Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
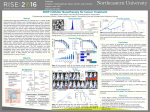
Updates in Ovarian Cancer Care Lisa McCluskey, MD Gynecologic Oncologist June 16, 2015 Compass Oncology in partnership with Ovarian Cancer Alliance of Oregon & SW Washington What is Ovarian Cancer? • The most common type of Ovarian Cancer that starts from epithelial cells –gland forming cells • Adenocarcinoma * * Other common adenocarcinomas are found in the breast, colon, lung, prostate, uterus, sometimes cervix • Other types of Ovarian Cancer start in the: »“eggs”(germ cell tumors) »body of the Ovary (stromal tumors) Who develops Ovarian Adenocarcinoma? • 15% Genetic Susceptibility known genetic susceptibility • BRCA 1 / 2, HNPCC • Lifetime risk up to 50% of developing Ovarian Cancer • 85% spontaneous somatic mutation • Lifetime risk < 2% of developing Ovarian Cancer Who develops Spontaneous Epithelial Ovarian Cancer • Risk Factors – increased age, (average age at diagnosis 63 years old) – never becoming pregnant, infertility – increased BMI > 30, – personal history of breast cancer. – Estrogen alone hormone replacement therapy • Protective – – – – – Having Tubal Ligation Hysterectomy Multiple pregnancies Pregnancy before 35 yo Birth Control Pills Different Types of Epithelial Ovarian Cancer by Histology How does Ovarian Cancer Present? • Vague Symptoms – Bloating, Distention, Changes in Bowel and Bladder Function, Pelvic / Abdominal Pain, Decreased Appetite – Symptoms persist and increase over time • >70% of women will present with • Advanced Stage Ovarian Cancer –Cancer has spread throughout the abdomen and sometimes beyond (lungs, liver) How do we treat Ovarian Cancer? • Current Approach -- Surgery and Chemotherapy • Primary Tumor Reductive Surgery (PDS) – Surgery Chemotherapy • Neoadjuvant Chemotherapy (NACT) – Chemotherapy Surgery Chemotherapy • Goal of Surgery remove all visible disease • Goal of Chemotherapy kill all cancer cells Past Significant Improvement in Ovarian Cancer Outcomes • Tumor Reductive Surgery • Optimal Tumor Reductive Surgery -- No residual cancer > 1 cm • Suboptimal – Residual Cancer > 2 cm • Chemotherapy • Intraperitoneal + Intravenous Chemotherapy • Intravenous Chemotherapy Dose-Dense • High Volume Surgeons (Gynecologic Oncologists) and High Volume Facilities • Risk Reduction by identifying women with a genetic susceptibility to ovarian cancer Important Questions at time of diagnosis • Will surgery remove all the visible cancer? • How much cancer is present to begin with? • How aggressive is the cancer? • How much skill and effort needed? • (Will chemotherapy kill the cancer?) • Is the cancer sensitive or resistant to “platinum”? How the decision is made • Assessment of Woman – Functional Status » » » » Need assistance in taking medication Limit walking less than 1 block Falls in last 6 months Fair or worse hearing – Overall Health Status and Co-morbidities » Anemia, Decreased Kidney function by blood test, » Multiple other medical problems such as Cardiovascular and Pulmonary – Cognitive Abilities – Psychological and Social Support. Assessment of the Disease • Symptoms / Physical Exam / Tumor Marker • Imaging (CT scan) • Fagotti Score –Laparoscopic Assessment – Anderson Algorithm Anticipated “Radicalness” of the Surgery • Procedures may include: • Resection of Pelvic tumor including uterus ovaries and fallopian tubes, • omentectomy • selective lymph node removal, • bowel resection, • removal of peritoneal implants, including diaphragm, • splenectomy, appendectomy Complete Tumor Resection • Surgeon knowledge, experience and skill • Biology of the Specific Cancer – Genomic signatures may be predictive – Stromal-tumor interaction appear important – TGF-beta signaling may be a therapeutic target Neoadjuvant Chemotherapy (NACT) – Chemotherapy given before surgery (usually 3 cycles) – NACT not inferior to Primary Tumor Reductive Surgery – NACT significantly improved the completeness of surgery with less residual disease at time of surgery – Less post-operative morbidity and mortality with NACT – Increased rate of Blood Transfusions Women who benefit most from NACT – Extensive Stage IIIC that is