Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Myocardial infarction wikipedia , lookup
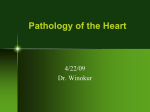
Clinical Science (2013) 125, 291–300 (Printed in Great Britain) doi: 10.1042/CS20120612 Decreased Nox4 levels in the myocardium of patients with aortic valve stenosis Marı́a U. MORENO∗ , Idoia GALLEGO∗ , Begoña LÓPEZ∗ , Arantxa GONZÁLEZ∗ , Ana FORTUÑO∗ , Gorka SAN JOSÉ∗ , Félix VALENCIA†, Juan José GÓMEZ-DOBLAS†, Eduardo DE TERESA†, Ajay M. SHAH‡, Javier DÍEZ∗ § and Guillermo ZALBA∗ ∗ Division of Cardiovascular Sciences, Centre for Applied Medical Research, University of Navarra, Avda. Pı́o XII 55, 31008 Pamplona, Spain †Division of Cardiology, Vı́rgen de la Victoria University Hospital, Campus Universitario de Teatinos, s/n. 29010 Málaga, Spain ‡Cardiovascular Division, King’s College London British Heart Foundation Centre of Excellence, Denmark Hill Campus, 125 Coldharbour Lane, London SE5 9NU, U.K. §Department of Cardiology and Cardiac Surgery, University Clinic, University of Navarra, Avda. Pı́o XII, 36, 31008 Pamplona, Spain Abstract The NADPH oxidases are a key family of ROS (reactive oxygen species)-producing enzymes which may differentially contribute to cardiac pathophysiology. Animal studies show uncertain results regarding the regulation of cardiac Nox4 by pressure overload and no data are available on human myocardial Nox4. In the present study, we evaluated Nox4 expression and its relationship with myocardial remodelling and LV (left ventricular) function in patients with severe AS (aortic valve stenosis). Endomyocardial biopsies from 34 patients with AS were obtained during aortic valve replacement surgery. LV morphology and function were assessed by echocardiography. Myocardial samples from subjects deceased of non-CVDs (cardiovascular diseases) were analysed as controls. Nox4 localization was evaluated by immunohistochemistry and quantified by Western blot. Myocardial capillary density, fibrosis and cardiomyocyte dimensions and apoptosis were assessed histologically to evaluate myocardial remodelling. Nox4 was present in samples from all subjects and expressed in cardiomyocytes, VSMCs (vascular smooth muscle cells), endothelium and fibroblasts. Nox4 levels were reduced 5-fold in AS patients compared with controls (P < 0.01). Nox4 levels directly correlated with cardiomyocyte cross-sectional area (r = 0.299, P<0.05) and diameter (r = 0.406, P < 0.05) and capillary density (r = 0.389, P < 0.05), and inversely with cardiomyocyte apoptosis (r = − 0.316, P < 0.05) in AS patients. In addition, Nox4 levels correlated with echocardiographic parameters (LV ejection fraction: r = 0.353, P < 0.05; midwall fractional shortening: r = 0.355, P < 0.05; deceleration time: r = − 0.345, P < 0.05) in AS patients. Nox4 is expressed in human myocardium and reduced in AS patients. The observed associations of Nox4 with cardiomyocyte parameters and capillary density in AS patients suggest a potential role of Nox4 deficiency in the myocardial remodelling present in the human pressure-overloaded heart. Key words: aortic valve stenosis, myocardial remodelling, NADPH oxidase, Nox4, pressure overload INTRODUCTION AS (aortic valve stenosis) is the most common valve disease in developed countries, affecting 2–3 % of the population over 65 years, and its prevalence is likely to rise in the future because it increases with advancing age [1]. Chronic pressure overload in AS patients induces a structural remodelling of the LV (left ventricular) myocardium characterized by alterations of cardiomyocytes, the extracellular matrix and the coronary microcirculation, which contributes to LV functional impairment [2,3]. Oxidative stress is implicated in the development of myocardial remodelling [4]. ROS (reactive oxygen species) contribute at the molecular level to alter cardiac structure and function, damaging macromolecules and altering redox-sensitive signalling pathways, thus contributing to myocardial remodelling [4,5]. Although there are multiple cardiac sources of ROS, the NADPH oxidase family of enzymes is the only one whose primary role is ROS generation. In general terms, they consist of a distinct catalytic subunit (Nox1–5, Duox1–2), usually bound to the smaller p22phox subunit, and have varying regulation depending upon Abbreviations: AngII, angiotensin II; AS, aortic valve stenosis; AU, arbitrary units; CVF, collagen volume fraction; eNOS, endothelial nitric oxide synthase; LV, left ventricular; LVEF, LV ejection fraction; LVMI, LV mass index; Nrf2, nuclear factor-erythroid 2-related factor 2; NT-pro-BNP, amino-terminal propeptide of brain natriuretic peptide; Poldip2, polymerase (DNA-directed) delta-interacting protein 2; ROS, reactive oxygen species; TBST, Tris-buffered saline with 1 % (v/v) Tween 20; VSMC, vascular smooth muscle cell; vWF, von Willebrand factor. Correspondence: Dr Maria U. Moreno (email [email protected]) or email Dr Guillermo Zalba (email [email protected]). www.clinsci.org 291 M. U. Moreno and others the isoform [6]. Nox4 requires the association of p22phox and is constitutively active [6–8], although its activity is increased by Poldip2 [polymerase (DNA-directed) delta-interacting protein 2] in VSMCs (vascular smooth muscle cells) [9]. Several reports indicate that Nox4 predominantly generates H2 O2 [7,8]. In human cells, there is in vitro evidence of Nox4 expression in microvascular endothelial cells [10], cardiac fibroblasts [11] and coronary artery smooth muscle cells [12]. Regarding the modulation of Nox4 