Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epigenetics of human development wikipedia , lookup
Genome evolution wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Gene expression programming wikipedia , lookup
Designer baby wikipedia , lookup
Segmental Duplication on the Human Y Chromosome wikipedia , lookup
Medical genetics wikipedia , lookup
Genomic imprinting wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Down syndrome wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Genome (book) wikipedia , lookup
Y chromosome wikipedia , lookup
X-inactivation wikipedia , lookup
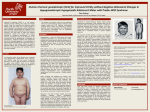
Annales de Génétique 47 (2004) 267–273 www.elsevier.com/locate/anngen Case Report Prader-Willi syndrome with an unusually large 15q deletion due to an unbalanced translocation t(4;15) Monica C. Varela, Graziela M. P. Lopes, Celia P. Koiffmann * Centro de Estudos do Genoma Humano, Departamento de Biologia, Instituto de Biociências, Universidade de São Paulo, São Paulo, SP, Brazil Received 29 November 2003; accepted 23 January 2004 Available online 12 March 2004 Abstract Prader-Willi syndrome (PWS) is a neurobehavioral disorder caused by deletions in the 15q11-q13 region, by maternal uniparental disomy of chromosome 15 or by imprinting defects. Structural rearrangements of chromosome 15 have been described in about 5% of the patients with typical or atypical PWS phenotype. An 8-year-old boy with a clinical diagnosis of PWS, severe neurodevelopmental delay, absence of speech and mental retardation was studied by cytogenetic and molecular techniques, and an unbalanced de novo karyotype 45,XY,der(4)t(4;15)(q35;q14),-15 was detected after GTG-banding. The patient was diagnosed by SNURF-SNRPN exon 1 methylation assay, and the extent of the deletions on chromosomes 4 and 15 was investigated by microsatellite analysis of markers located in 4qter and 15q13-q14 regions. The deletion of chromosome 4q was distal to D4S1652, and that of chromosome 15 was located between D15S1043 and D15S1010. Our patient’s severely affected phenotype could be due to the extent of the deletion, larger than usually seen in PWS patients, although the unbalance of the derivative chromosome 4 cannot be ruled out as another possible cause. The breakpoint was located in the subtelomeric region, very close to the telomere, a region that has been described as having the lowest gene concentrations in the human genome. © 2004 Elsevier SAS. All rights reserved. Keywords: Prader-Willi syndrome; Unbalanced translocation; Absence of speech © 2004 Elsevier SAS. All rights reserved. doi:10.1016/j.anngen.2004.01.003 268 M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 1. Introduction Prader-Willi syndrome (PWS; MIM 176 270) is characterized by neonatal hypotonia with poor sucking and failure to thrive in the postnatal period, delayed psychomotor development, hyperphagia in early childhood resulting in severe obesity, as well as short stature in adolescents, small hands and feet, hypogonadism, mild to moderate mental retardation, temper tantrums, and obsessive-compulsive mannerisms [17,8,4,7]. The incidence of this syndrome has been estimated at 1/15-20,000 [4]. PWS results from the loss of expression of at least 7 paternal imprinted genes mapped to the chromosome region 15q11-q13 [15]. Three different genetic mechanisms can lead to the PWS phenotype, the main one being a paternal deletion of the 15q11-q13 region, which accounts for about 65-75% of the cases [11,12]. Approximately 20-25% of the patients present maternal uniparental disomy (UPD) [13], and about 5% have a mutation in the imprinting center [2]. Most deletions are interstitial, but approximately 5% of the patients have a de novo unbalanced structural rearrangement involving the proximal 15q region and telomere ends of several other chromosomes [3,19,9]. We report herein on a PWS patient with severe mental retardation and absence of speech, who has an unusually large 15q11-q13 deletion, caused by an unbalanced translocation t(4q;15q). Studies by FISH, SNURF-SNRPN exon 1 methylation assay and microsatellite genotyping were performed to characterize the extent of the deletion and to attempt to correlate it with the severity of his phenotype. 