too extensive for optimal surgical resection by imaging or laparoscopic scoring – Stage IV disease (Complete Resection <10%) – Performance status too poor to undergo attempt at major surgery, particularly extensive surgery – No access to experience Gynecologic Oncology surgical team Standard of Care (SOC) Chemotherapy Carboplatin Taxol (Paclitaxel) • Intravenous • Every 3 weeks (before surgery and / or start within 6 weeks after surgery) • for 6 treatments (@ 18 weeks) • Well tolerated – (nausea, bone marrow suppression, hair loss, peripheral neuropathy, fatigue) • Not all women in US are receiving SOC Research related to 1st line Chemotherapy • • • • • Intraperitoneal Chemotherapy Dose Dense Chemotherapy Possible additional agents (disease response / toxicity) Changes in the Staging and Histology Classification System Changes in Research Endpoint Definitions. • Research continues to show that the most significant influence in outcome is stage of disease and completeness of surgical resection. Recurrent Ovarian Cancer is a Chronic Disease Process • For most women who are diagnosed with ovarian cancer, the cancer will recur and the cancer becomes a chronic disease. – Over 70% of all women diagnosed with ovarian cancer will have recurrent disease. • Good news is that women are living longer with better quality of life with recurrent ovarian cancer. – Better control of the cancer with newer treatment options Swanton Cancer Tree Model Treatment of Recurrent Cancer • Timing of Recurrence • Platinum Resistance vs Platinum Sensitivity • Prior Chemotherapy Treatments • Goal is Quality of Life and Longevity • Treatment Options • Chemotherapy • Surgery (selective cases) • New Treatment Options such as biologic therapies Definitions of Disease State • Cure (completely eradicate all cancer cells) • Recurrent Ovarian Cancer – Asymptomatic – Biochemical – Measurable Disease • After Treatment »Complete Response »Partial Response »Stable Disease »Progression Definition of Longevity • Overall Survival • Time from diagnosis to death • Progression Free Interval/ Survival – Interval between Treatment Response to Evidence of Progression • How is Progression defined? – – – – Biochemical - CA125 Imaging -- CT / PET Physical Exam Increased Symptoms Treatment Goals • Optimal Response for Disease State at that time – Control of Tumor Growth • Quality of Life -- Acceptable Toxicity – Decreased symptoms of disease – Acceptable Toxicities from Treatment • Clinical Trials • Phase I – Acceptable toxicity • Phase II – Cancer response to treatment • Phase III – New treatment better than prior treatment Treatment Approaches • Chemotherapy – kill cancer cells as they replicate • Biologic Therapies – Alter how the cancer cell is able to function and replicate • Radiation Therapy – rarely used in ovarian cancer http://www.genome.jp/kegg-bin/show_pathway?hsa05200 Subway Cancer Pathway Complexity of Cancer Cell Function Treatment Approaches – Complex Cancer Function / Process may make eradicating cancer more difficult, but also gives multiple options / approaches to treatment. – Identifying the complex processes at the • GENETIC • CELLULAR • MOLECULAR Levels – What turns on or off the cancer controls Cancer Cell Function which may be altered Treatment Strategies related to Cancer Function Molecular Profiling • Identifying abnormalities in an individual person’s cancer that may be altered in a that cancer. – Less about the ‘type’ of cancer and more about specific functions of the cells • Usually are able to obtain a massive amount of information for very small fragments of the tumor. • Different methods – examples --DNA Sequencing, Microscopic Staining • Currently in ovarian cancer there are few findings that are “actionable”– cancer treatments available targeted at a specific abnormality PARP Poly ADP-ribose polymerase (DNA Repair Enzyme) • Healthy cells undergo replication. Cancer cells replicate quickly and often. – Sometimes there are breaks or mistakes in the duplication of the DNA to form new cells. – Healthy cells are able to activate a couple of different DNA repair pathways. One of these pathways is regulated by a PARP enzyme. • When there a