expression in experimental cardiac pressure overload, there is no undisputable evidence. Studies in mice subjected to suprarenal constriction show no changes in Nox4 protein levels [13], an increase in Nox4 mRNA levels [14] or an increase in Nox4 protein levels [15]. Models of pressure overload by thoracic aortic constriction report an increase in cardiac Nox4 mRNA [16] or Nox4 protein levels [17]. Currently, there is no information regarding the myocardial localization of Nox4 in humans or of changes of its levels in pressure overload. Therefore the aim of the present study was to evaluate the presence of Nox4 in the myocardium of patients with pressure overload due to AS and assess the associations of Nox4 with myocardial remodelling and LV morphology and function. MATERIALS AND METHODS Study population All patients gave written, informed consent to participate in the present study. The study was carried out in accordance with the Helsinki Declaration and the Ethics Committee of the Vı́rgen de la Victoria University Hospital (Málaga, Spain) approved the protocol. The study population consisted of 34 patients with clinically diagnosed severe isolated AS, defined in accordance with the following criteria [18]: mean transvalvular pressure gradient 40 mmHg, aortic valve area <1 cm2 or aortic valve area index <0.6 cm2 /m2 . The patients were referred for valve replacement due to the presence of characteristic clinical symptoms (i.e. angina, syncope or heart failure manifestations) and/or LVEF (LV ejection fraction) <50 %. Patients with cardiac valve disease other than AS and/or history of acute myocardial infarction were excluded after complete medical examination. Heart failure was clinically diagnosed on the basis of the presence of at least one major and two minor Framingham criteria [19] and was reinforced by either echocardiographic signs of systolic dysfunction (LVEF <50 %) or by the presence of elevated levels of the NT-pro-BNP (Nterminal propeptide of brain natriuretic peptide) and alterations in cardiac morphology and function indicative of heart failure with normal ejection fraction according to the European Society of Cardiology [20]. Cardiac samples were collected from 18 subjects who had died from non-cardiovascular-related diseases, nine of which were processed for protein studies [six men and three women, average age 54 (range 46–62) years] and nine processed for histomorphological studies [six men and three women, average age 59 (range 40–68) years], to be used as controls. 292 C The Authors Journal compilation C 2013 Biochemical Society Echocardiographic assessment Two-dimensional echocardiographic imaging, targeted M-mode recordings, and Doppler ultrasound measurements were obtained in each AS patient. LV mass was measured from M-mode recordings according to the American Society of Echocardiography criteria [21], and LVMI (LV mass index) was calculated by dividing LV mass by the body surface area. The presence of LV hypertrophy was established when the LVMI was >149 g/m2 for men and >122 g/m2 for women [22]. The presence of concentric LV hypertrophy was established when relative wall thickness was >0.42 [22]. LV midwall fractional shortening and ejection fraction were calculated according to the method of Quinones et al. [23]. The following pulsed Doppler measurements were obtained: maximal early transmitral diastolic velocity, maximal late transmitral diastolic velocity, the deceleration time of the early mitral filling wave and the isovolumic relaxation time. Mean and maximal transvalvular pressure gradient and aortic valve area were assessed in all patients. Myocardial sampling During surgical aortic valve replacement two endomyocardial biopsies were taken from the interventricular septum. The biopsy procedure was well tolerated in all cases and no complications were recorded. The first sample, for molecular studies, was divided into two pieces, immediately frozen in liquid nitrogen and processed for mRNA and for protein extraction. The second sample was processed for histomorphological and immunohistochemical studies. The biopsies were taken from adjacent areas, so that they were equivalent. The average biopsy size was 21 + −2 mm3 . Histomorphological and immunohistochemical studies After formalin fixation, the biopsies were embedded in paraffin and serially sectioned in 4-μm-thick sections. In all the cases, the endogenous peroxidase was inactivated by 30 min incubation in 0.01 % H2 O2 in methanol. Slides were blocked in 20 % (v/v) normal goat serum (Dako) for 30 min. Primary antibodies used were Nox4 (sc-30141 diluted 1:100; SantaCruz Biotechnology), noncommercial Nox4 [14] (diluted 1:100), Poldip2 (ab85364 diluted 1:200; Abcam) and vWF (von Willebrand factor) (A0082 diluted 1:250; Dako). Immunohistochemistry to confirm cell type was performed in serial sections with antibodies against vWF (to detect endothelium), α and β myosin heavy chain (to detect cardiomyocytes) (Ab15 diluted 1:400; Abcam), smooth muscle α-actin (to detect smooth muscle cells) (A5228 diluted 1:400 Sigma) or vimentin (to detect fibroblasts) (sc-6260 diluted 1:500; Santa Cruz Biotechnology). Secondary antibodies were Envision anti-rabbit or anti-mouse, as appropriate, incubated for 30 min. Signal was detected by 3,3 -DAB (diaminobenzidine) (Dako). Slides were counterstained with Harris haematoxylin (Sigma). Negative controls were carried out with primary antibody omission. Cardiac capillarization was quantified in sections by immunohistochemistry against vWF. Images