosapentaenoic acid; ER, endoplasmic reticulum; GPCR, G-protein-coupled receptor; HIF, hypoxia-inducible factor; IFNγ, interferon γ; IKK, inhibitor of nuclear factor κB kinase; IL, interleukin; IRS-1, insulin receptor substrate-1; JNK, c-Jun N-terminal kinase; LDL, low-density lipoprotein; Ldlr, LDL receptor; LXR, liver X receptor; MCP-1, monocyte chemoattractant protein 1; miRNA, microRNA; mTOR, mammalian target of rapamycin; NAFLD, non-alcoholic fatty liver disease; NF-κB, nuclear factor κB; NLRP3, NLR (nucleotide-binding-domain- and leucine-rich-repeatcontaining) family, pyrin-domain-containing 3; oxLDL, oxidized LDL; PKR, double-stranded RNA-dependent protein kinase; PPAR, peroxisome-proliferatoractivated receptor; STAT6, signal transducer and activator of transcription 6; SVF, stromal vascular fraction; TLR, Toll-like receptor; TNFα, tumour necrosis factor α; UPR, unfolded protein response; WAT, white adipose tissue. 1 To whom correspondence should be addressed (email [email protected]). c The Authors Journal compilation c 2012 Biochemical Society 254 P. Bhargava and C.-H. Lee signalling molecules in metabolic diseases. Earlier studies have demonstrated that MCP-1- and CCR2-knockout mice are protected from atherosclerosis [19–21]. CCR2-knockout mice also display attenuated macrophage accumulation and chronic inflammation in adipose tissue [22]. In addition, mice lacking MCP-1 or expressing a dominant-negative form of MCP-1 show improved insulin sensitivity [23], whereas transgenic MCP-1 overexpression in adipose tissue causes insulin resistance and hepatic steatosis [23,24]. Other chemokines, such as osteopontin, angiopoietin-like protein 2 and CXCL14 (CXC chemokine ligand 14) have also been shown to play a role in obesity-induced macrophage recruitment [25–28]. These studies demonstrate that macrophage infiltration is an essential step for metabolic disease pathogenesis. Activation Figure 1 Metabolic dysregulation leads to a feedforward cycle of chronic inflammation Activation of inflammatory pathways by metabolic stress leads to macrophage recruitment to sites of affected tissues, such as vasculature, WAT, muscle and liver. There, they pick up excess lipids and cell debris in an attempt to restore homoeostasis. The presence of persistent pro-inflammatory stimulants (e.g. fatty acids and cholesterol) causes macrophage dysfunction, including defective efferocytosis and unresolved inflammation, resulting in recruitment and activation of more macrophages. In WAT, infiltrated macrophages are concentrated around the dying fat cells, known as the crown-like structure. In the vasculature, macrophages are enriched in areas of fatty streaks. Inflammatory cytokines produced by activated macrophages induce insulin resistance in major metabolic tissues, promote hepatosteatosis and facilitate foam cell and plaque formation in the vessel wall. morphological phenotypes. Resident populations, such as Kupffer cells in the liver, resident macrophages in WAT and alveolar macrophages in the lung, show expression profiles distinct from those of recruited macrophages responding to systemic cues [1]. For example, studies have demonstrated that ATMs (adipose-tissue-resident macrophages) are functionally distinct from infiltrating macrophages (discussed below). In the process of understanding the aetiology of the metabolic syndrome, we have begun to understand the general mechanisms underlying metabolic diseases, particularly the roles of macrophages in atherosclerosis and in adipose tissue insulin resistance. Owing to a lack of specific markers for resident and recruited macrophages and the cross-talk between tissues in the progression of metabolic diseases, it is often difficult to tease apart the precise contribution of individual macrophage populations to the onset and development of systemic metabolic dysfunction. Nonetheless, it is clear that the interaction between macrophages and metabolic cells plays a key role in disease pathogenesis. Macrophages are recruited by pro-inflammatory cytokines and chemokines to deal with lipid overload-induced tissue dysfunction and are also subject to the detrimental effect of lipid influx. As such, metabolic stress initiates a feedforward cycle of inflammatory responses, resulting in a state of unresolved chronic inflammation, with macrophages as major culprits contributing to metabolic diseases (Figure 1). Macrophage infiltration and activation Recruitment The production of chemokines, the factors that recruit immune cells to sites of trouble, is increased in states of metabolic dysfunction. MCP-1 (monocyte chemoattractant protein 1) [also known as CCL2 (CC chemokine ligand 2)] and its receptor CCR2 (CC chemokine receptor 2) are the most studied chemokine c The Authors Journal compilation c 2012 Biochemical Society Macrophages respond to many different types of foreign and host-derived stimuli and exhibit very precise and co-ordinated activation states according to the signals they receive. These states lie on a spectrum ranging from the pro-inflammatory state to the anti-inflammatory state [29] (Figure 2). Foreign pathogens or Th1 cytokines [e.g. TNFα, IL (interleukin)-1β and IFNγ (interferon γ )] transduce signals that activate macrophages to a proinflammatory phenotype, typically referred to as an M1 response, characterized by the expression of inflammatory markers, such as TNFα, IFNγ and iNOS (inducible nitric oxide synthase) [29]. In contrast, M2 macrophages, induced by Th2 cytokines IL-4 and IL-13, produce anti-inflammatory mediators, notably IL-10 [29]. As discussed below, the M1/M2 paradigm also applies to metabolic regulation, with M1 inducing and M2 preventing metabolic diseases respectively (Figure 3). Interestingly, dietary fatty acids are able to polarize macrophages towards M1 or M2 activation states, depending on the signalling molecules with which they interact (Figure 2), thus providing a molecular basis for the cross-talk between metabolic and inflammatory pathways. Resolution/deactivation The initial pro-inflammatory response is terminated by antiinflammatory cytokines, such as IL-10, which is induced by both M1 and M2 cytokines to deactivate macrophages and promote resolution [30–33]. Lack of this termination signal leads to persistent establishment of the inflammatory response [34–36]. Epidemiological studies have shown that polymorphisms in the IL10 gene are associated with obesity and metabolic diseases [37– 39]. Furthermore, in patients with Type 2 diabetes, circulating monocytes express decreased levels of IL-10 [40]. IL-10 and other deactivating signalling molecules are also induced during efferocytosis, a process by which macrophages engulf and clear apoptotic cells in an effort to prevent necrosis and suppress inflammation [41]. This process is thought to help remove oxidized lipids and cholesterol and to activate Akt and NF-κB (nuclear factor κB) survival pathways [42]. Several studies have shown that efficient efferocytosis is necessary to inhibit necrotic plaque formation and defects in efferocytosis lead to the formation of unstable lesions and an increase in systemic inflammation [43– 46]. Faulty efferocytosis has also been observed in diabetic mouse models and is thought to promote inflammatory signalling [47]. Oxidative stress and macrophage insulin resistance are two of the potential mechanisms that cause defective efferocytosis [41,48]. Therefore the combined effects of persistent pro-inflammatory stimulation from increased lipid influx, decreased deactivating signals and compromised efferocytosis lead to the unresolved inflammation in metabolic dysregulation. Role and function of macrophages in the metabolic syndrome Figure 2 255 Dietary lipids and inflammatory mediators share common signalling pathways in the control of macrophage activation The Th2 (M2) type response, elicited by Th2 cytokines, notably IL-4 and IL-13, and parasitic worm infection, induces an anti-inflammatory phenotype in the macrophage and promotes metabolic homoeostasis, tissue repair, wound healing and angiogenesis. STAT6 is activated by Th2 cytokines to control the expression of PPARδ and PPARγ . Together, they regulate mitochondrial oxidative metabolism and macrophage alternative activation. The ω − 3 fatty acids DHA and EPA are known to ligate the GPCR GPR120 to promote anti-inflammatory response. These fatty acids can also mediate PPAR activation. In contrast, saturated fatty acids (FAs), ceramides (metabolites of fatty acids) and cholesterol crystal can induce pro-inflammatory activation of the macrophage through pathogen-sensing proteins TLR2/TLR4, which activate the JNK cascade, leading to NF-κB relocation to the nucleus and induction of inflammatory cytokines and glycolytic pathways. Excess lipids have also been shown to induce ER stress and inflammasome activation. Pro-inflammatory cytokines produced by these macrophages, including