defect in the BRCA 1 or 2 gene (gene mutation) – The ”other” DNA repair pathways doesn’t work. – DNA repair pathways is dependent on PARP enzyme to repair the DNA. – If the PARP action is blocked (by a PARP Inhibitor) then the PARP pathways is also will not function. There is no “back-up” repair system. – If the DNA can’t repair itself, it can’t replicate—leading to cell death and replication is stopped. Olaparib—(PARP Inhibitor) • Blocks a the PARP-associated DNA Repair Pathway – Particularly effective when there is a BRCA mutation • Oral drug • Well tolerated – Common Side Effects • Nausea, fatigue, vomiting, diarrhea, affects take and digestion • Bone Marrow Suppression (increased risk infection, bleeding , anemia) • Rare serious toxicity leukemia, lung inflammation Olaparib—(PARP Inhibitor) Olaparib Combination of Testing and Treatment • FDA accelerated Approval – 12-19-2014 (accelerated approval) • 1st Laboratory Development Testing –Companion Diagnostic / Treatment Package • Myriad Genetic Laboratories »BRACAnalysis CDx™ • Astra-Zeneca Pharmaceuticals »Lynparza™ –> Olaparib (PARP inhibitor) Criteria for Testing / Treatment • FDA approved for women who have received three or more chemotherapy treatments for ovarian cancer. – Not approved for anyone who is has a BRCA mutation – Initial Diagnosis and 2 separate recurrences – FDA did not approve olaparib for maintenance treatment. • Insurance is likely to pay for drug if a woman meets criteria above, but may not otherwise • Estimated cost is @$7000 / month Other PARP-Inhibitors • Veliparib • Rucaparib • Niraparib Angiogenesis Inhibitors Blocks the growth of blood vessels in a tumor, starving the cancer of the nutrition and oxygen it needs to survive. Bevavizumab (Avastin) • Angiogenesis Inhibitor – One of the first ‘biologic’ treatments for ovarian cancer – Effective in several other cancers (colon, breast, lung) • Intravenous every 2-3 weeks • Limited side effects (symptoms) but significant potential toxicities (risk to health) • Research related to Ovarian Cancer • “1st line” Ovarian Cancer Treatment • Maintenance Treatment • Recurrent Disease Cediranib • Angiogenesis Inhibitor – a potent inhibitor of vascular endothelial growth factor receptor tyrosine kinases • Oral • Similar Side Effects of Olaparib – Fatigue, Nausea, diarrhea, hypertension Combination of Olaparib and Cediranib Based on Phase II Study • Combined treatment vs monotherapy – Tumors shrank more dramatically – Greater delayed progression (compared to standard chemotherapy) – More complete remission with combination • (5 women in combination group and 2 women in monotherapy group) Combination Treatment better than Olaparib Alone by 7 months Combination Treatment increased progression free survival 3 months in women with BRCA mutation 10 months in women without BRCA mutation New Targeted Therapies • • • • • • • • Bevacizumab (Avastin) Bortezomib (Velcade) Ceritinib (Zykadia) Ipilimumab (Yervoy) Nivolumab (Opdivo) Olaparib (Lynparza) Pazopanib (Votrient) Pembrolizumab (Keytruda) • Pertuzumab (Perjeta) • Temsirolimus (Torisel) • Trametinib (Mekinist) • • • • • • • • • Trebananib Veliparib Rucaparib Avelumab Binimetinib Niraparib VB-111 Vanucizumab Selinexor New Cancer Targets • Cancer Cell Resistance to treatment – Platinum sensitive versus Platinum Resistance • Cellular immunity pathways • • • • Checkpoint Inhibitors Stromal Interaction with cancer Enhance Anti-Cancer Immune Systems Vaccines – – FANG individualized vaccine against the original ovarian cancer cells. • Monoclonal Antibodies • Testing drugs that have been approved for other types of cancer (melanoma, breast) Other Research Areas • Why all women do not receive the Standard of Care – and making changes in systems • Development of Biomarkers • Stratification of Treatments to Individual Tumor • Changing combinations of treatments – adding additional treatment to already proven regimens • Identifying women with genetic mutations so that risk reducing options can be offered • Quality of Life – Management of Toxicities of Treatment – Palliative Care—symptom Management – Survivorship Programs Conclusion: Where we are at in Cancer Therapies?