were captured at ×20 magnification with an Eclipse 80i microscope (Nikon) and the average capillary number was calculated from six fields. Cardiac Decreased Nox4 in human aortic stenosis capillarization was calculated as the number of capillaries per area (capillaries/mm2 ) and the capillary-to-cardiomyocyte ratio (by dividing the number of capillaries present in each field by the number of cardiomyocyte nuclei present in each field). Collagen was identified by Picrosirius Red staining and quantified as described previously [24], which allowed us to calculate the area occupied by collagen [CVF (collagen volume fraction)]. Cell apoptosis was assessed by TUNEL (terminal deoxynucleotidyltransferase-mediated dUTP nick-end labelling) as described previously [25]. Cardiomyocyte mean cross-sectional diameter and area were assessed in Masson’s trichrome-stained sections, captured at ×40 magnification, with the AnalySIS 3.1 software (Soft Imaging System). Quantification of Nox4 immunostaining was carried out by quantitative morphometry with an automated image analysis system (AnalySYS; Soft Imaging System). Biochemical determinations Venous blood samples were obtained in each patient from the left antecubital vein. The NT-pro-BNP was measured in plasma samples by an ELISA method (Biomedica Gruppe) [26]. Protein studies Protein was extracted in lysis buffer [7 mol/l urea, 2 mol/l thiourea, 4% (w/v) CHAPS and 1% (w/v) DTT (dithiothreitol)] and quantified (Pierce BCA Protein Assay Kit; Thermo Scientific). Then, 10 μg of the protein homogenate were mixed with adequate volumes of Laemmli buffer and subjected to SDS/PAGE (10 % gel). Gels were blotted on to nitrocellulose membranes (Hybond ECL; GE Healthcare). Membranes were then washed in TBST [Tris-buffered saline with 1% (v/v) Tween 20] for 5 min at room temperature (22 ◦ C) and incubated in blocking solution [5% (w/v) non-fat dried skimmed milk powder in TBST] for 2 h at room temperature. Afterwards, the blots were incubated with the primary antibody in blocking solution [Nox4: sc-30141 diluted 1:1000 (Santa Cruz Biotechnology); and Poldip2: ab85364 diluted 1:1000 (Abcam)] overnight at 4 ◦ C with slow rocking. The blots were then washed five times for 5 min in TBST and incubated with an HRP (horseradish peroxidase)-conjugated secondary antibody in blocking solution. After washing five times for 5 min in TBST, bands were identified by chemiluminescence with the ECL Advanced kit (GE Healthcare). The membranes were stripped using Restore Western Blot Stripping Buffer (Pierce) according to instructions and reblotted for α-tubulin (sc-5286 diluted 1:10000). Band intensities were quantified with the MultiAnalyst software (Bio-Rad Laboratories). Data are expressed as AU (arbitrary units) relative to α-tubulin levels. The specificity of the Nox4 band was confirmed with a noncommercial antibody against Nox4 (diluted 1:2000) that had been validated using Nox4-transfected cells and Nox4-knockout mice as positive and negative controls respectively [14,27]. Table 1 Clinical characteristics of the patients Results are expressed as means + − S.E.M or percentage of subjects. V E /V A , maximal early transmitral diastolic velocity/maximal late transmitral diastolic velocity ratio. Parameter Patients (n = 34) 71 + −1 Age (year) Sex (male/female) (n) 10/24 28.2 + − 0.9 120 + −3 69 + −1 Body mass index (kg/m2 ) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg) Hypertension (%) 71 Diabetes mellitus (%) 35 Coronary artery disease (%) 35 Heart failure (%) 56 Atrial fibrillation (%) 32 Treatment (%) Warfarin 21 Diuretics 70 Digitalis 9 Angiotensin-converting enzyme inhibitors 18 AngII type1 receptor antagonists 15 β-Blockers 36 Aldosterone antagonists 6 Ca2 + antagonists 18 Aortic valve area (cm2 ) Aortic valve area index (cm2 /m2 ) Mean transvalvular pressure gradient (mmHg) Maximal transvalvular pressure gradient (mmHg) LVMI (g/m2 ) Relative wall thickness Concentric LV hypertrophy (%) LVEF (%) LV midwall fractional shortening (%) End-systolic wall stress (kdyn/cm2 ) V E /V A Isovolumic relaxation time (ms) Deceleration time (ms) NT-pro-BNP (fmol/ml) 0.63 + − 0.04 0.38 + − 0.02 53.45 + − 2.89 82.24 + − 4.37 147.7 + − 7.5 0.612 + − 0.025 58 66.15 + − 2.84 38.96 + − 1.91 59.66 + − 4.28 1.05 + − 0.18 97.73 + − 7.37 291.24 + − 20.50 829 + − 72 spectrophotometer). Retrotranscription of 1 μg of total RNA was carried out with random hexamers and Superscript III (Invitrogen). Quantification of the cDNA was performed by Real time PCR with TaqMan probes (4333760F for 18S, Applied Biosystems) and SYBR green technology (Promega) with primers 5 -GTGGCTGTCTGCATGGACCT-3 and 5 CCACGATGGTGACTTTGGCT-3 for eNOS (endothelial nitric oxide synthase) in an ABI Prism 7000 Sequence Detection System (Applied Biosystems). Data are expressed as AU relative to the 18S ribosomal RNA. Statistical analysis RNA studies Extraction of total RNA was performed with TRIzol® (Invitrogen) according to the manufacturer’s instructions. RNA quantity and quality were assessed by absorbance (Ultraspec Results are expressed as means + − S.E.M. Differences between the groups were evaluated using a Student’s t test for unpaired data or Mann–Whitney U test, as appropriate after evaluating normality (Shapiro–Wilks test). Correlations between continuously www.clinsci.org 293 M. U. Moreno and others Figure 1 Myocardial Nox4 expression Nox4 was detected in myocardial biopsies from controls and AS patients, with a lower intensity in the latter. (A) Myocardium from a control subject, Nox4 