TNFα and IL-1β, cause tissue damage and inhibit insulin signalling, which contribute to the pathogenesis of metabolic diseases. IκB, inhibitor of NF-κB; iNOS, inducible nitric oxide synthase. Figure 3 Cross-talk between macrophages and adipocytes plays an important role in adipose tissue homoeostasis In the physiological state, ATMs exhibit an M2 phenotype, mediated by the Th2 cytokines IL-4 and IL-13, and downstream transcription factors STAT6 and PPARδ/PPARγ . Several cell types within WAT have been reported to be the sources of Th2 cytokines, including T-lymphocytes, eosinophils and adipocytes. ω − 3 fatty acids (FAs) are also able to induce an anti-inflammatory response through GPR120 and possibly PPARs. IL-10 is one of the well-characterized anti-inflammatory cytokines produced by these macrophages. In obesity, stressed adipocytes produce inflammatory mediators (e.g. MCP-1, TNFα and saturated fatty acids) to induce M1 activation through inflammatory transcription factors, such as NF-κB. Macrophages respond by up-regulating inflammatory cytokines, which activate JNK and inhibit insulin signalling pathways in the adipocyte. Macrophages and metabolic pathologies Macrophage infiltration and adipose tissue insulin resistance The SVF (stromal vascular fraction) of WAT has been studied extensively in the progression of obesity-induced insulin resistance. Adipose tissues from lean animals and humans contain a resident macrophage population exhibiting the M2 phenotype [49] (Figure 3). In contrast, the obese state is characterized by infiltration of M1 macrophages that accumulate around apoptotic fat cells (referred to as crown-like structures) and express the CD11c marker [49]. It has been suggested that macrophages are recruited in response to adipocyte hypertrophy or to signals from dying adipocytes in an attempt to restore homoeostasis [50–52]. There they can be activated further by non-esterified c The Authors Journal compilation c 2012 Biochemical Society 256 P. Bhargava and C.-H. Lee fatty acids released by dysfunctional fat cells (discussed below), thus amplifying the inflammatory response. These macrophages contain lipid droplets derived from direct lipid intake or ingestion of dead fat cells and account for up to 40 % of the SVF in severe cases of obesity [22]. They secrete pro-inflammatory factors, such as MCP-1, TNFα and IL-6, which both amplify inflammatory responses and inhibit adipocyte insulin signalling [17,18]. Similarly, monocytes from Type 2 diabetic patients or obese individuals express more M1 markers [40]. Conditional depletion of CD11c-expressing macrophages or inhibition of macrophage recruitment (e.g. MCP-1 knockout) in obese mice resulted in a significant reduction in systemic inflammation and an improvement in insulin sensitivity [23,24,53]. It should also be noted that adipocytes also produce inflammatory mediators. Because of similarities between adipocytes and macrophages, the source of the pro-inflammatory cytokines/chemokines within WAT is obscured. In contrast with WAT, macrophage infiltration into BAT (brown adipose tissue) seems to be limited and, as such, the role of macrophages in BAT is unclear [54,55]. Vascular inflammation and atherosclerosis The most well-characterized macrophage population in the metabolic syndrome is that of macrophages recruited to sites of endothelial dysfunction in atherosclerosis [56,57]. Elevated LDL (low-density lipoprotein)/cholesterol levels result in accumulation of LDL particles in the subendothelial matrix. Careful analyses of temporal changes leading to lesion formation revealed that this lipid deposition is the crucial initiating event in macrophage recruitment [57]; the accumulated LDL becomes oxidized (oxLDL) and locally produced cytokines and chemokines, in response to oxLDL, recruit monocytes/macrophages into the subendothelial space. Lipid particles are taken up by macrophages through specialized receptors SR-A (scavenger receptor A) and CD36, among other mechanisms [58]. These processes evoke a characteristic inflammatory response by releasing inflammatory molecules, such as MCP-1, to the ECM (extracellular matrix), which recruit more macrophages. The lipid-laden macrophages become foam cells and undergo necrotic cell death releasing intracellular components leading to a vicious cycle of chronic inflammation [36]. Subsequently, smooth muscle cells migrate to the lesion in response to inflammatory mediators and contribute to fibrotic plaque formation and rupture [57]. Hepatosteatosis Liver insulin resistance and hepatic steatosis, referred to as NAFLDs (non-alcoholic fatty liver diseases), are major components of the metabolic syndrome. Lipidomic analyses of liver tissue during various stages of NAFLD show a strong correlation between abnormal fat composition and disease pathogenesis [59], with excess fat accumulation leading to the recruitment of inflammatory cells [60]. Together with Kupffer cells, these immune cells are responsible for the development of hepatic inflammation in both humans and various animal models. Studies have shown that depletion of Kupffer cells or inhibition of pro-inflammatory mediators protect against the development of NAFLD [61–63]. During high-fat-diet treatment, depletion of Kupffer cells by GdCl3 or clodronate-encapsulated liposomes has been shown to improve insulin sensitivity and glucose tolerance [64–66]. A single dose of GdCl3 in mice on normal chow enhances insulin signalling and reduces glucose production in the liver [65]. In contrast, macrophage-specific Ppard − / − (peroxisome-proliferator-activated receptor δ) mice, whose macrophages/Kupffer cells exhibit a predominantly M1 phenotype, develop insulin resistance and hepatic steatosis [67]. c The Authors Journal compilation c 2012 Biochemical Society Muscle dysfunction The resident macrophage population in muscle has not been characterized. Macrophages do, however, play a significant role in muscle repair during exercise and tissue damage [68]. Studies have shown that macrophages infiltrate fat depots formed around the muscle in obesity [17]. Additionally, muscle can be affected by inflammatory cytokines from other tissues, such as liver and adipose tissue, even though it may not be a site of significant production of inflammatory mediators [69]. INFLAMMATORY SIGNALLING AND METABOLIC DISEASES Although the role of inflammation in atherogenesis is well documented [36,56,57], the underlying mechanisms through which pro-inflammatory signalling pathways cause insulin resistance are still under investigation. One of the better-defined mechanisms is through JNK (c-Jun N-terminal kinase) activation, which phosphorylates IRS-1 (insulin receptor substrate-1) to block insulin signal transduction [7,70]. Similarly, our knowledge regarding how anti-inflammatory pathways improve metabolic homoeostasis is limited, apart from their ability to antagonize M1 activation [71]. In this section, we summarize various signalling pathways mediating macrophage activation during the pathogenesis of the metabolic syndrome. Pro-inflammatory signalling JNK and pro-inflammatory cytokines JNK is an important regulatory node for inflammatory mediators, including pro-inflammatory cytokines, TLRs (Toll-like receptors) and ER (endoplasmic reticulum) stress (Figure 2). In obesityinduced insulin resistance and hepatic steatosis, deletion of JNK1 in the haemopoietic compartment by bone marrow transplantation is beneficial [72]. TNFα was one of the first pro-inflammatory cytokines to be linked to JNK activation [4,70]. TNFα-receptor-knockout mice show improved metabolic homoeostasis and insulin sensitivity fed on both normal chow and a high-fat diet [73]. Additionally, Tnf + / + bone marrow donated to a Tnf − / − mouse induces insulin resistance in an otherwise insulin-sensitive mouse [74]. Recently, PKR (doublestranded RNA-dependent protein kinase), which senses viral infection, was shown to interact with JNK and IRS-1 [75]. Interestingly, PKR is able to phosphorylate IRS-1 directly, suggesting that JNK integrates different inflammatory signals through a multicomponent inflammatory complex. TLRs and NF-κB TLRs are pattern-recognition receptors that respond to pathogenic antigens and propagate inflammatory signalling [76]. In vitro, non-esterified fatty acids (saturated fatty acids, e.g. palmitic acid) or ceramides can signal through TLR2 and TLR4 on macrophages and induce pro-inflammatory gene expression [77–79]. In vivo, whole-body TLR4 deletion improves insulin sensitivity in a lipidinfusion model of transient insulin resistance. Similarly, TLR4 loss-of-function mutation or TLR2 deficiency protects against diet-induced obesity and insulin resistance [80–82]. However, TLR2 and TLR4 are expressed on most tissue types including adipocytes and hepatocytes, in addition to immune cells. The contribution of macrophage TLR4 was examined