2. Case report The patient, an 8 year-old boy, was the first child born to non-consanguineous, healthy parents when the mother was 32 and the father 35 years of age. After 5 months of gestation, fetal movements decreased. He was born at term by caesarian section, due to abnormal fetal position; his birth weight was 2500g and his length was 50cm. He presented severe neonatal hypotonia with poor sucking, absence of crying, and respiratory distress. Hyperphagia and obesity began at the age of 1 year and 6 months, and he could walk at 4 years and 6 months. At the age of 8 years (Figure 1), he had severe mental retardation, did not speak at all, and presented behavioral problems such as temper tantrums and stubbornness. He had a narrow bitemporal diameter, low-set ears, strabismus and hypogonadism with bilateral cryptorchidism. His weight was 45kg (>97th centile), height 1.22m (25th centile), and head circumference 53.5cm (98<p<50th centile). His foot length was 13.5cm (<3rd centile), and his whole hand measurement was 14cm (25th centile). He was unable to write or read, and had a deficiency in communicating, socializing and every-day living skills. He also presented high pain and vomiting thresholds, and skin picking. * Corresponding author: C.P. Koiffmann, Departamento de Biologia, Instituto de Biociências, USP, Caixa Postal 11.461, CEP: 05422-970, São Paulo, SP, Brazil. Phone: +55 11 3031 4304 Fax: +55 11 3091 7553;. E-mail address: [email protected] (C.P. Koiffmann). M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 269 Fig. 1. The patient at ages: a) 8 years; b) 8 years and 4 months. Fig. 2. a) G-banded partial karyotype showing normal chromosome 4, der(4), normal chromosome 15 and normal pair 5. b) FISH with D15S11 (red) / D15Z1 (green) probe, showing the normal chromosome 15 (arrow) and deletion of the PWS/AS region within chromosome der(4) (arrow t). 3. Results The patient’s karyotype after GTG-banding was 45,XY,der(4)t(4;15)(q35;q14),-15 (Figure 2a), and FISH analysis with probe D15S11/CEP15-D15Z1 (Vysis) confirmed the 270 M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 Fig. 3. A schematic diagram showing the position of deletion breakpoints observed in ~95% of PWS and AS patients (zigzag lines [5,6]); the breakpoint in our patient and in the patients described by Matsumura et al. (2003) and Windpassinger et al., (2003) (bars); genes and relevant markers mapped to 15q11-q13 (circles). deletion of the PWS/AS region on the der(4) chromosome (Figure 2b). Both parents had normal karyotypes. The patient’s diagnosis was confirmed by methylation analysis of the SNURF-SNRPN exon 1 gene amplified by PCR [24], which showed the typical pattern of PWS. Microsatellite genotyping with markers mapped to 4qter and to the segment 15q11q14 indicated the extent of the deletions in both chromosomes (4 and 15): the 4q deletion was distal to D4S1652 (which maps to 4q35.2-qter), and the 15q deletion was located between D15S1043 and D15S1010 (Figure 3). 4. Discussion Our patient had all the striking features of PWS, such as hypotonia, poor sucking and failure to thrive in the postnatal period, delayed psychomotor development, hyperphagia, severe obesity, small feet, and hypogonadism. However, while patients with PWS usually have moderate mental retardation and good communication skills, our patient presented severe mental retardation and absence of speech. In approximately 95% of PWS patients with a deletion, the distal breakpoint lies at15q13, between D15S1002 and D15S1048 (called BP3) [1,6]. However, in our patient , the breakpoint was at 15q14 (between the markers D15S1043 and D15S1010; called BP5). This distal breakpoint has not been previously described in PWS patients with a deletion, but it is found in most large inv dup(15) chromosomes [22], and in patients with intrachromosomal duplications or triplications of the PWS/AS region [21]. BP5 also contains parts of the genomic duplication derived from the HERC2 gene (duplicon) present in BP2 and BP3 [10], which are likely to be hotspots for recombination [21]. Amos-Landgraf et al. [1] suggested that the commonly occurring de novo rearrangements in the chromosome region 15q11-q13 might involve misalignment and recombination within these duplicons derived from the HERC2 gene. Unbalanced translocations have been reported involving the region 15q11-q13 and virtually all other chromosomes, with the exception of chromosomes 2, 4, 16, and 21 [3,9,20]. Here in we report an unbalanced translocation involving the segment 15q11-q14 and chromosome 4. The breakpoint in the terminal region of chromosome 4q was located in the subtelomeric region very close to the telomere. Although we cannot rule out the unbalance of the derivative chromosome 4 as another cause of the severely affected phenotype, patients with such a small putative deletion have not been reported, and associated clinical features are unknown. Moreover, Saccone et al. [18], who studied gene concentrations in the human genome through G+C gradient, and Pavlícek et al. [16], who analyzed GC level histograms M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 271 obtained after the draft human genome sequence, observed that 4qter was the subtelomeric region with the lowest gene concentration. Recently, cytogenetic and molecular characterizations of the breakpoints in chromosome segment 