staining (left) and immunohistochemistry negative control (right) (×10 magnification). (B) Myocardium from a patient with AS, Nox4 staining (left) and immunohistochemistry negative control (right) (×10 magnification). distributed variables were tested by bivariate association and univariate and multivariate regression analysis. A P value <0.05 was considered statistically significant. Analyses were performed with the SPSS 15.0 statistical package. capillary-to-cardiomyocyte ratio (1.18 + − 0.08 compared with + 0.15; P < 0.001). Patients showed greater CVF than con2.63 − trols (17.33 + − 1.90 % compared with 1.95 + − 0.07 %; P < 0.001). Nox4 and Poldip2 expression RESULTS Characteristics of patients The clinical characteristics of patients are summarized in Table 1. Around half of them had clinical heart failure and almost onethird exhibited atrial fibrillation. Myocardial remodelling Compared with controls, patients had increased cardiomyocyte cross-sectional area (498.48 + − 95.91 compared with 2 203.09 + − 0.44 − 17.36 μm ; P < 0.001) and diameter (26.13 + compared with 16.61 + − 0.69 μm; P < 0.001). The cardiomyocyte apoptotic index was increased in patients compared with controls (0.101 + − 0.016 compared with 0.0045 + − 0.0 016 %; P < 0.001). The cardiac capillary density was reduced in patients compared with controls, whether calculated as the capillaries/mm2 (522 + − 48 compared with 1531 + − 78; P < 0.001) or the 294 C The Authors Journal compilation C 2013 Biochemical Society Detection of Nox4 by immunohistochemistry showed that it is expressed in the human heart, both in controls and AS patients, although with greater stained area in controls (23.3 + − 2.2 compared with 9.5 + 2.5 %; P < 0.01) (Figure 1). Serial immunohistoche− mistry with cell-type markers confirmed the expression of Nox4 in cardiomyocytes, VSMCs, endothelial cells and fibroblasts, both in controls and in AS patients (Figure 2). In cardiomyocytes, Nox4 staining was present in the cytoplasm and some nuclei (Figure 3A). Quantification in cardiac homogenates showed that Nox4 protein levels were 5-fold lower in AS patients than in controls (0.48 + − 0.03 compared with 2.45 + − 0.50 AU; P < 0.01) (Figure 3B). We observed in patients that Nox4 levels were higher in women than in men (0.50 + − 0.04 compared with 0.34 + − 0.02 AU; P < 0.05). However, there were no differences in Nox4 levels between patients without (n = 14, 0.437 + − 0.057 AU) and with (n = 20, 0.502 + 0.036 AU) LV hypertrophy, between − patients without (n = 20, 0.508 + 0.046 AU) and with heart − failure (n = 14, 0.428 + 0.037 AU), between patients without − Decreased Nox4 in human aortic stenosis Figure 2 Co-expression of Nox4 and cell-type markers Serial immunohistochemical staining of Nox4 and cell-type markers α- and β-myosin heavy chain for cardiomyocyte (×20 magnification), vWF for endothelium (×40 magnification), α-actin for vascular smooth muscle (×40 magnification) and vimentin for fibroblasts (×100 magnification) showed that Nox4 was expressed in these cell types in myocardial samples from (A) controls and (B) patients with AS (n = 23, 0.482 + − 0.045 AU) and with (n = 11, 0.461 + − 0.030 AU) arrhythmias, between patients without (n = 22, 0.459 + − 0.037 AU) and with (n = 12, 0.505 + − 0.061 AU) coronary artery disease, between patients without (n = 10, 0.457 + − 0.055 AU) and with (n = 24, 0.483 + 0.039 AU) hypertension, or between pa− tients without (n = 22, 0.471 + 0.039 AU) and with (n = 12, − 0.482 + 0.057 AU) diabetes. There were no differences in Nox4 − levels between patients taking medications interfering with the renin–angiotensin–aldosterone system (n = 13, 0.498 + − 0.041 AU) and those who were not taking such medication (n = 20, 0.462 + − 0.047 AU), or between patients under statin treatment (n = 21, 0.451 + − 0.031 AU) and those who were not (n = 12, 0.521 + 0.072 AU). − In addition, we assessed Poldip2, a regulator of Nox4 activity [9]. Immunohistochemical studies showed that it was expressed in the human heart, in the cytoplasm and nucleus of cardiomyocytes (Figure 3C). Quantification in homogenates showed that Poldip2 expression was 8-fold lower in AS patients than in controls (0.29 + − 0.02 compared with 2.33 + − 0.51 AU; P < 0.01) (Figure 3D). Association studies Nox4 levels directly correlated with the cardiomyocyte crosssectional area (Figure 4A) and diameter (Figure 4B) in AS patients. Furthermore, Nox4 levels correlated inversely with the apoptotic index in AS patients (Figure 4C). There was a direct correlation between Nox4 levels and the degree of capillary density expressed as the capillary-to-cardiomyocyte ratio (Figure 4D) in AS patients. These associations were independent of age, sex and the severity of AS (transvalvular gradient and valve area). Nox4 levels did not correlate with the CVF (r = − 0.181, P = not significant). It has been proposed that Nox4 may regulate eNOS expression and contribute to vessel generation [28,29]. We observed in AS patients that Nox4 levels directly correlated with the mRNA levels of eNOS (r = 0.402, P < 0.05). www.clinsci.org 295 M. U. Moreno and others Figure 3 Localization of Nox4 and Poldip2 within the myocardium (A) Immunohistochemistry of Nox4 in patients with AS. Nox4 was detected mainly in cardiomyocyte cytoplasm and some nuclei (arrows) (left, ×10 magnification; right, ×40 magnification). (B) Representative Western blot images and histograms quantifying Nox4 in homogenates. Nox4 expression was lower in patients with AS than in