through haemopoietic cell-specific TLR4 deletion, which ameliorates high-fatdiet-induced hepatic and adipose tissue insulin resistance [83]. Role and function of macrophages in the metabolic syndrome TLR4 ligation promotes IKK (inhibitor of NF-κB kinase) activation, followed by phosphorylation and nuclear translocation of NF-κB to activate inflammatory gene transcription. Systemic deletions of NF-κB or various IKK isoforms (e.g. IKKβ and IKKε) prevent obesity-induced insulin resistance [36,84,85]. Myeloid-specific IKKβ deletion also leads to improved systemic insulin sensitivity, increased glucose disposal and suppressed hepatic glucose production [84]. In line with these observations, salicylate treatment, known to attenuate NF-κB activation, increases insulin sensitivity in humans [86–88]. In the setting of atherosclerosis, many studies have demonstrated that a complete deletion of various TLR family members reduces the lesion size in Ldlr − / − (low-densitylipoprotein receptor) or Apoe − / − (apolipoprotein E) mice [89,90]. Ldlr − / − mice transplanted with Tlr2 − / − bone marrow are protected from atherosclerosis [89]. Similarly, Ldlr − / − mice deficient in myeloid-specific NF-κB subunit p50 have decreased atherosclerotic lesions [91]. Lesions in these animals exhibit near complete loss of foam cells, supporting previous findings that NF-κB regulates genes involved in lipid uptake and foam cell formation [92]. 257 has been shown that the ER stress in the macrophage is caused by increased aP2 (adipocyte protein 2) lipid chaperone activity, which promotes atherogenesis [109]. Hypoxia Activation of macrophages to a pro-inflammatory state increases glucose influx for glycolysis, which is controlled by HIF (hypoxia-inducible factor)-1α [110–113]. Loss of HIF-1α in the macrophage leads to decreased pro-inflammatory cytokine production, whereas deletion of VHL (von Hippel–Lindau tumour-suppressor protein), a repressor of HIF-1α, results in chronic activation of HIF-1α and uncontrolled inflammation [112,114]. In the context of metabolic dysregulation, adipose tissues in obese mice are hypoxic, which may cause macrophage HIF-1α activation [51,52,115,116]. Systemic hypoxia has been shown to induce insulin resistance and NAFLD [51,117,118]. Furthermore, high levels of hypoxia during adipose expansion may lead to necrotic death of both adipocytes and macrophages, since HIF-1α activation blocks physiological apoptotic cell death [52,116,119]. Similarly, hypoxia promotes macrophage necrosis in mouse models of atherosclerosis [119–121]. Inflammasome The NLRP3 [NLR (nucleotide-binding-domain- and leucinerich-repeat-containing) family, pyrin-domain-containing 3] inflammasome senses endogenous danger signals and generates the mature secreted forms of IL-1β and IL-18 through caspase 1 activation [93–96]. In vitro, palmitic acid and ceramide are able to induce IL-1β and caspase 1 processing in the macrophage [97]. Mice deficient in NLRP3 or ASC (apoptosis-associated specklike protein containing a caspase-recruitment domain, an adaptor protein of the NLRP3 inflammasome) exhibit increased insulin sensitivity in liver, WAT and muscle [97–99]. In addition, caspase 1 and IL-1β have been shown to mediate inflammasome-induced insulin resistance [98]. Along these lines, lack of IL-1R, the receptor for IL-1β, confers protection against insulin resistance induced by a high-fat diet [100]. Inflammasome activation can also be detected in atherosclerotic lesions [101,102]. Cultured macrophages exposed to crystalline cholesterol secrete IL-1β and IL-18 [101,102]. In concert, Ldlr − / − mice transplanted with bone marrow from mice lacking NLRP3 or ASC show a reduction in the lesion area and IL-18 levels [101]. Anti-inflammatory signalling Th2 cytokines The other end of the macrophage activity spectrum is Th2 cytokine-induced alternative activation, characterized by the expression of M2 markers, such as Arg1, Mgl1 and YM1 [29,71]. These macrophages function to repair damage elicited by pro-inflammatory M1 macrophages. As discussed above, in the lean state, ATMs display an M2 phenotype, suggesting that, at the physiological level, M2 macrophages may play an important role in metabolic homoeostasis [49]. In line with this notion, Th2 cytokines, notably IL-13, have been detected in WAT and liver [122]. Treatment of diet-induced obese mice with IL-4 significantly improves glucose homoeostasis and insulin sensitivity, whereas deletion of STAT6 (signal transducer and activator of transcription 6), a Th2 effector, worsens insulin resistance [123]. In addition, mice infected with helminth worms, which induce an M2 response, exhibit improved insulin sensitivity [124]. Nuclear receptors ER stress The ER is the site of protein folding, vesicle transport and lipid synthesis. When the capacity of ER is overburdened, the UPR (unfolded protein response) is activated characterized by increased activities of PERK (PKR-like ER kinase), IRE1 (inositol-requiring enzyme 1) and ATF6 (activating transcription factor 6) [103]. Activation of the UPR through these signalling molecules leads to downstream CHOP [C/EBP (CCAAT/enhancer-binding protein)-homologous protein] activation and subsequent induction of apoptosis. The initiation and propagation of the UPR and ER stress by obesity and metabolic stress have been reviewed in detail [103]. ER stress in adipose tissue or liver leads to insulin resistance, which is associated with activation of JNK and IKK, suggesting that ER stress is linked to inflammatory pathways [103–105]. In atherosclerosis, chronic activation of the ER stress pathway contributes to macrophage death and subsequent plaque necrosis [42]. CHOP expression and macrophage apoptosis have been correlated with advanced lesions [106,107], and deletion of CHOP suppresses lesional macrophage death/necrosis [108]. Lastly, it Nuclear receptors are ligand-activated transcription factors that control important biological processes [125]. Several lipidsensing nuclear receptors, such as the PPARs (PPARα, PPARδ and PPARγ , activated by dietary fatty acids) [126,127] and the LXRs (liver X receptors) (LXRα and LXRβ, activated by cholesterol metabolites) are drug targets to treat metabolic diseases [128,129]. In the macrophage, IL-4/IL-13-induced alternative macrophage activation is associated with increased fatty acid β-oxidation and oxidative metabolism [122,130], pathways regulated by PPARs [131]. Accordingly, PPARδ and PPARγ have been shown to be induced by Th2 cytokines and control M2 activation [122,132]. Mice with myeloid-specific deletion of PPARδ or PPARγ show increased M1 and decreased M2 markers in WAT and liver and develop systemic insulin resistance [122,132–135]. The M1/M2 paradigm is also relevant in Kupffer cells in the liver. Myeloid PPARδ deletion worsens hepatic steatosis in mice fed on a highfat diet [122,135]. It has been shown that macrophages from these mice produce factors that promote adipocyte and hepatocyte dysfunction in vitro [122]. Earlier studies also demonstrated an anti-inflammatory role for PPARs and LXRs, which correlates c The Authors Journal compilation c 2012 Biochemical Society 258 P. Bhargava and C.-H. Lee well with the atheroprotective roles for these nuclear receptors [136–138]. GPCRs (G-protein-coupled receptors) Although saturated fatty acids are known to induce inflammatory signalling pathways, epidemiological studies show that Mediterranean diets high in polyunsaturated ω − 3 (n − 3) fatty acids actually reduce the incidence of metabolic diseases [139– 142]. ω − 3 fatty acid derivatives, such as DHA (docosahexaenoic acid), EPA (eicosapentaenoic acid) and resolvins, exhibit antiinflammatory activities [143]. DHA and EPA have been shown to bind to the GPCR GPR120 on macrophage surfaces. GPR120 ligation inhibits the actions of TNFα and reverses insulin resistance brought on by a high-fat diet [144]. GPR120 and PPARs share several fatty acid ligands, suggesting potential cross-talk between these two signalling pathways [145]. CONCLUDING REMARKS The host immune system is essential for defending against foreign pathogens. Macrophages rely on the rapid influx of extracellular glucose for ATP production via anaerobic respiration [146–148]. As such, the ability of pathogen-stimulated macrophages to inhibit glucose uptake and insulin sensitivity in other metabolically demanding tissues is thought to be a mechanism by which immune cells sequester energy stores for defence [149–151]. However, in states of gluttony and energy storage, these evolutionary pathways have become detrimental. As the metabolic syndrome is a rapidly rising global epidemic affecting ∼ 8 % of the U.S. population alone and over 170 million people worldwide, efforts to identify effective therapies for treatment of associated pathologies are paramount [ADA (American Diabetes Association), WHO (World Health Organization)]. Exercise