Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
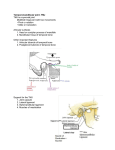
DIAGNOSTIC IMAGING OF TEMPEROMANDIBULAR JOINT Introduction The temporomandibular joint, or TMJ, is the articulation between the condyle of the mandible and the squamous portion of the temporal bone. The condyle is elliptically shaped with its long axis oriented mediolaterally. The articular surface of the temporal bone is composed of the concave articular fossa and the convex articular eminence. Normal Anatomy Osseous structures Glenoid fossa Articular eminence Mandibular condyle Post-glenoid tubercle Normal Anatomy Soft tissue components Disk Joint capsule Synovia Lateral ligament Upper and lower joint spaces Normal Disk Position When the mouth opens, two distinct motions occur at the joint. The first motion is rotation around a horizontal axis through the condylar heads. The second motion is translation. The condyle and meniscus move together anteriorly beneath the articular eminence. In the closed mouth position, the thick posterior band of the meniscus lies immediately above the condyle. As the condyle translates forward, the thinner intermediate zone of the meniscus becomes the articulating surface between the condyle and the articular eminence. When the mouth is fully open, the condyle may lie beneath the anterior band of the meniscus Imaging The decision to image is made after evaluation of patient history, clinical findings, and in some cases response to conservative treatment Hard tissue imaging OPG Plain films- TMJ views, SMV and conventional tomography Specialized- CT, Nuclear medicine Soft tissue imaging Arthrography MRI Plain Films in TMJ Disorders Transcranial Transorbital Transpharyngeal Others Submentovertex Reverse Towne’s Lateral oblique TRANSCRANIAL PROJECTION:(Lindblom technique) Lateral aspect of TMJ well visualized. Central / medial part of TMJ not clearly seen- since xray beam is not target to these articular surfaces. This disadvantage partly compensated because of most of early osseous changes occurs laterally in joint. TECHNIQUE AND POSITIONING: MAIN INDICATIONS: TMJ pain dysfunction syndrome and internal derangement of joint producing pain, clicking, limitation in opening. To investigate size and position of disc this can only be inferred indirectly from relative position of bony elements of joints. To investigate range of movement in joint. TMJ Transcranial DIAGNOSTIC INFORMATION: Information provided by closed view includes: This provides indirect information about position and shape of disc. (Joint space radiologically refers to radiolucent zone between condylar head and glenoid fossa, which includes disc and upper /lower anatomical joint spaces.) Position of head of condyle within fossa Shape and condition of glenoid fossa a articular eminence (on lateral aspect only). Shape of head of condyle and condition of articular surface. (On lateral aspect only) A comparison of both sides. INFORMATION PROVIDED BY OPEN VIEW INCLUDES: Range and type of movement of condyle. Comparison of degree of movement on both sides. TRANS PHARYNGEAL: (Infra cranial TMJ projection, Parma, Mc Queen projection) MAIN INDICATIONS: TMJ pain dysfunction syndrome. To investigate presence of joint disease particularly Osteoarthritis & Rheumatoid arthritis. To investigate pathological conditions affecting condylar head, including cysts or tumors. fracture of neck and head of condyle. Sup surface of condyle visualized. TRANS ORBITAL PROJECTION: (ZIMMER) TECHNIQUE AND POSITIONING: Conventional frontal TMJ projection is most routinely successful in delineating joint with minimal super imposition is transorbital (ZIMMER) projection, also called Transmaxillary Projection. Advantage- Lack of major superimposition over most of condylar process. Productions of relatively true “enface” frontal projection of condyle (directing central ray perpendicular to long axis of condyle) and simplicity with which it is made. Patient positioning- TMJ- Transorbital Panoramic Imaging Shows significant erosion, sclerosis, or osteophyte Probable fracture diagnosis Little info on articular eminence or fossa Good initial examination Some pan machines have TMJ programs MAIN INDICATIONS: TMJ pain dysfunction syndrome. To investigate disease within joint. To investigate pathological condition affecting condylar head. Fracture of condylar head or neck. Condylar hypo/hyperplasia. DIAGNOSTIC INFORMATION: It gives information of shape of condylar heads and condition of articular surfaces from lateral aspect. Direct comparison of both condylar heads. Some panaromic machines can give closed and open view of condyle is not of information. Two views of condyle at maximum opening will reflect maximum translation from initial closed position, it will maximize information and minimize patient absorbed x-ray dose. Condylar hyperplasia: note elongated right condyle Condylar hyperplasia: note relatively elongated left mandibular condyle. Mandibular condylar hypoplasia: The left condyle is smaller and altered in shape in comparison with the right. R Osseous ankylosis (arrowheads) between coronoid process and zygomatic arch. Metallic sutures are from a previous trauma-related operation. Others SMV Reverse towne’s Lateral oblique SUBMENTOVERTEX PROJECTION Projection show base of the skull, sphenoidal sinuses and facial skeleton from below This view helps ruling out TMJ erosion from nasopaharygeal carcinoma extending to base of skull. Also be used to define angulations of condyle in transverse plane of skull. REVERSE TOWNE’S MAIN INDICATIONS: To investigate articular surface of condyle and disease within joint. Fracture of condylar head and neck (especially medially displaced fracture of condyle) Condylar hypo/hyperplasia. TECHNIQUE: USES To know the Shape of condylar heads and condition of articular surface from posterior aspect. A direct comparison of both condyles. Lateral Oblique Projection Tomography MAIN INDICATIONS: Estimation of joint space, examination of condylar surface from medical to lateral pole for arthritic changes, visualization of condylar translation, visualization of articular eminence changes. It helps in assessment of whole of joint to determine presence and site of any bone disease or abnormality. To investigate condyle and articular fossa, when patient unable to open mouth. Assessment of fracture in the articular fossa and