controls. (C) Immunohistochemistry of Poldip2 in patients with AS. Poldip2 was detected in cardiomyocyte cytoplasm, by the plasma membrane (dotted arrows) and some nuclei (closed arrows) (left, ×10 magnification; right, ×40 magnification). (D) Representative Western blot images and histograms quantifying Poldip2 in homogenates. Poldip2 expression was lower in patients with AS than in controls. ∗ P<0.01. Nox4 levels correlated with echocardiographic parameters in AS patients. Nox4 levels directly correlated with the LVEF (Figure 5A) and the LV midwall fractional shortening (Figure 5B) and inversely with the deceleration time (Figure 5C). These associations were independent of age, sex and the severity of AS (transvalvular gradient and valve area). Poldip2 levels did not correlate with Nox4 levels, parameters of myocardial remodelling or parameters of cardiac function. DISCUSSION The main novel findings of our study are the following: (i) Nox4 is expressed in human cardiac cells; (ii) Nox4 levels are abnormally decreased in patients with severe AS; (iii) Nox4 levels are associated with alterations in parameters assessing myocardial structure in AS patients; and (iv) Nox4 levels are associated with parameters of LV systolic and diastolic function in these patients. Taken together, these results suggest that Nox4 deficiency may contribute to the remodelling of the myocardium present in human cardiac pressure overload. In the present study, we provide the first data on the expression of Nox4 in the human myocardium. Regarding its localization, we detected Nox4 expression in cardiomyocytes, as well as in VSMCs, endothelial cells and fibroblasts, 296 C The Authors Journal compilation C 2013 Biochemical Society in both controls and AS patients. These data expand previous observations in animal studies showing Nox4 expression in cardiac cells [30]. Moreover, we observed Nox4 in both the cytoplasm and the nucleus of cardiomyocytes, supporting data from other studies identifying Nox4 in the nuclei [31] and cellular organelles {i.e. ER (endoplasmic reticulum [30,32] and mitochondria [17,30]}. Currently, there is conflicting evidence on the myocardial changes of Nox4 in experimental pressure overload, with studies showing no changes in Nox4 protein levels [13], an increase in Nox4 mRNA levels [14,16], or an increase in Nox4 protein levels [15,17]. Surprisingly, our data indicate that patients with pressure overload secondary to AS present a marked reduction of myocardial Nox4 levels compared with controls. Nox4 seems to be modulated by a number of factors that may also be of relevance for myocardial remodelling in the setting of pressure overload, for instance, AngII (angiotensin II) [30,33]. Although some authors have shown that AngII administration decreases Nox4 expression in VSMCs [34], others failed to show any effect [35], and yet others reported increased Nox4 expression in VSMCs [36] and endothelial cells [37]. In this regard, no relationship was found between Nox4 expression and the treatment with drugs interfering with the renin–angiotensin–aldosterone system in the patients from the present study. In addition, down-regulation of Nox4 expression in the vasculature has been reported following Decreased Nox4 in human aortic stenosis Figure 4 Correlations of Nox4 with parameters assessing myocardial remodelling Myocardial Nox4 expression correlated with (A) the cardiomyocyte cross sectional area (y = 103.6x + 434.59), (B) the cardiomyocyte cross-sectional diameter (y = 6.6682x + 23.335), (C) the cardiomyocyte apoptotic index (y = − 0.0988x + 0.1252) and (D) the capillary-to-cardiomyocyte ratio (y = 0.9479x + 0.7299) in patients with AS. pathophysiological shear stress [38,39], although the potential contribution of this factor to reduced Nox4 expression in the myocardium of AS patients remains to be investigated. Nox4 seems to be constitutively active [7] and thus Nox4 levels may be a good indicator of the Nox4-dependent NADPH oxidase activity. In addition, we also evaluated the levels of Poldip2, an enhancer of Nox4 activity [9]. We identified for the first time that Poldip2 is expressed in human myocardium and that Poldip2 levels were lower in AS patients than in controls, thus suggesting that besides reduced Nox4 availability, the activity of the enzyme dependent on this factor may also be reduced in the myocardium of AS patients. Several findings reported in the present study deal with the potential consequences of Nox4 deficiency. On the one hand, we find an association between reduced Nox4 levels and decreased capillarization in patients with AS. This mirrors the data from Zhang et al. [14] showing that cardiac Nox4 overexpression is associated with increased capillary density in mice subjected to pressure overload. Craige et al. [28] demonstrated that an augmented endothelial Nox4 expression promotes angiogenesis in an eNOS-dependent manner, which was recently corroborated by Schröder et al. [29] in a study on the role of endogenous Nox4 during ischaemic or AngII-induced stress. In this regard, we have detected in AS patients an association between reduced Nox4 levels and decreased eNOS mRNA expression. Thus, it can be hypothesized that Nox4 deficiency contributes to diminished capillarization via reduced eNOS availability among other mechanisms in the myocardium of AS patients. On the other hand, we detect an association between reduced Nox4 levels and reduced cardiomyocyte hypertrophy and increased cardiomyocyte apoptosis. It is known that H2 O2 may determine cardiomyocyte