and healthy diets are most effective in improving the outcome of the metabolic syndrome [152,153]. However, lifestyle changes are often an unachievable ideal for many patients, and therefore development of medications is crucial. Growing evidence indicates that macrophage activation plays a key role in metabolic dysregulation. Understanding the contribution of macrophages to disease pathogenesis can help in the development of immunometabolic therapeutics to treat metabolic diseases. As described above, macrophages have evolved to sense dietary fats. The role of cholesterol in macrophage proinflammatory responses and atherosclerosis is well established. Studies have demonstrated further that fatty acids have a broad spectrum of activity on macrophage activation [77–79,144]. This is particularly relevant in obesity, in which the interaction of adipocyte and macrophage through fatty-acid-dependent mechanisms is critical to metabolic homoeostasis (Figure 3). Dietary ω − 3 fatty acids and their derivatives, including EPA, DHA and resolvins, can inhibit inflammatory responses through GPCRs or PPARs [143,144] and, as such, represent an attractive means for dietary intervention to reduce metabolic inflammation. In addition to dietary fats, studies have suggested that some amino acids, such as arginine and glutamine, promote insulin sensitivity and insulin secretion. However, epidemiological data also suggest that levels of branched-chain amino acids are associated with diabetes as early as 12 years before the onset of frank insulin resistance [154,155]. The role of amino-acid-sensing pathways in macrophage function and metabolic inflammation is currently unclear. In cultured macrophages, glutamine and arginine are critical for cytokine secretion, eicosanoid production and phagocytic uptake during macrophage activation [156]. mTOR c The Authors Journal compilation c 2012 Biochemical Society (mammalian target of rapamycin), a major amino-acid-sensing molecule, is anti-inflammatory in the macrophage. However, mTOR inhibition by rapamycin blocks MCP-1 production, despite its pro-inflammatory phenotype [157]. Additional work is needed to clarify the roles of amino acids in metabolic syndrome and whether these effects are mediated, in part, through macrophage activation. Although it is evident that metabolic stress (e.g. fatty acids, ceramides and oxLDL/cholesterol) induces macrophage inflammation, the detailed mechanisms through which proinflammatory signalling pathways cause metabolic diseases, notably in the setting of insulin resistance, remain unclear. For example, contradictory results have challenged the role of myeloid JNK1 in insulin resistance [158,159]. It appears that the initiation of a chronic inflammatory cycle may be due to loss of anti-inflammatory and/or regulatory signalling. However, the beneficial effects associated with alternative activation also require further investigation, as Th2 cytokines are known to mediate allergic responses. Recent studies have implicated several other immune cell types, such as T-lymphocytes, mast cells, natural killer cells and eosinophils, in the modulation of insulin sensitivity [124,160–165]. For example, T-cell-deficient Rag − / − (recombination-activating gene) mice are more susceptible to dietinduced obesity and adoptive transfer of CD4 + Foxp3 + (forkhead box P3) regulatory T-cells restores energy balance in these mice [160,165,166]. These studies indicate that the interactions between innate and adaptive immune systems also contribute to the onset of the metabolic syndrome and implicate an autoimmune response in the associated pathologies. What have not been described are the temporal recruitment and activation of various immune cells in metabolic tissues and the role of their interaction in metabolic diseases. Other anti-inflammatory or immunomodulatory mechanisms may be relevant in metabolic homoeostasis. Certain miRNAs (microRNAs) are up-regulated by TLR signalling and act through NF-κB pathways to dampen the inflammatory response [167,168]. miRNAs have also been implicated in atherosclerotic plaque initiation and expansion [169]. In addition, gut flora has been shown to modulate energy-utilization efficiency and adiposity and contribute to the onset of metabolic diseases [170,171]. Helminth infection is known to deactivate the immune response, and mice infected with parasitic worms exhibit improved insulin sensitivity, suggesting the potential use of helminthic antigens for therapies. Lastly, exercise reduces blood inflammatory markers and improves metabolic parameters. The so-called myokines produced by muscle after physical activity may modulate macrophage activation [172–175]. In fact, exercise-induced improvements in the inflammatory profile were found to be independent of weight loss [176,177]. Through understanding these different aspects of metabolic-related immune responses, it may be possible to design drugs to specifically target the feedforward loop of metabolic-stress-induced inflammation without unwanted side effects, such as immunosuppression or allergic responses. ACKNOWLEDGEMENT We thank K. Stanya for valuable comments. FUNDING P.B. is supported by the National Institute of Diabetes and Digestive and Kidney Disease (NIDDK) [training grant number T90DK070078]. C.H.L. is supported by the American Diabetes Association, the American Heart Association and the National Institutes of Health [grant number R01DK075046]. Role and function of macrophages in the metabolic syndrome REFERENCES 1 Gordon, S. (2007) The macrophage: past, present and future. Eur. J. Immunol. 37 (Suppl. 1), S9–S17 2 Grundy, S. M., Brewer, Jr, H. B., Cleeman, J. I., Smith, Jr, S. C. and Lenfant, C. (2004) Definition of metabolic syndrome: report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Arterioscler. Thromb. Vasc. Biol. 24, e13–e18 3 Williamson, R. T. (1901) On the treatment of glycosuria and diabetes mellitus with sodium salicylate. Br. Med. J. 1, 760–762 4 Hotamisligil, G. S., Murray, D. L., Choy, L. N. and Spiegelman, B. M. (1994) Tumor necrosis factor α inhibits signaling from the insulin receptor. Proc. Natl. Acad. Sci. U.S.A. 91, 4854–4858 5 Hotamisligil, G. S., Shargill, N. S. and Spiegelman, B. M. (1993) Adipose expression of tumor necrosis factor-α: direct role in obesity-linked insulin resistance. Science 259, 87–91 6 Wellen, K. E. and Hotamisligil, G. S. (2005) Inflammation, stress, and diabetes. J. Clin. Invest. 115, 1111–1119 7 Hotamisligil, G. S. and Erbay, E. (2008) Nutrient sensing and inflammation in metabolic diseases. Nat. Rev. Immunol. 8, 923–934 8 Karin, M., Lawrence, T. and Nizet, V. (2006) Innate immunity gone awry: linking microbial infections to chronic inflammation and cancer. Cell 124, 823–835 9 Hartman, M. E., O’Connor, J. C., Godbout, J. P., Minor, K. D., Mazzocco, V. R. and Freund, G. G. (2004) Insulin receptor substrate-2-dependent interleukin-4 signaling in macrophages is impaired in two models of type 2 diabetes mellitus. J. Biol. Chem. 279, 28045–28050 10 O’Connor, J. C., Sherry, C. L., Guest, C. B. and Freund, G. G. (2007) Type 2 diabetes impairs insulin receptor substrate-2-mediated phosphatidylinositol 3-kinase activity in primary macrophages to induce a state of cytokine resistance to IL-4 in association with overexpression of suppressor of cytokine signaling-3. J. Immunol. 178, 6886–6893 11 Rosa, L. F., Cury, Y. and Curi, R. (1992) Effects of insulin, glucocorticoids and thyroid hormones on the activities of key enzymes of glycolysis, glutaminolysis, the pentose-phosphate pathway and the Krebs cycle in rat macrophages. J. Endocrinol. 135, 213–219 12 Bala, M., Kopp, A., Wurm, S., Buchler, C., Scholmerich, J. and Schaffler, A. (2011) Type 2 diabetes and lipoprotein metabolism affect LPS-induced cytokine and chemokine release in primary human monocytes. Exp. Clin. Endocrinol. Diabetes 119, 370–376 13 Geerlings, S. E., Brouwer, E. C., van Kessel, K. P., Gaastra, W. and Hoepelman, A. M. (2000) Cytokine secretion is impaired in women with diabetes mellitus. Adv. Exp. Med. Biol. 485, 255–262 14 Vejlsgaard, R. (1966) Studies on urinary infection in diabetics. I. Bacteriuria in patients with diabetes mellitus and in control subjects. Acta Med. Scand. 179, 173–182 15 Geerlings, S. E. and Hoepelman, A. I. (1999) Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol. Med. Microbiol. 26, 259–265 16 Chelvarajan, R. L., Liu, Y., Popa, D., Getchell, M. L., Getchell, T. V., Stromberg, A. J. and Bondada, S. (2006) Molecular basis of age-associated cytokine dysregulation in LPS-stimulated macrophages. J. Leukocyte Biol. 79, 1314–1327 17 Weisberg, S. P., McCann, D., Desai, M., Rosenbaum, M., Leibel, R. L. and Ferrante, Jr, A. W. (2003) Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Invest. 