Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
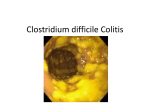
Clostridium Dr.Batool Clostridium difficile 1- Pathogen disease causing Pseudomembranous Colitis 2- Habitats (gastrointestinal tract of Humans and other animals, Soils, Marine Sediments). 3- Target Area of Infection: Colon 4- The mortality rate is 1 to 2.5%. Virulence factors: 1- Enterotoxin (Toxin A): - Causing diarrhea: Protein toxin released by C. difficile in the lower Intestine. - Alters the permeability of the epithelial cells of the intestinal wall. - Pore forming toxins, secreted by bacteria, form pores in cell membranes causing cells death. 2- Cytotoxin (Toxin B). - kill cells. - Associated with inflammation. Pathogenesis: 1- Toxigenic strains produce 2 large protein exotoxins that are associated with virulence (Toxins A and B) 2- Mutants strains that do not make toxins A and B are not virulent. 3-Some strains make a third toxin known as Binary Toxin by itself, not pathogenic may act synergistically with toxins A and B in severe colitis (More common in animal strains). C. difficile which secretes two types of toxin (A and B), which cause disruption to the barrier function of the colonic mucosa. They are cytotoxic to cells of the intestinal tract, B being about 1,000 times more potent than A. Transmission of infection is via an indirect faeco-oral route, through spores left on surfaces. The spores can survive for months and patients can become carriers. The risk of colonization increases with length of hospital stay. 1 Clostridium Dr.Batool Pseudomembranous colitis (PMC) is an acute, exudative colitis usually caused by Clostridium difficile. PMC can rarely be caused by other bacteria - eg, Staphylococcus spp. or enterotoxigenic Clostridium perfringens, Campylobacter spp., Listeria spp. and Salmonella spp. C difficile colonization results in a wide spectrum of clinical conditions, including an asymptomatic carrier state; mild, selflimited diarrhea; pseudomembranous colitis; and fulminant colitis. Most patients develop diarrhea during or shortly after starting antibiotics. However, 25-40% of patients asymptomatic for 10 weeks after completing antibiotic therapy. PMC has emerged, particularly in recent years, as a major and very expensive health care problem. Spores formed by the organism are implicated in spread of infection and have implications for hygiene and prevention of infection. C. difficile is an anaerobic Gram-positive rod Symptoms: Mild to moderate watery diarrhea that is rarely bloody. Cramping abdominal pain Anorexia and Malaise Fever, especially in more severe cases. Treatment: 1- C. difficile sometimes resolves in two to three days after you have stopped taking antibiotics. 2- It can also be treated with other antibiotics, such as vancomycin and Flagyle. The strain of C. difficile that produces a large amount of toxin is harder to treat. What increases my risk for acquiring C. difficile? •Taking antibiotics •Having surgery •Being in a health care facility for an extended period of time •Having serious, underlying illness 2 Clostridium Dr.Batool •Advanced age Role of Antibiotics: • All antibiotics (including metronidazole and vancomycin) are associated with CDI. • High-risk group – Clindamycin – Cephalosporins/penicillins/beta-lactams. – Fluoroquinolones. • Alteration of normal colonic flora thought to favor growth of C. difficile Infection Control: 1- Wash hands with warm soap and water. 2- Mechanical removal of spores. 3- Alcohol does not kill spores 4- Stool is pre-treated with alcohol when growing C. difficile 5- Contact and barrier precautions 6- Antibiotic stewardship Clostridium botulinum 1-Gram positive 2-Obligate anaerobic bacillus. 3-Motile. 4-Spores (ubiquitous, Resistant to heat, light, drying and radiation, specific conditions for germination, anaerobic conditions, warmth (10-50 C),Mild alkalinity. 5- Clostridium botulinum is widely distributed in soil and contaminated fruits and vegetables. Inadequate precautions in processing and handling of a certain food will allow this organism to grow and produce one of the most powerful exotoxins known. Transmission: 1234- Ingestion (organism, spores, neurotoxin) Wound contamination Inhalation Person-to-person not documented. 3 Clostridium Dr.Batool Virulence factors (exotoxin, neurotoxin): There are seven antigenic varieties of toxin(A-G) are known: 1- A,B,E and F are the principle causes of human illness. 2- Type E predominantly with fish products. 3- Type C and D are associated with animal diseases. Action of botulism toxin: It is a neurotoxic protein. All of its types (A, B, and E) are made of heavy and light chains linked by disulfide bonds. The heavy chain is thought to bind the toxin to the motor nerve end. The light chain blocks the calcium mediated release of acetyl choline. The toxin acts by blocking the release of acetyl choline at synapses and neuromuscular junctions causing flaccid paralysis. Pathogenesis: -Three forms are fatal and need to a medical emergency -Incubation period: 12-36 hours 1- Wound Botulism Organism enters wound Develops under anaerobic conditions, From ground-in dirt or gravelIt does not penetrate intact skin Associated with addicts of black-tar heroin. 2- Food borne Botulism Preformed toxin ingested from contaminated food(most common from home-canned foods (green beans, beets, corn, garlic, tomatoes; type A Improperly fermented fish (Alaska); type E 3 Infant Botulism Infants < 1 year old, 94% < 6 months old Spores from varied sources Honey, food, dust, corn syrup 4 Clostridium Dr.Batool Diagnosis:- Demonstration of toxins in serum from the patient and toxin may be found in left food. Treatment: 1- Trivalent antitoxin(A,B,E,F toxin must be administrated intravenously. 2- Adequate ventilation These will reduce mortality rate from 65 % to below25%. 3- Infant botulism is recovered with supportive therapy alone. Control: 1-Boiling of home canned food for 20 minutes to destroy the toxin. 2-Strict regulation of commercial canning. 3- Avoiding swelled canned food or that with suspected appearance or odor. References: 1- Jawetz, Melnick, & Adelberg’s.( 2013). Medical Microbiology (Twenty-Sixth Edition). 2- Kenneth Todar. (2008).Todar’s Online Textbook of Bacteriology ,University of Wisconsin. 3- Ray, C.G., ed. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. 5