fate, either death (apoptosis) or survival (hypertrophy), in a dosedependent manner [40–42], with the involvement of Nrf2 (nuclear factor-erythroid 2-related factor 2) and antioxidants [41,43]. Interestingly, Brewer et al. [44] in cardiomyocytes and Schröder et al. [29] in blood vessels, showed that Nox4 contributes to the antioxidant defences via the Nrf2 transcription factor, supporting a beneficial role of Nox4. In this conceptual framework, it can be suggested that reduced Nox4 may contribute to the cardiomyocyte alterations seen in AS patients. Some considerations suggest that the association of Nox4 with myocardial remodelling reported in the present study may be of potential pathophysiological relevance. First, there is evidence of reduced capillarization in AS [45] and of its negative impact on cardiac function [46,47]. Similarly, there is evidence of increased apoptosis in AS, which is associated with the preoperative functional class and valve-replacement postoperative outcome [48]. These findings fit well with our results showing that Nox4 levels are associated with parameters of LV systolic and diastolic function, suggesting that reduced Nox4 levels may contribute to the functional alterations of the left ventricle in AS patients. Several limitations of our study must be acknowledged. First, this is a clinical study involving relatively small amounts of tissue obtained from patients, making it difficult to undertake an extensive range of analyses as would be possible in an animalbased study. Secondly, we studied AS patients at the time of www.clinsci.org 297 M. U. Moreno and others r r In the present study, we provide novel information on cardiac Nox4 in humans. In particular, our findings suggest that a decrease in Nox4 levels is associated with myocardial remodelling in patients with severe AS. Although descriptive in nature, these findings set the stage for future investigations to assess the role of Nox4 in the development and progression of myocardial remodelling in human cardiac pressure overload, as well as to explore its modulation as a potential therapeutic target to prevent myocardial remodelling. AUTHOR CONTRIBUTION Marı́a Moreno, Javier Dı́ez, Guillermo Zalba conceived, designed, analysed and interpreted the data, drafted and revised the paper critically for important intellectual content, and gave final approval. Idoia Gallego, Begoña López and Arantxa González conceived, designed, analysed and interpreted the data, and revised the paper critically for important intellectual content and gave final approval. Ana Fortuño, Gorka San José, Félix Valencia, Juan Gómez-Doblas, Eduardo de Teresa and Ajay Shah revised the paper critically for important intellectual content and gave final approval. ACKNOWLEDGEMENTS We gratefully acknowledge the technical assistance of Idoia Rodrı́guez, Ana Montoya, Sonia Martı́nez and Marı́a González. FUNDING Figure 5 Correlation of Nox4 with cardiac function Myocardial Nox4 expression correlated with (A) ejection fraction (y = 31.769x + 51.056), (B) midwall fractional shortening (y = 20.499x + 29.079) and (C) deceleration time (y = − 1.5546x + 3.5834) in patients with AS. valve replacement, hence we lack information regarding the progression of the disease. Thus, although novel and valuable, the information provided in the present study regarding Nox4 expression is rather a snapshot of the late state of the valve disease. In addition, the study involved a relatively small number of patients, but because of the nature of the aims of the study, the design was appropriate. Moreover, we are aware that patients were under treatment, which may influence the results, although Nox4 levels did not seem to be influenced by therapy. Finally, as there was no material available for mRNA studies in controls, we could not evaluate if the decrease in Nox4 levels in AS patients was due to decreased Nox4 transcription. This study was supported through the agreement between the Foundation for Applied Medical Research and ‘UTE project CIMA’, the Ministry of Economy and Competitiveness [grant numbers RECAVA RD06/0014/0008, SAF-2010-20367, RYC-2010-05797 (to A.G.)], the European Union [MEDIA project grant HEALTH-F2-2010261409], the British Heart Foundation and a Foundation Leducq Transatlantic Network of Excellence award (to A.M.S.). REFERENCES 1 2 3 CLINICAL PERSPECTIVES r 298 NADPH oxidases are a key family of ROS-producing enzymes, but there is currently no information regarding the presence of Nox4 in the myocardium of patients with pressure overload due to aortic valve stenosis (AS) or changes in its levels during pressure overload. C The Authors Journal compilation C 2013 Biochemical Society 4 5 Lindroos, M., Kupari, M., Heikkila, J. and Tilvis, R. (1993) Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J. Am. Coll. Cardiol. 