112, 1796–1808 18 Xu, H., Barnes, G. T., Yang, Q., Tan, G., Yang, D., Chou, C. J., Sole, J., Nichols, A., Ross, J. S., Tartaglia, L. A. and Chen, H. (2003) Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J. Clin. Invest. 112, 1821–1830 19 Dawson, T. C., Kuziel, W. A., Osahar, T. A. and Maeda, N. (1999) Absence of CC chemokine receptor-2 reduces atherosclerosis in apolipoprotein E-deficient mice. Atherosclerosis 143, 205–211 20 Gosling, J., Slaymaker, S., Gu, L., Tseng, S., Zlot, C. H., Young, S. G., Rollins, B. J. and Charo, I. F. (1999) MCP-1 deficiency reduces susceptibility to atherosclerosis in mice that overexpress human apolipoprotein B. J. Clin. Invest. 103, 773–778 21 Boring, L., Gosling, J., Cleary, M. and Charo, I. F. (1998) Decreased lesion formation in CCR2 − / − mice reveals a role for chemokines in the initiation of atherosclerosis. Nature 394, 894–897 22 Weisberg, S. P., Hunter, D., Huber, R., Lemieux, J., Slaymaker, S., Vaddi, K., Charo, I., Leibel, R. L. and Ferrante, Jr, A. W. (2006) CCR2 modulates inflammatory and metabolic effects of high-fat feeding. J. Clin. Invest. 116, 115–124 23 Kanda, H. (2006) MCP-1 contributes to macrophage infiltration into adipose tissue, insulin resistance, and hepatic steatosis in obesity. J. Clin. Invest. 116, 1494–1505 24 Kamei, N. (2006) Overexpression of monocyte chemoattractant protein-1 in adipose tissues causes macrophage recruitment and insulin resistance. J. Biol. Chem. 281, 26602–26614 259 25 Kiefer, F. W., Zeyda, M., Gollinger, K., Pfau, B., Neuhofer, A., Weichhart, T., Saemann, M. D., Geyeregger, R., Schlederer, M., Kenner, L. and Stulnig, T. M. (2010) Neutralization of osteopontin inhibits obesity-induced inflammation and insulin resistance. Diabetes 59, 935–946 26 Nomiyama, T., Perez-Tilve, D., Ogawa, D., Gizard, F., Zhao, Y., Heywood, E. B., Jones, K. L., Kawamori, R., Cassis, L. A., Tschop, M. H. and Bruemmer, D. (2007) Osteopontin mediates obesity-induced adipose tissue macrophage infiltration and insulin resistance in mice. J. Clin. Invest. 117, 2877–2888 27 Nara, N., Nakayama, Y., Okamoto, S., Tamura, H., Kiyono, M., Muraoka, M., Tanaka, K., Taya, C., Shitara, H., Ishii, R. et al. (2007) Disruption of CXC motif chemokine ligand-14 in mice ameliorates obesity-induced insulin resistance. J. Biol. Chem. 282, 30794–30803 28 Tabata, M., Kadomatsu, T., Fukuhara, S., Miyata, K., Ito, Y., Endo, M., Urano, T., Zhu, H. J., Tsukano, H., Tazume, H. et al. (2009) Angiopoietin-like protein 2 promotes chronic adipose tissue inflammation and obesity-related systemic insulin resistance. Cell Metab. 10, 178–188 29 Mosser, D. M. and Edwards, J. P. (2008) Exploring the full spectrum of macrophage activation. Nat. Rev. Immunol. 8, 958–969 30 Del Prete, G., De Carli, M., Almerigogna, F., Giudizi, M. G., Biagiotti, R. and Romagnani, S. (1993) Human IL-10 is produced by both type 1 helper (Th1) and type 2 helper (Th2) T cell clones and inhibits their antigen-specific proliferation and cytokine production. J. Immunol. 150, 353–360 31 Fiorentino, D. F., Zlotnik, A., Vieira, P., Mosmann, T. R., Howard, M., Moore, K. W. and O’Garra, A. (1991) IL-10 acts on the antigen-presenting cell to inhibit cytokine production by Th1 cells. J. Immunol. 146, 3444–3451 32 Fiorentino, D. F., Zlotnik, A., Mosmann, T. R., Howard, M. and O’Garra, A. (1991) IL-10 inhibits cytokine production by activated macrophages. J. Immunol. 147, 3815–3822 33 de Waal Malefyt, R., Abrams, J., Bennett, B., Figdor, C. G. and de Vries, J. E. (1991) Interleukin 10 (IL-10) inhibits cytokine synthesis by human monocytes: an autoregulatory role of IL-10 produced by monocytes. J. Exp. Med. 174, 1209–1220 34 Baumgartl, J., Baudler, S., Scherner, M., Babaev, V., Makowski, L., Suttles, J., McDuffie, M., Tobe, K., Kadowaki, T., Fazio, S. et al. (2006) Myeloid lineage cell-restricted insulin resistance protects apolipoprotein E-deficient mice against atherosclerosis. Cell Metab. 3, 247–256 35 Kanters, E., Pasparakis, M., Gijbels, M. J., Vergouwe, M. N., Partouns-Hendriks, I., Fijneman, R. J., Clausen, B. E., Forster, I., Kockx, M. M., Rajewsky, K. et al. (2003) Inhibition of NF-κB activation in macrophages increases atherosclerosis in LDL receptor-deficient mice. J. Clin. Invest. 112, 1176–1185 36 Baker, R. G., Hayden, M. S. and Ghosh, S. (2011) NF-κB, inflammation, and metabolic disease. Cell Metab. 13, 11–22 37 Chang, Y. H., Huang, C. N., Wu, C. Y. and Shiau, M. Y. (2005) Association of interleukin-10 A-592C and T-819C polymorphisms with type 2 diabetes mellitus. Hum. Immunol. 66, 1258–1263 38 Erdogan, M., Cetinkalp, S., Ozgen, A. G., Saygili, F., Berdeli, A. and Yilmaz, C. (2011) Interleukin-10 ( − 1082G/A) gene polymorphism in patients with type 2 diabetes with and without nephropathy. Genet. Test. Mol. Biomarkers, doi:10.1089/gtmb.2011.0075 39 Scarpelli, D., Cardellini, M., Andreozzi, F., Laratta, E., Hribal, M. L., Marini, M. A., Tassi, V., Lauro, R., Perticone, F. and Sesti, G. (2006) Variants of the interleukin-10 promoter gene are associated with obesity and insulin resistance but not type 2 diabetes in Caucasian Italian subjects. Diabetes 55, 1529–1533 40 Satoh, N., Shimatsu, A., Himeno, A., Sasaki, Y., Yamakage, H., Yamada, K., Suganami, T. and Ogawa, Y. (2010) Unbalanced M1/M2 phenotype of peripheral blood monocytes in obese diabetic patients: effect of pioglitazone. Diabetes Care 33, e7 41 Tabas, I., Tall, A. and Accili, D. (2010) The impact of macrophage insulin resistance on advanced atherosclerotic plaque progression. Circ. Res. 106, 58–67 42 Tabas, I. (2010) The role of endoplasmic reticulum stress in the progression of atherosclerosis. Circ. Res. 107, 839–850 43 Ball, R. Y., Stowers, E. C., Burton, J. H., Cary, N. R., Skepper, J. N. and Mitchinson, M. J. (1995) Evidence that the death of macrophage foam cells contributes to the lipid core of atheroma. Atherosclerosis 114, 45–54 44 Tabas, I. (2005) Consequences and therapeutic implications of macrophage apoptosis in atherosclerosis: the importance of lesion stage and phagocytic efficiency. Arterioscler. Thromb. Vasc. Biol. 25, 2255–2264 45 Hegyi, L., Skepper, J. N., Cary, N. R. and Mitchinson, M. J. (1996) Foam cell apoptosis and the development of the lipid core of human atherosclerosis. J. Pathol. 180, 423–429 46 Fadok, V. A., Bratton, D. L. and Henson, P. M. (2001) Phagocyte receptors for apoptotic cells: recognition, uptake, and consequences. J. Clin. Invest. 108, 957–962 47 Marée, A. F. M., Komba, M., Dyck, C., Łabecki, M., Finegood, D. T. and Edelstein-Keshet, L. (2005) Quantifying macrophage defects in type 1 diabetes. J. Theor. Biol. 233, 533–551 48 Yvan-Charvet, L., Pagler, T. A., Seimon, T. A., Thorp, E., Welch, C. L., Witztum, J. L., Tabas, I. and Tall, A. R. (2010) ABCA1 and ABCG1 protect against oxidative stress-induced macrophage apoptosis during efferocytosis. Circ Res. 106, 1861–1869 c The Authors Journal compilation c 2012 Biochemical Society 260 P. Bhargava and C.-H. Lee 49 Lumeng, C. N., Bodzin, J. L. and Saltiel, A. R. (2007) Obesity induces a phenotypic switch in adipose tissue macrophage polarization. J. Clin. Invest. 117, 175–184 50 Guerre-Millo, M. (2004) Adipose tissue and adipokines: for better or worse. Diabetes Metab. 30, 13–19 51 Ye, J. (2009) Emerging role of adipose tissue hypoxia in obesity and insulin resistance. Int. J. Obes. Relat. Metab. Disord. 33, 54–66 52 Yin, J., Gao, Z., He, Q., Zhou, D., Guo, Z. and Ye, J. (2009) Role of hypoxia in obesity-induced disorders of glucose and lipid metabolism in adipose tissue. Am. J. Physiol. Endocrinol. Metab. 296, E333–E342 53 Patsouris, D., Li, P., Thapar, D., Chapman, J., Olefsky, J. and Neels, J. (2008) Ablation of CD11c-positive cells normalizes insulin sensitivity in obese insulin resistant animals. Cell Metab. 8, 301–309 54 Fitzgibbons, T. P., Kogan, S., Aouadi, M., Hendricks, G. M., Straubhaar, J. and Czech, M. P. (2011) Similarity of mouse perivascular and brown adipose tissues and their resistance to diet-induced inflammation. Am. J. Physiol. Heart Circ. Physiol. 301, H1425–H1437 55 Ortega, M. T., Xie, L., Mora, S. and Chapes, S. K. (2011) Evaluation of macrophage plasticity in brown and white adipose tissue. Cell. Immunol. 