intra capsular space. Tomography in Coronal Plane provides information about medial and lateral poles of condyle, which is not adequately depicted on sagittal tomograms. Osseous structures Condylar position Used along with arthrography Disadvantage of Tomography is large irradition dose delivered to lens of eye. Types Linear tomogram Multidirectional Hypocycolloidal tomogram Multi-Computer Controlled Spiral tomogram DIAGNOSTIC INFORMATION: to know Size of joint space. Position of head of condyle within fossa. Shape of head of condition of articular surface including medial and lateral aspects. Shape and condition of articular fossa and eminence. Information on all aspects of joint. Position and orientation of fracture fragment. Body section tomography provides most definitive radiologic information about TMJ. Complex motion tomography (hypocycloidal) /spiral motion) is superior to transcranial radiography for demonstrating changes on articulating surface and position of condyle within mandibular fossa. An initial SMV projection required to measure angles of each condyle within information patient head may be oriented correctly for performing Tomography examination Tomographic section of TMJ made in 2 orientations with respect to joint With head positioned so that section is at right angle to long axis of condyle (the lateral tomographic section.) Often with section parallel to long axis of condyle (frontal tomographic section) A proper tomographic examination is comprised of from 4-7section at 2-3 mm intervals. Tube and film move in opposite direction, and rotate about a fulcrum Focal plain The level of the fulcrum is the focal plain TMJ - Tomograms Tomograms TMJ osteoarthrosis Conventional tomogram: Joint “space” is thinned because of loss of articular cartilage. Anterior osteophyte is composed of dense cortical bone and articular eminence (E) is eburnated. CT Scan CT permits the imaging of thin slices of tissues in a wide variety of planes, and provide axial, coronal and sagittal plane Slices thickness-10mm-body and brain 5mm- H&N 3D recon- 1-1.5mm Images viewed- bone windowing and soft tissue windowing Scan images are composed of picture elements(pixels) Hounsfield scale-’0’HU(water), -1000HU(air), TMJ-sagittal projection-most suitable Radiation dose- less than that of tomography or arthrotomography Sagittal Coronal Axial Indications Not for soft tissue changes Evaluation of trauma and tumors Perforation of alloplastic grafts into cranial fossa Volume averaging Accuracy and limitations Normal Flattening MRI Uses electrical and magnetic fields and radiofrequency No assoc radiologic risk and non-invasive Soft tissues are imaged directly C/I: Claustrophobia pts not tolerated, pts with metallic vascular clips, metallic implants and pacemakers Disk location and displacement (~ 95% accuracy) Osseous details poor Soft tissue changes Fluid or joint effusion Protocol dependant MRI Parameters TR TE Term Effect Short Short T1 Anatomy –excellent Disk -low intensity Long Long T2 Poor anatomy Joint effusion – high intensity Relative Brightness of Tissues Fat Marrow Brain Muscle Body fluid TMJ disk Cortical bone Air white gray black Normal T1-weighted MRI of TMJ (TR450,TE20) Closed mouth Condyle (C); Glenoid fossa (F); Articular eminence (E); Anterior band (A); Posterior band (P). Normal T1-weighted MRI of TMJ (TR450,TE20) Open mouth Condyle (C); Glenoid fossa (F); Articular eminence (E); Anterior band (A); Posterior band (P). Note classic “bowtie” appearance of disk. Arthrography Temporuniandibular arthrography utilizes the injection of radiopaque material into on or both of the joint compartments to enhance the contrast between the disc and spaces. The shape and position of the disc are then inferred from the shapes of opacities above and below it. Single and double contrast Indication Internal derangements Disk perforation As a therapy? Arthrocentesis Contraindication Infection Contrast sensitivity Atthrographic evidence of perforation is seen fluoroscopically during injection of the contrast medium into the lower joint compartment. The radiopaque material can be seen flowing into the upper joint space, and injection of this compartment becomes unnecessary. Arthrography: Technique Clinical exam and history Informed consent Asepsis and anesthesia Contrast agents Injecting the contrast material under fluoroscope Translation of condyle A 25 or 23 gauge needle is placed into the inferior joint space immediately posterior to the condyle. Small amounts of iodinated contrast are injected under fluoroscopy. The contrast tracks along the posterior, superior and anterior portions of the condyle. The anterior collection of contrast, called the anterior recess, normally has a smooth, tear-drop shape. If the meniscus is perforated, contrast flows into both the superior and inferior joint recesses. However, the arthrographic needle can inadvertently puncture the meniscus and cause iatrogenic filling of both joint spaces. As the condyle translates anteriorly, the contrast usually empties from the anterior recess and flows posteriorly. When the meniscus is anteriorly displaced, the anterior recess becomes abnormally elongated. Often the displaced meniscus is deformed or buckled, which results in a mass effect against the contrast in the anterior recess. As the condyle translates anteriorly, the mass effect against the anterior recess often increases. When the meniscus reduces, the anterior recess returns to a normal appearance. If the meniscus does not reduce, the anterior recess remains deformed in the fully open mouth position. R/Gs POST-OP INST Scout Tomogram Osseous structures Disk space Sclerotic changes Opacification of Lower Space Open Position Translation of condyle Reduction of disk Protruded Position Closed mouth Open mouth Normal TMJ arthrogram Intermediate zone (Z) lies in narrowest part of joint condyle (C) and articular eminence (E). The anterior (A) and posterior (P) bands occupy the wider part of the joint. Glenoid fossa (F). Usually, in an arthrogram of a normal TMJ, little contrast medium appears anterior to the condyle in the closed mouth position and this volume is further reduced in the opened mouth position. Throughout the range of motion, the posterior band remains behind the condyle, the anterior band remians ahead, and the thin intermediate zone remains between the two functional surfaces.