21, 1220–1225 Hein, S., Arnon, E., Kostin, S., Schonburg, M., Elsasser, A., Polyakova, V., Bauer, E. P., Klovekorn, W. P. and Schaper, J. (2003) Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation 107, 984–991 Schwartzkopff, B., Frenzel, H., Dieckerhoff, J., Betz, P., Flasshove, M., Schulte, H. D., Mundhenke, M., Motz, W. and Strauer, B. E. (1992) Morphometric investigation of human myocardium in arterial hypertension and valvular aortic stenosis. Eur. Heart J. 13, 17–23 Seddon, M., Looi, Y. H. and Shah, A. M. (2007) Oxidative stress and redox signalling in cardiac hypertrophy and heart failure. Heart 93, 903–907 Takimoto, E. and Kass, D. A. (2007) Role of oxidative stress in cardiac hypertrophy and remodeling. Hypertension 49, 241–248 Decreased Nox4 in human aortic stenosis 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Bedard, K. and Krause, K. H. (2007) The NOX family of ROS-generating NADPH oxidases: physiology and pathophysiology. Physiol. Rev. 87, 245–313 Nisimoto, Y., Jackson, H. M., Ogawa, H., Kawahara, T. and Lambeth, J. D. (2010) Constitutive NADPH-dependent electron transferase activity of the Nox4 dehydrogenase domain. Biochemistry 49, 2433–2442 Takac, I., Schroder, K., Zhang, L., Lardy, B., Anilkumar, N., Lambeth, J. D., Shah, A. M., Morel, F. and Brandes, R. P. (2011) The E-loop is involved in hydrogen peroxide formation by the NADPH oxidase Nox4. J. Biol. Chem. 286, 13304–13313 Lyle, A. N., Deshpande, N. N., Taniyama, Y., Seidel-Rogol, B., Pounkova, L., Du, P., Papaharalambus, C., Lassegue, B. and Griendling, K. K. (2009) Poldip2, a novel regulator of Nox4 and cytoskeletal integrity in vascular smooth muscle cells. Circ. Res. 105, 249–259 Montezano, A. C., Burger, D., Paravicini, T. M., Chignalia, A. Z., Yusuf, H., Almasri, M., He, Y., Callera, G. E., He, G., Krause, K. H. et al. (2010) Nicotinamide adenine dinucleotide phosphate reduced oxidase 5 (Nox5) regulation by angiotensin II and endothelin-1 is mediated via calcium/calmodulin-dependent, rac-1-independent pathways in human endothelial cells. Circ. Res. 106, 1363–1373 Cucoranu, I., Clempus, R., Dikalova, A., Phelan, P. J., Ariyan, S., Dikalov, S. and Sorescu, D. (2005) NAD(P)H oxidase 4 mediates transforming growth factor-beta1-induced differentiation of cardiac fibroblasts into myofibroblasts. Circ. Res. 97, 900–907 Sorescu, D., Weiss, D., Lassegue, B., Clempus, R. E., Szocs, K., Sorescu, G. P., Valppu, L., Quinn, M. T., Lambeth, J. D., Vega, J. D. et al. (2002) Superoxide production and expression of nox family proteins in human atherosclerosis. Circulation 105, 1429–1435 Byrne, J. A., Grieve, D. J., Bendall, J. K., Li, J. M., Gove, C., Lambeth, J. D., Cave, A. C. and Shah, A. M. (2003) Contrasting roles of NADPH oxidase isoforms in pressure-overload versus angiotensin II-induced cardiac hypertrophy. Circ. Res. 93, 802–805 Zhang, M., Brewer, A. C., Schroder, K., Santos, C. X., Grieve, D. J., Wang, M., Anilkumar, N., Yu, B., Dong, X., Walker, S. J. et al. (2010) NADPH oxidase-4 mediates protection against chronic load-induced stress in mouse hearts by enhancing angiogenesis. Proc. Natl. Acad. Sci. U.S.A. 107, 18121–18126 Henderson, B. C., Sen, U., Reynolds, C., Moshal, K. S., Ovechkin, A., Tyagi, N., Kartha, G. K., Rodriguez, W. E. and Tyagi, S. C. (2007) Reversal of systemic hypertension-associated cardiac remodeling in chronic pressure overload myocardium by ciglitazone. Int. J. Biol. Sci. 3, 385–392 Mohammed, S. F., Ohtani, T., Korinek, J., Lam, C. S., Larsen, K., Simari, R. D., Valencik, M. L., Burnett, Jr, J. C. and Redfield, M. M. (2010) Mineralocorticoid accelerates transition to heart failure with preserved ejection fraction via ‘nongenomic effects’. Circulation 122, 370–378 Ago, T., Kuroda, J., Pain, J., Fu, C., Li, H. and Sadoshima, J. (2010) Upregulation of Nox4 by hypertrophic stimuli promotes apoptosis and mitochondrial dysfunction in cardiac myocytes. Circ. Res. 106, 1253–1264 Bonow, R. O., Carabello, B. A., Chatterjee, K., de Leon, Jr, A. C., Faxon, D. P., Freed, M. D., Gaasch, W. H., Lytle, B. W., Nishimura, R. A., O’Gara, P. T. et al. (2008) Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 118, e523–e661 Ho, K. K., Pinsky, J. L., Kannel, W. B. and Levy, D. (1993) The epidemiology of heart failure: the Framingham Study. J. Am. Coll. Cardiol. 22, 6A–13A 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 Paulus, W. J., Tschope, C., Sanderson, J. E., Rusconi, C., Flachskampf, F. A., Rademakers, F. E., Marino, P., Smiseth, O. A., De Keulenaer, G., Leite-Moreira, A. F. et al. (2007) How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur. Heart J. 28, 2539–2550 Sahn, D. J., DeMaria, A., Kisslo, J. and Weyman, A. (1978) Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation 58, 1072–1083 Lang, R. M., Bierig, M., Devereux, R. B., Flachskampf, F. A., Foster, E., Pellikka, P. A., Picard, M. H., Roman, M. J., Seward, J., Shanewise, J. et al. (2006) Recommendations for chamber quantification. Eur. J. Echocardiogr. 7, 79–108 Quinones, M. A., Pickering, E. and Alexander, J. K. (1978) Percentage of shortening of the echocardiographic left ventricular dimension. Its use in determining ejection fraction and stroke volume. Chest 74, 59–65 López, B., González, A., Querejeta, R., Larman, M. and Dı́ez, J. (2006) Alterations in the pattern of collagen deposition may contribute to the deterioration of systolic function in hypertensive patients with heart failure. J. Am. Coll. Cardiol. 