271, 124–133 56 Glass, C. K. and Witztum, J. L. (2001) Atherosclerosis: the road ahead. Cell 104, 503–516 57 Moore, K. J. and Tabas, I. (2011) Macrophages in the pathogenesis of atherosclerosis. Cell 145, 341–355 58 Kunjathoor, V. V., Febbraio, M., Podrez, E. A., Moore, K. J., Andersson, L., Koehn, S., Rhee, J. S., Silverstein, R., Hoff, H. F. and Freeman, M. W. (2002) Scavenger receptors class A-I/II and CD36 are the principal receptors responsible for the uptake of modified low density lipoprotein leading to lipid loading in macrophages. J. Biol. Chem. 277, 49982–49988 59 Elizondo, A., Araya, J., Rodrigo, R., Poniachik, J., Csendes, A., Maluenda, F., Diaz, J. C., Signorini, C., Sgherri, C., Comporti, M. and Videla, L. A. (2007) Polyunsaturated fatty acid pattern in liver and erythrocyte phospholipids from obese patients. Obesity 15, 24–31 60 Wouters, K., van Gorp, P. J., Bieghs, V., Gijbels, M. J., Duimel, H., Lutjohann, D., Kerksiek, A., van Kruchten, R., Maeda, N., Staels, B. et al. (2008) Dietary cholesterol, rather than liver steatosis, leads to hepatic inflammation in hyperlipidemic mouse models of nonalcoholic steatohepatitis. Hepatology 48, 474–486 61 Shoelson, S. E., Herrero, L. and Naaz, A. (2007) Obesity, inflammation, and insulin resistance. Gastroenterology 132, 2169–2180 62 Maher, J. J., Leon, P. and Ryan, J. C. (2008) Beyond insulin resistance: innate immunity in nonalcoholic steatohepatitis. Hepatology 48, 670–678 63 Rivera, C. A., Adegboyega, P., van Rooijen, N., Tagalicud, A., Allman, M. and Wallace, M. (2007) Toll-like receptor-4 signaling and Kupffer cells play pivotal roles in the pathogenesis of non-alcoholic steatohepatitis. J. Hepatol. 47, 571–579 64 Huang, W., Metlakunta, A., Dedousis, N., Zhang, P., Sipula, I., Dube, J. J., Scott, D. K. and O’Doherty, R. M. (2010) Depletion of liver Kupffer cells prevents the development of diet-induced hepatic steatosis and insulin resistance. Diabetes 59, 347–357 65 Neyrinck, A. M., Cani, P. D., Dewulf, E. M., Backer, F. D., Bindels, L. B. and Delzenne, N. M. (2009) Critical role of Kupffer cells in the management of diet-induced diabetes and obesity. Biochem. Biophys. Res. Commun. 385, 351–356 66 Lanthier, N., Molendi-Coste, O., Horsmans, Y., van Rooijen, N., Cani, P. D. and Leclercq, I. A. (2010) Kupffer cell activation is a causal factor for hepatic insulin resistance. Am. J. Physiol. Gastrointest. Liver Physiol. 298, G107–G116 67 Kang, K., Hatano, B. and Lee, C. H. (2007) PPARδ agonists and metabolic diseases. Curr. Atheroscler. Rep. 9, 72–77 68 Chazaud, B., Brigitte, M., Yacoub-Youssef, H., Arnold, L., Gherardi, R., Sonnet, C., Lafuste, P. and Chretien, F. (2009) Dual and beneficial roles of macrophages during skeletal muscle regeneration. Exercise Sport Sci. Rev. 37, 18–22 69 Cai, D., Yuan, M., Frantz, D. F., Melendez, P. A., Hansen, L., Lee, J. and Shoelson, S. E. (2005) Local and systemic insulin resistance resulting from hepatic activation of IKK-β and NF-κB. Nat. Med. 11, 183–190 70 Hirosumi, J., Tuncman, G., Chang, L., Gorgun, C. Z., Uysal, K. T., Maeda, K., Karin, M. and Hotamisligil, G. S. (2002) A central role for JNK in obesity and insulin resistance. Nature 420, 333–336 71 Martinez, F. O., Helming, L. and Gordon, S. (2009) Alternative activation of macrophages: an immunologic functional perspective. Annu. Rev. Immunol. 27, 451–483 72 Solinas, G., Vilcu, C., Neels, J., Bandyopadhyay, G., Luo, J., Naugler, W., Grivennikov, S., Wynshawboris, A., Scadeng, M. and Olefsky, J. (2007) JNK1 in hematopoietically derived cells contributes to diet-induced inflammation and insulin resistance without affecting obesity. Cell Metab. 6, 386–397 73 Romanatto, T., Roman, E. A., Arruda, A. P., Denis, R. G., Solon, C., Milanski, M., Moraes, J. C., Bonfleur, M. L., Degasperi, G. R., Picardi, P. K. et al. (2009) Deletion of tumor necrosis factor-α receptor 1 (TNFR1) protects against diet-induced obesity by means of increased thermogenesis. J. Biol. Chem. 284, 36213–36222 c The Authors Journal compilation c 2012 Biochemical Society 74 De Taeye, B. M., Novitskaya, T., Mcguinness, O. P., Gleaves, L., Medda, M., Covington, J. W. and Vaughan, D. E. (2007) Macrophage TNF-α contributes to insulin resistance and hepatic steatosis in diet-induced obesity. Am. J. Physiol. Endocrinol. Metab. 293, E713–E725 75 Nakamura, T., Furuhashi, M., Li, P., Cao, H., Tuncman, G., Sonenberg, N., Gorgun, C. Z. and Hotamisligil, G. S. (2010) Double-stranded RNA-dependent protein kinase links pathogen sensing with stress and metabolic homeostasis. Cell 140, 338–348 76 Kumar, H., Kawai, T. and Akira, S. (2009) Pathogen recognition in the innate immune response. Biochem. J. 420, 1–16 77 Nguyen, M. T., Favelyukis, S., Nguyen, A.-K., Reichart, D., Scott, P. A., Jenn, A., Liu-Bryan, R., Glass, C. K., Neels, J. G. and Olefsky, J. M. (2007) A subpopulation of macrophages infiltrates hypertrophic adipose tissue and is activated by free fatty acids via Toll-like receptors 2 and 4 and JNK-dependent pathways. J. Biol. Chem. 282, 35279–35292 78 Shi, H., Kokoeva, M. V., Inouye, K., Tzameli, I., Yin, H. and Flier, J. S. (2006) TLR4 links innate immunity and fatty acid-induced insulin resistance. J. Clin. Invest. 116, 3015–3025 79 Holland, W. L., Bikman, B. T., Wang, L.-P., Yuguang, G., Sargent, K. M., Bulchand, S., Knotts, T. A., Shui, G., Clegg, D. J., Wenk, M. R. et al. (2011) Lipid-induced insulin resistance mediated by the proinflammatory receptor TLR4 requires saturated fatty acid-induced ceramide biosynthesis in mice. J. Clin. Invest. 121, 1858–1870 80 Poggi, M., Bastelica, D., Gual, P., Iglesias, M. A., Gremeaux, T., Knauf, C., Peiretti, F., Verdier, M., Juhan-Vague, I., Tanti, J. F. et al. (2007) C3H/HeJ mice carrying a Toll-like receptor 4 mutation are protected against the development of insulin resistance in white adipose tissue in response to a high-fat diet. Diabetologia 50, 1267–1276 81 Tsukumo, D. M., Carvalho-Filho, M. A., Carvalheira, J. B., Prada, P. O., Hirabara, S. M., Schenka, A. A., Araujo, E. P., Vassallo, J., Curi, R., Velloso, L. A. and Saad, M. J. (2007) Loss-of-function mutation in Toll-like receptor 4 prevents diet-induced obesity and insulin resistance. Diabetes 56, 1986–1998 82 Davis, J. E., Gabler, N. K., Walker-Daniels, J. and Spurlock, M. E. (2008) Tlr-4 deficiency selectively protects against obesity induced by diets high in saturated fat. Obesity 16, 1248–1255 83 Saberi, M., Woods, N.-B., de Luca, C., Schenk, S., Lu, J. C., Bandyopadhyay, G., Verma, I. M. and Olefsky, J. M. (2009) Hematopoietic cell-specific deletion of Toll-like receptor 4 ameliorates hepatic and adipose tissue insulin resistance in high-fat-fed mice. Cell Metab. 10, 419–429 84 Arkan, M. C., Hevener, A. L., Greten, F. R., Maeda, S., Li, Z. W., Long, J. M., Wynshaw-Boris, A., Poli, G., Olefsky, J. and Karin, M. (2005) IKK-β links inflammation to obesity-induced insulin resistance. Nat. Med. 11, 191–198 85 Chiang, S. H., Bazuine, M., Lumeng, C. N., Geletka, L. M., Mowers, J., White, N. M., Ma, J. T., Zhou, J., Qi, N., Westcott, D. et al. (2009) The protein kinase IKKε regulates energy balance in obese mice. Cell 138, 961–975 86 Yuan, M. (2001) Reversal of obesity- and diet-induced insulin resistance with salicylates or targeted disruption of IKKβ. Science 293, 1673–1677 87 Shoelson, S. E., Lee, J. and Yuan, M. (2003) Inflammation and the IKKβ/IκB/NF-κB axis in obesity- and diet-induced insulin resistance. Int. J. Obes. Relat. Metab. Disord. 27 (Suppl. 3), S49–S52 88 Hundal, R. S., Petersen, K. F., Mayerson, A. B., Randhawa, P. S., Inzucchi, S., Shoelson, S. E. and Shulman, G. I. (2002) Mechanism by which high-dose aspirin improves glucose metabolism in type 2 diabetes. J. Clin. Invest. 109, 1321–1326 89 Mullick, A. E., Tobias, P. S. and Curtiss, L. K. (2005) Modulation of atherosclerosis in mice by Toll-like receptor 2. J. Clin. Invest. 115, 3149–3156 90 Michelsen, K. S., Wong, M. H., Shah, P. K., Zhang, W., Yano, J., Doherty, T. M., Akira, S., Rajavashisth, T. B. and Arditi, M. (2004) Lack of Toll-like receptor 4 or myeloid differentiation factor 88 reduces atherosclerosis and alters plaque phenotype in mice deficient in apolipoprotein E. Proc. Natl. Acad. Sci. U.S.A. 101, 10679–10684 91 Kanters, E., Gijbels, M. J., van der Made, I., Vergouwe, M. N., Heeringa, P., Kraal, G., Hofker, M. H. and de Winther, M. P. (2004) Hematopoietic NF-κB1 deficiency results in small atherosclerotic lesions with an inflammatory phenotype. Blood 103, 934–940 92 Ferreira, V., van Dijk, K. W., Groen, A. K., Vos, R. M., van der Kaa, J., Gijbels, M. J., Havekes, L. M. and Pannekoek, H. (2007) Macrophage-specific inhibition of NF-κB activation reduces foam-cell formation. Atherosclerosis 192, 283–290 93 Dunne, A. (2011) Inflammasome activation: from inflammatory disease to infection. Biochem. Soc. Trans. 39, 669–673 94 Jin, C. and Flavell, R. A. (2010) Molecular mechanism of NLRP3 inflammasome activation. J. Clin. Immunol. 30, 628–631 95 Lumeng, C. N. and Saltiel, A. R. (2011) Inflammatory links between obesity and metabolic disease. J. Clin. Invest. 121, 2111–2117 96 Martinon, F., Mayor, A. and Tschopp, J. (2009) The inflammasomes: guardians of the body. Annu. Rev. Immunol. 27, 229–265 97 Wen, H., Gris, D., Lei, Y., Jha, S., Zhang, L., Huang, M. T., Brickey, W. J. and Ting, J. P. (2011) Fatty acid-induced NLRP3-ASC inflammasome activation interferes with insulin signaling. Nat. Immunol. 12, 408–415 Role and function of macrophages in the metabolic syndrome 98 Stienstra, R., Joosten, L. A., Koenen, T., van Tits, B., van Diepen, J. A., van den Berg, S. A., Rensen, P. C., Voshol, P. J., Fantuzzi, G., Hijmans, A. et al. (2010) The inflammasome-mediated caspase-1 activation controls adipocyte differentiation and insulin sensitivity. Cell Metab. 12, 593–605 99 Vandanmagsar, B., Youm, Y.-H., Ravussin, A., Galgani, J. E., Stadler, K., Mynatt, R. L., Ravussin, E., Stephens, J. M. and Dixit, V. D. (2011) The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat. Med. 17, 179–188 100 McGillicuddy, F. C., Harford, K. A., Reynolds, C. M., Oliver, E., Claessens, M., Mills, K. H.G. and Roche, H. M. (2011) Lack of interleukin-1 receptor I (IL-1RI) protects mice from high-fat diet-induced adipose tissue inflammation coincident with improved glucose homeostasis. Diabetes 60, 1688–1698 101 Duewell, P., Kono, H., Rayner, K. J., Sirois, C. M., Vladimer, G., Bauernfeind, F. G., Abela, G. S., Franchi, L., Nunez, G., Schnurr, M. et al. (2010) NLRP3 inflammasomes are required for atherogenesis and activated by cholesterol crystals. Nature 464, 1357–1361 102 Rajamaki, K., Lappalainen, J., Oorni, K., Valimaki, E., Matikainen, S., Kovanen, P. T. and Eklund, K. K. (2010) Cholesterol crystals activate the NLRP3 inflammasome in human macrophages: a novel link between cholesterol metabolism and inflammation. PLoS ONE 5, e11765 103 Hotamisligil, G. S. (2005) Role of endoplasmic reticulum stress and c-Jun NH2 -terminal kinase pathways in inflammation and origin of obesity and diabetes. Diabetes 54 (Suppl. 2), S73–S78 104 Hotamisligil, G. S. (2006) Inflammation and metabolic disorders. Nature 444, 860–867 105 Ozcan, U., Cao, Q., Yilmaz, E., Lee, A. H., Iwakoshi, N. N., Ozdelen, E., Tuncman, G., Gorgun, C., Glimcher, L. H. and Hotamisligil, G. S. (2004) Endoplasmic reticulum stress links obesity, insulin action, and type 2 diabetes. Science 306, 457–461 106 Han, S., Liang, C. P., DeVries-Seimon, T., Ranalletta, M., Welch, C. L., Collins-Fletcher, K., Accili, D., Tabas, I. and Tall, A. R. (2006) Macrophage insulin receptor deficiency increases ER stress-induced apoptosis and necrotic core formation in advanced atherosclerotic lesions. Cell Metab. 3, 257–266 107 Myoishi, M., Hao, H., Minamino, T., Watanabe, K., Nishihira, K., Hatakeyama, K., Asada, Y., Okada, K., Ishibashi-Ueda, H., Gabbiani, G. et al. (2007) Increased endoplasmic reticulum stress in atherosclerotic plaques associated with acute coronary syndrome. Circulation 116, 1226–1233 108 Thorp, E., Li, G., Seimon, T. A., Kuriakose, G., Ron, D. and Tabas, I. (2009) Reduced apoptosis and plaque necrosis in advanced atherosclerotic lesions of Apoe − / − and Ldlr − / − mice lacking CHOP. Cell Metab. 9, 474–481 109 Erbay, E., Babaev, V. R., Mayers, J. R., Makowski, L., Charles, K. N., Snitow, M. E., Fazio, S., Wiest, M. M., Watkins, S. M., Linton, M. F. and Hotamisligil, G. S. (2009) Reducing endoplasmic reticulum stress through a macrophage lipid chaperone alleviates atherosclerosis. Nat. Med. 15, 1383–1391 110 Blouin, C. C., Page, E. L., Soucy, G. M. and Richard, D. E. (2004) Hypoxic gene activation by lipopolysaccharide in macrophages: implication of hypoxia-inducible factor 1α. Blood 103, 1124–1130 111 Cramer, T. and Johnson, R. S. (2003) A novel role for the hypoxia inducible transcription factor HIF-1α: critical regulation of inflammatory cell function. Cell Cycle 2, 192–193 112 Cramer, T., Yamanishi, Y., Clausen, B. E., Forster, I., Pawlinski, R., Mackman, N., Haase, V. H., Jaenisch, R., Corr, M., Nizet, V. et al. (2003) HIF-1α is essential for myeloid cell-mediated inflammation. Cell 112, 645–657 113 Peyssonnaux, C., Datta, V., Cramer, T., Doedens, A., Theodorakis, E. A., Gallo, R. L., Hurtado-Ziola, N., Nizet, V. and Johnson, R. S. (2005) HIF-1α expression regulates the bactericidal capacity of phagocytes. J. Clin. Invest. 115, 1806–1815 114 Zinkernagel, A. S., Johnson, R. S. and Nizet, V. (2007) Hypoxia inducible factor (HIF) function in innate immunity and infection. J. Mol. Med. 85, 1339–1346 115 Hosogai, N., Fukuhara, A., Oshima, K., Miyata, Y., Tanaka, S., Segawa, K., Furukawa, S., Tochino, Y., Komuro, R., Matsuda, M. and Shimomura, I. (2007) Adipose tissue hypoxia in obesity and its impact on adipocytokine dysregulation. Diabetes 56, 901–911 116 Rausch, M. E., Weisberg, S., Vardhana, P. and Tortoriello, D. V. (2008) Obesity in C57BL/6J mice is characterized by adipose tissue hypoxia and cytotoxic T-cell infiltration. Int. J. Obes. 32, 451–463 117 Iiyori, N., Alonso, L. C., Li, J., Sanders, M. H., Garcia-Ocana, A., O’Doherty, R. M., Polotsky, V. Y. and O’Donnell, C. P. (2007) Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am. J. Respir. Crit. Care Med. 175, 851–857 118 Aron-Wisnewsky, J., Minville, C., Tordjman, J., Lévy, P., Bouillot, J. L., Basdevant, A., Bedossa, P., Clement, K. and Pepin, J. L. (2011) Chronic intermittent hypoxia is a major trigger for non-alcoholic fatty liver disease in morbid obese. J. Hepatol. 56, 225–233 119 Deguchi, J. O., Yamazaki, H., Aikawa, E. and Aikawa, M. (2009) Chronic hypoxia activates the Akt and β-catenin pathways in human macrophages. Arterioscler. Thromb. Vasc. Biol. 29, 1664–1670 120 Parathath, S., Mick, S. L., Feig, J. E., Joaquin, V., Grauer, L., Habiel, D. M., Gassmann, M., Gardner, L. B. and Fisher, E. A. (2011) Hypoxia is present in murine atherosclerotic plaques and has multiple adverse effects on macrophage lipid metabolism. Circ. Res. 109, 1141–1152 261 121 Arnaud, C., Poulain, L., Lévy, P. and Dematteis, M. (2011) Inflammation contributes to the atherogenic role of intermittent hypoxia in apolipoprotein-E knock out mice. Atherosclerosis 219, 425–431 122 Kang, K., Reilly, S. M., Karabacak, V., Gangl, M. R., Fitzgerald, K., Hatano, B. and Lee, C. H. (2008) Adipocyte-derived Th2 cytokines and myeloid PPARδ regulate macrophage polarization and insulin sensitivity. Cell Metab. 7, 485–495 123 Ricardo-Gonzalez, R. R., Red Eagle, A., Odegaard, J. I., Jouihan, H., Morel, C. R., Heredia, J. E., Mukundan, L., Wu, D., Locksley, R. M. and Chawla, A. (2010) IL-4/STAT6 immune axis regulates peripheral nutrient metabolism and insulin sensitivity. Proc. Natl. Acad. Sci. U.S.A. 107, 22617–22622 124 Wu, D., Molofsky, A. B., Liang, H. E., Ricardo-Gonzalez, R. R., Jouihan, H. A., Bando, J. K., Chawla, A. and Locksley, R. M. (2011) Eosinophils sustain adipose alternatively activated macrophages associated with glucose homeostasis. Science 332, 243–247 125 Chawla, A., Repa, J. J., Evans, R. M. and Mangelsdorf, D. J. (2001) Nuclear receptors and lipid physiology: opening the X-files. Science 294, 1866–1870 126 Lee, C. H., Olson, P. and Evans, R. M. (2003) Minireview: lipid metabolism, metabolic diseases, and peroxisome proliferator-activated receptors. Endocrinology 144, 2201–2207 127 Reilly, S. M. and Lee, C. H. (2008) PPARδ as a therapeutic target in metabolic disease. FEBS Lett. 582, 26–31 128 Szanto, A. and Roszer, T. (2008) Nuclear receptors in macrophages: a link between metabolism and inflammation. FEBS Lett. 582, 106–116 129 Hong, C. and Tontonoz, P. (2008) Coordination of inflammation and metabolism by PPAR and LXR nuclear receptors. Curr. Opin. Genet. Dev. 18, 461–467 130 Vats, D., Mukundan, L., Odegaard, J. I., Zhang, L., Smith, K. L., Morel, C. R., Wagner, R. A., Greaves, D. R., Murray, P. J. and Chawla, A. (2006) Oxidative metabolism and PGC-1β attenuate macrophage-mediated inflammation. Cell Metab. 4, 13–24 131 Lee, C. H., Kang, K., Mehl, I. R., Nofsinger, R., Alaynick, W. A., Chong, L. W., Rosenfeld, J. M. and Evans, R. M. (2006) Peroxisome proliferator-activated receptor δ promotes very low-density lipoprotein-derived fatty acid catabolism in the macrophage. Proc. Natl. Acad. Sci. U.S.A. 103, 2434–2439 132 Odegaard, J. I., Ricardo-Gonzalez, R. R., Goforth, M. H., Morel, C. R., Subramanian, V., Mukundan, L., Eagle, A. R., Vats, D., Brombacher, F., Ferrante, A. W. and Chawla, A. (2007) Macrophage-specific PPARγ controls alternative activation and improves insulin resistance. Nature 447, 1116–1120 133 Bouhlel, M. A., Derudas, B., Rigamonti, E., Dievart, R., Brozek, J., Haulon, S., Zawadzki, C., Jude, B., Torpier, G., Marx, N. et al. (2007) PPARγ activation primes human monocytes into alternative M2 macrophages with anti-inflammatory properties. Cell Metab. 6, 137–143 134 Hevener, A. L., Olefsky, J. M., Reichart, D., Nguyen, M. T., Bandyopadyhay, G., Leung, H. Y., Watt, M. J., Benner, C., Febbraio, M. A., Nguyen, A. K. et al. (2007) Macrophage PPARγ is required for normal skeletal muscle and hepatic insulin sensitivity and full antidiabetic effects of thiazolidinediones. J. Clin. Invest. 117, 1658–1669 135 Odegaard, J. I., Ricardo-Gonzalez, R. R., Red Eagle, A., Vats, D., Morel, C. R., Goforth, M. H., Subramanian, V., Mukundan, L., Ferrante, A. W. and Chawla, A. (2008) Alternative M2 activation of Kupffer cells by PPARδ ameliorates obesity-induced insulin resistance. Cell Metab. 7, 496–507 136 Chawla, A. (2010) Control of macrophage activation and function by PPARs. Circ. Res. 106, 1559–1569 137 Barish, G. D., Narkar, V. A. and Evans, R. M. (2006) PPARδ: a dagger in the heart of the metabolic syndrome. J. Clin. Invest. 