48, 89–96 González, A., Lóez, B., Ravassa, S., Querejeta, R., Larman, M., Dı́ez, J. and Fortuño, M. A. (2002) Stimulation of cardiac apoptosis in essential hypertension: potential role of angiotensin II. Hypertension 39, 75–80 González, A., López, B., Querejeta, R., Zubillaga, E., Echeverrı́a, T. and Dı́ez, J. (2010) Filling pressures and collagen metabolism in hypertensive patients with heart failure and normal ejection fraction. Hypertension 55, 1418–1424 Anilkumar, N., Weber, R., Zhang, M., Brewer, A. and Shah, A. M. (2008) Nox4 and Nox2 NADPH oxidases mediate distinct cellular redox signaling responses to agonist stimulation. Arterioscler. Thromb. Vasc. Biol. 28, 1347–1354 Craige, S. M., Chen, K., Pei, Y., Li, C., Huang, X., Chen, C., Shibata, R., Sato, K., Walsh, K. and Keaney, Jr, J. F. (2011) NADPH Oxidase 4 promotes endothelial angiogenesis through endothelial nitric oxide synthase activation. Circulation 124, 731–740 Schröder, K., Zhang, M., Benkhoff, S., Mieth, A., Pliquett, R., Kosowski, J., Kruse, C., Ludike, P., Michaelis, U. R., Weissmann, N. et al. (2012) Nox4 is a protective reactive oxygen species generating vascular NADPH oxidase. Circ. Res. 110, 1217–1225 Lassegue, B., San Martin, A. and Griendling, K. K. (2012) Biochemistry, physiology, and pathophysiology of NADPH oxidases in the cardiovascular system. Circ. Res. 110, 1364–1390 Kuroda, J., Nakagawa, K., Yamasaki, T., Nakamura, K., Takeya, R., Kuribayashi, F., Imajoh-Ohmi, S., Igarashi, K., Shibata, Y., Sueishi, K. et al. (2005) The superoxide-producing NAD(P)H oxidase Nox4 in the nucleus of human vascular endothelial cells. Genes Cells 10, 1139–1151 Zhang, L., Nguyen, M. V., Lardy, B., Jesaitis, A. J., Grichine, A., Rousset, F., Talbot, M., Paclet, M. H., Qian, G. and Morel, F. (2011) New insight into the Nox4 subcellular localization in HEK293 cells: first monoclonal antibodies against Nox4. Biochimie 93, 457–468 Yamazaki, T. and Yazaki, Y. (1999) Role of tissue angiotensin II in myocardial remodelling induced by mechanical stress. J. Hum. Hypertens. 13 (Suppl. 1), S43–S47 Lassegue, B., Sorescu, D., Szocs, K., Yin, Q., Akers, M., Zhang, Y., Grant, S. L., Lambeth, J. D. and Griendling, K. K. (2001) Novel gp91phox homologues in vascular smooth muscle cells: nox1 mediates angiotensin II-induced superoxide formation and redox-sensitive signaling pathways. Circ. Res. 88, 888–894 www.clinsci.org 299 M. U. Moreno and others 35 36 37 38 39 40 41 Wosniak, Jr, J., Santos, C. X., Kowaltowski, A. J. and Laurindo, F. R. (2009) Cross-talk between mitochondria and NADPH oxidase: effects of mild mitochondrial dysfunction on angiotensin II-mediated increase in Nox isoform expression and activity in vascular smooth muscle cells. Antioxid. Redox Signaling 11, 1265–1278 Wingler, K., Wunsch, S., Kreutz, R., Rothermund, L., Paul, M. and Schmidt, H. H. (2001) Upregulation of the vascular NAD(P)H-oxidase isoforms Nox1 and Nox4 by the renin-angiotensin system in vitro and in vivo. Free Radical Biol. Med. 31, 1456–1464 Alvarez, E., Rodino-Janeiro, B. K., Ucieda-Somoza, R. and Gonzalez-Juanatey, J. R. (2010) Pravastatin counteracts angiotensin II-induced upregulation and activation of NADPH oxidase at plasma membrane of human endothelial cells. J. Cardiovasc. Pharmacol. 55, 203–212 Hwang, J., Ing, M. H., Salazar, A., Lassegue, B., Griendling, K., Navab, M., Sevanian, A. and Hsiai, T. K. (2003) Pulsatile versus oscillatory shear stress regulates NADPH oxidase subunit expression: implication for native LDL oxidation. Circ. Res. 93, 1225–1232 Goettsch, C., Goettsch, W., Arsov, A., Hofbauer, L. C., Bornstein, S. R. and Morawietz, H. (2009) Long-term cyclic strain downregulates endothelial Nox4. Antioxid. Redox Signaling 11, 2385–2397 Seenarain, V., Viola, H. M., Ravenscroft, G., Casey, T. M., Lipscombe, R. J., Ingley, E., Laing, N. G., Bringans, S. D. and Hool, L. C. (2010) Evidence of altered guinea pig ventricular cardiomyocyte protein expression and growth in response to a 5 min in vitro exposure to H2 O2 . J. Proteome Res. 9, 1985–1994 Oyama, K., Takahashi, K. and Sakurai, K. (2009) Cardiomyocyte H9c2 cells exhibit differential sensitivity to intracellular reactive oxygen species generation with regard to their hypertrophic vs death responses to exogenously added hydrogen peroxide. J. Clin. Biochem. Nutr. 45, 361–369 42 43 44 45 46 47 48 Kwon, S. H., Pimentel, D. R., Remondino, A., Sawyer, D. B. and Colucci, W. S. (2003) H2 O0 regulates cardiac myocyte phenotype via concentration-dependent activation of distinct kinase pathways. J. Mol. Cell. Cardiol. 35, 615–621 Gupta, M. K., Neelakantan, T. V., Sanghamitra, M., Tyagi, R. K., Dinda, A., Maulik, S., Mukhopadhyay, C. K. and Goswami, S. K. (2006) An assessment of the role of reactive oxygen species and redox signaling in norepinephrine-induced apoptosis and hypertrophy of H9c2 cardiac myoblasts. Antioxid. Redox Signaling 8, 1081–1093 Brewer, A. C., Murray, T. V., Arno, M., Zhang, M., Anilkumar, N. P., Mann, G. E. and Shah, A. M. (2011) Nox4 regulates Nrf2 and glutathione redox in cardiomyocytes in vivo. Free Radical Biol. Med. 51, 205–215 Rakusan, K., Flanagan, M. F., Geva, T., Southern, J. and Van Praagh, R. (1992) Morphometry of human coronary capillaries during normal growth and the effect of age in left ventricular pressure-overload hypertrophy. Circulation 86, 38–46 Rajappan, K., Rimoldi, O. E., Dutka, D. P., Ariff, B., Pennell, D. J., Sheridan, D. J. and Camici, P. G. (2002) Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation 105, 470–476 Tsagalou, E. P., Anastasiou-Nana, M., Agapitos, E., Gika, A., Drakos, S. G., Terrovitis, J. V., Ntalianis, A. and Nanas, J. N. (2008) Depressed coronary flow reserve is associated with decreased myocardial capillary density in patients with heart failure due to idiopathic dilated cardiomyopathy. J. Am. Coll. Cardiol. 52, 1391–1398 Gaudino, M., Anselmi, A., Abbate, A., Galiuto, L., Luciani, N., Glieca, F. and Possati, G. (2007) Myocardial apoptosis predicts postoperative course after aortic valve replacement in patients with severe left ventricular hypertrophy. J. Heart Valve Dis. 16, 344–348 Received 13 November 2012/27 March 2013; accepted 4 April 2013 Published as Immediate Publication 4 April 2013, doi: 10.1042/CS20120612 300 C The Authors Journal compilation C 2013 Biochemical Society