116, 590–597 138 Rigamonti, E., Chinetti-Gbaguidi, G. and Staels, B. (2008) Regulation of macrophage functions by PPAR-α, PPAR-γ , and LXRs in mice and men. Arterioscler. Thromb. Vasc. Biol. 28, 1050–1059 139 de Lorgeril, M., Renaud, S., Mamelle, N., Salen, P., Martin, J. L., Monjaud, I., Guidollet, J., Touboul, P. and Delaye, J. (1994) Mediterranean α-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 343, 1454–1459 140 Esposito, K., Marfella, R., Ciotola, M., Di Palo, C., Giugliano, F., Giugliano, G., D’Armiento, M., D’Andrea, F. and Giugliano, D. (2004) Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA, J. Am. Med. Assoc. 292, 1440–1446 141 Kabir, M., Skurnik, G., Naour, N., Pechtner, V., Meugnier, E., Rome, S., Quignard-Boulangé, A., Vidal, H., Slama, G., Clément, K. et al. (2007) Treatment for 2 mo with n − 3 polyunsaturated fatty acids reduces adiposity and some atherogenic factors but does not improve insulin sensitivity in women with type 2 diabetes: a randomized controlled study. Am. J. Clin. Nutr. 86, 1670–1679 142 Yashodhara, B. M., Umakanth, S., Pappachan, J. M., Bhat, S. K., Kamath, R. and Choo, B. H. (2009) ω − 3 fatty acids: a comprehensive review of their role in health and disease. Postgrad. Med. J. 85, 84–90 143 Serhan, C. N. (2009) Systems approach to inflammation resolution: identification of novel anti-inflammatory and pro-resolving mediators. J. Thromb. Haemostasis 7 (Suppl. 1), 44–48 c The Authors Journal compilation c 2012 Biochemical Society 262 P. Bhargava and C.-H. Lee 144 Oh, D. Y., Talukdar, S., Bae, E. J., Imamura, T., Morinaga, H., Fan, W., Li, P., Lu, W. J., Watkins, S. M. and Olefsky, J. M. (2010) GPR120 is an ω − 3 fatty acid receptor mediating potent anti-inflammatory and insulin-sensitizing effects. Cell 142, 687–698 145 Suzuki, T., Igari, S., Hirasawa, A., Hata, M., Ishiguro, M., Fujieda, H., Itoh, Y., Hirano, T., Nakagawa, H., Ogura, M. et al. (2008) Identification of G protein-coupled receptor 120-selective agonists derived from PPARγ agonists. J. Med. Chem. 51, 7640–7644 146 Newsholme, P., Curi, R., Gordon, S. and Newsholme, E. A. (1986) Metabolism of glucose, glutamine, long-chain fatty acids and ketone bodies by murine macrophages. Biochem. J. 239, 121–125 147 Newsholme, P., Costa Rosa, L. F. B. P., Newsholme, E. A. and Curi, R. (1996) The importance of fuel metabolism to macrophage function. Cell Biochem. Funct. 14, 1–10 148 Simon, L. M., Axline, S. G., Horn, B. R. and Robin, E. D. (1973) Adaptations in energy metabolism in the cultivated macrophage. J. Exp. Med. 138, 1413–1425 149 Virkamaki, A. and Yki-Jarvinen, H. (1994) Mechanisms of insulin resistance during acute endotoxemia. Endocrinology 134, 2072–2078 150 Yki-Jarvinen, H., Sammalkorpi, K., Koivisto, V. A. and Nikkila, E. A. (1989) Severity, duration, and mechanisms of insulin resistance during acute infections. J. Clin. Endocrinol. Metab. 69, 317–323 151 Agwunobi, A. O., Reid, C., Maycock, P., Little, R. A. and Carlson, G. L. (2000) Insulin resistance and substrate utilization in human endotoxemia. J. Clin. Endocrinol. Metab. 85, 3770–3778 152 Haffner, S., Temprosa, M., Crandall, J., Fowler, S., Goldberg, R., Horton, E., Marcovina, S., Mather, K., Orchard, T., Ratner, R. and Barrett-Connor, E. (2005) Intensive lifestyle intervention or metformin on inflammation and coagulation in participants with impaired glucose tolerance. Diabetes 54, 1566–1572 153 Oliver, E., McGillicuddy, F., Phillips, C., Toomey, S. and Roche, H. M. (2010) The role of inflammation and macrophage accumulation in the development of obesity-induced type 2 diabetes mellitus and the possible therapeutic effects of long-chain n − 3 PUFA. Proc. Nutr. Soc. 69, 232–243 154 Wang, T. J., Larson, M. G., Vasan, R. S., Cheng, S., Rhee, E. P., McCabe, E., Lewis, G. D., Fox, C. S., Jacques, P. F., Fernandez, C. et al. (2011) Metabolite profiles and the risk of developing diabetes. Nat. Med. 17, 448–453 155 Newgard, C. B., An, J., Bain, J. R., Muehlbauer, M. J., Stevens, R. D., Lien, L. F., Haqq, A. M., Shah, S. H., Arlotto, M., Slentz, C. A. et al. (2009) A branched-chain amino acid-related metabolic signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 9, 311–326 156 Newsholme, P. (2001) Why is L-glutamine metabolism important to cells of the immune system in health, postinjury, surgery or infection? J. Nutr. 131 (Suppl.), 2515S–2522S 157 Weichhart, T., Costantino, G., Poglitsch, M., Rosner, M., Zeyda, M., Stuhlmeier, K. M., Kolbe, T., Stulnig, T. M., Horl, W. H., Hengstschlager, M. et al. (2008) The TSC–mTOR signaling pathway regulates the innate inflammatory response. Immunity 29, 565–577 158 Sabio, G., Das, M., Mora, A., Zhang, Z., Jun, J. Y., Ko, H. J., Barrett, T., Kim, J. K. and Davis, R. J. (2008) A stress signaling pathway in adipose tissue regulates hepatic insulin resistance. Science 322, 1539–1543 159 Vallerie, S. N., Furuhashi, M., Fucho, R. and Hotamisligil, G. S. (2008) A predominant role for parenchymal c-Jun amino terminal kinase (JNK) in the regulation of systemic insulin sensitivity. PLoS ONE 3, e3151 Received 23 September 2011/15 November 2011; accepted 16 November 2011 Published on the Internet 13 February 2012, doi:10.1042/BJ20111708 c The Authors Journal compilation c 2012 Biochemical Society 160 Feuerer, M., Herrero, L., Cipolletta, D., Naaz, A., Wong, J., Nayer, A., Lee, J., Goldfine, A. B., Benoist, C., Shoelson, S. and Mathis, D. (2009) Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters. Nat. Med. 15, 930–939 161 Zhang, J. and Shi, G.-P. (2011) Mast cells and metabolic syndrome. Biochim. Biophys. Acta 1822, 14–20 162 O’Rourke, R. W., Metcalf, M. D., White, A. E., Madala, A., Winters, B. R., Maizlin, I. I., Jobe, B. A., Roberts, Jr, C. T., Slifka, M. K. and Marks, D. L. (2009) Depot-specific differences in inflammatory mediators and a role for NK cells and IFN-γ in inflammation in human adipose tissue. Int. J. Obes. 33, 978–990 163 Ohmura, K., Ishimori, N., Ohmura, Y., Tokuhara, S., Nozawa, A., Horii, S., Andoh, Y., Fujii, S., Iwabuchi, K., Onoe, K. and Tsutsui, H. (2010) Natural killer T cells are involved in adipose tissues inflammation and glucose intolerance in diet-induced obese mice. Arterioscler. Thromb. Vasc. Biol. 30, 193–199 164 Nishimura, S., Manabe, I., Nagasaki, M., Eto, K., Yamashita, H., Ohsugi, M., Otsu, M., Hara, K., Ueki, K., Sugiura, S. et al. (2009) CD8 + effector T cells contribute to macrophage recruitment and adipose tissue inflammation in obesity. Nat. Med. 15, 914–920 165 Winer, S., Chan, Y., Paltser, G., Truong, D., Tsui, H., Bahrami, J., Dorfman, R., Wang, Y., Zielenski, J., Mastronardi, F. et al. (2009) Normalization of obesity-associated insulin resistance through immunotherapy. Nat. Med. 15, 921–929 166 Ilan, Y., Maron, R., Tukpah, A. M., Maioli, T. U., Murugaiyan, G., Yang, K., Wu, H. Y. and Weiner, H. L. (2010) Induction of regulatory T cells decreases adipose inflammation and alleviates insulin resistance in ob /ob mice. Proc. Natl. Acad. Sci. U.S.A. 107, 9765–9770 167 O’Neill, L. A.J., Sheedy, F. J. and McCoy, C. E. (2011) MicroRNAs: the fine-tuners of Toll-like receptor signalling. Nat. Rev. Immunol. 11, 163–175 168 Pandey, A. K., Agarwal, P., Kaur, K. and Datta, M. (2009) MicroRNAs in diabetes: tiny players in big disease. Cell. Physiol. Biochem. 23, 221–232 169 Vickers, K. C. and Remaley, A. T. (2010) MicroRNAs in atherosclerosis and lipoprotein metabolism. Curr. Opin. Endocrinol. Diabetes Obes. 17, 150–155 170 Ley, R. E., Turnbaugh, P. J., Klein, S. and Gordon, J. I. (2006) Microbial ecology: human gut microbes associated with obesity. Nature 444, 1022–1023 171 Vijay-Kumar, M., Aitken, J. D., Carvalho, F. A., Cullender, T. C., Mwangi, S., Srinivasan, S., Sitaraman, S. V., Knight, R., Ley, R. E. and Gewirtz, A. T. (2010) Metabolic syndrome and altered gut microbiota in mice lacking Toll-like receptor 5. Science 328, 228–231 172 Brandt, C. and Pedersen, B. K. (2010) The role of exercise-induced myokines in muscle homeostasis and the defense against chronic diseases. J. Biomed. Biotechnol. 2010, 520258 173 Pedersen, B. K. (2011) Muscles and their myokines. J. Exp. Biol. 214, 337–346 174 Shaw, C. S., Clark, J. and Wagenmakers, A. J. (2010) The effect of exercise and nutrition on intramuscular fat metabolism and insulin sensitivity. Annu. Rev. Nutr. 30, 13–34 175 Pedersen, B. K., Akerstrom, T. C., Nielsen, A. R. and Fischer, C. P. (2007) Role of myokines in exercise and metabolism. J. Appl. Physiol. 103, 1093–1098 176 Beavers, K. M. and Nicklas, B. J. (2011) Effects of lifestyle interventions on inflammatory markers in the metabolic syndrome. Front. Biosci. (Schol. Ed.) 3, 168–177 177 Christ, M., Iannello, C., Iannello, P. G. and Grimm, W. (2004) Effects of a weight reduction program with and without aerobic exercise in the metabolic syndrome. Int. J. Cardiol. 97, 115–122