15q14 were published and correlated to the patients’ phenotypic features [20,14,23]. Smith et al. [20] reported a patient with severe mental retardation and absence of speech, with an unbalanced translocation t(15;22); the deleted segment on 22q did not include 22q13.3 and ARSA, but the distal non-specific pantelomeric probe was deleted. On 15q, the deletion extends beyond 15q13 to q14, but its precise localization was not determined. The severe PWS phenotype was mainly attributed to the terminal 22q deletion, although the presence of a larger deletion on 15q could not be ruled out. Matsumura et al. [14] described a patient with an unbalanced t(15;22) translocation [46,XY,-15,+der(22)t(15,22)(q14;q11)] ,who showed a severe PWS phenotype. The patient presented heart and renal failure, down-slanting palpebral fissures, a pre-auricular dimple, one malformed ear, micrognathia (characteristic features of patients with cat-eye syndrome), hypotonia, dolichocephaly, and small mouth with thin upper lip (characteristic features of PWS patients). This patient had also had intrauterine growth retardation. This severe PWS phenotype might be due to the partial trisomy 22q. Windpassinger et al. [23] reported a 2-year-old PWS patient with a deletion in the critical PWS region, as a result of an unbalanced t(3;15) translocation [45,XY,-15,der(3) t(3;15)(qter;q14)]. This patient presented additional features which are uncommon in PWS, including central visual impairment, macrocephaly, retrognathia, preauricular tags, and bilateral clubfoot. The authors attributed these characteristics to the largest deletion so far detected in the 15q region (between markers ACTC.PCR3 and D15S194) (Figure 3). Based on our results and on these three reports, we suggest that the severe mental retardation and absence of speech presented by our patient and by the patient described by Smith et al. [20] might be due to the larger extent of the paternal deletion on chromosome 15q, rather than to the derivative chromosomes (4 and 22) involved in the unbalanced translocations. Acknowledgements This work was supported by FAPESP (M.C.V. 99/10414-8), CEPID and CNPq. We thank Roseli M. Zanelato for technical assistance. References [1] [2] J.M. Amos-Landgraf,Y. Ji, W. Gottlieb, T. Depinet, A.E. Wandstrat, S.B. Cassidy, D.J. Driscoll, P.K. Rogan, S. Schwartz, R.D. Nicholls, Chromosome breakage in the Prader-Willi and Angelman syndromes involves recombination between large, transcribed repeats at proximal and distal breakpoints, Am J Hum Genet 65 (1999) 370–386. K. Buiting, S. Saitoh, S. Gross, B. Dittrich, S. Schwartz, R.D. Nicholls, B. Horsthemke, Inherited microdeletions in the Angelman and Prader-Willi syndromes define an imprinting center on human chromosome 15, Nature Genet 9 (1995) 395–400. 272 [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] [21] [22] M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 M.G. Butler, Prader-Willi syndrome: current understanding of cause and diagnosis, Am J Med Genet 35 (1990) 319–332. S.B. Cassidy, Prader-Willi syndrome, J Med Genet 34 (1997) 917–923. S.L. Christian, W.P.P. Robinson, B. Huang, A. Mutirangura, M.R. Line, M. Nakao, U. Surti, A. Chakravarti, D.H. Ledbetter, Molecular characterization of two proximal deletion breakpoint regions in both PraderWilli and Angelman syndrome patients, Am J Hum Genet 57 (1995) 40–48. S.L. Christian, J.A. Fantes, S.K. Mewborn, B. Huang, D.H. Ledbetter, Large genomic duplicons map to sites of instability in the Prader-Willi/Angelman syndrome chromosome region (15q11-q13), Hum Mol Genet 8 (1999) 1025–1037. C. Fridman, M.C. Varela, F. Kok, N. Setian, C.P. Koiffmann, Prader-Willi syndrome: genetic tests and clinical findings, Genetic Testing 4 (2000) 387–392. V.A. Holm, S.B. Cassidy, M.G. Butler, J.M. Hanchett, L.R. Greenswag, B.Y. Whitman, F. Greenberg, Prader-Willi syndrome: consensus diagnostic criteria, Pediatrics 91 (1993) 398–402. A. Jauch, L. Robson, A. Smith, Investigations with fluorescence in situ hybridization (FISH) demonstrate loss of the telomeres on the reciprocal chromosome in three unbalanced translocations involving chromosome 15 in the Prader-Willi and Angelman syndromes, Hum Genet 96 (1995) 345–349. Y. Ji, M.J. Walkowicz, K. Buiting, D.K. Johnson, R.E. Tarvin, E.M. Rinchik, B. Horsthemke, L. Stubbs, R.D. Nicholls, The ancestral gene for transcribed, low-copy repeats in Prader-Willi/Angelman region encodes a large protein implicated in protein traficking, which is deficient in mice with neuromuscular and spermiogenic abnormalities, Hum Mol Genet 3 (1999) 533–542. J.H.M. Knoll, R.D. Nicholls, R.E. Magenis, J.M. Graham Jr, M. Lalande, S.A. Latt, Angelman and Prader-Willi syndromes share a common chromosome 15 deletion, but differ in parental origin of the deletion, Am J Med Genet 32 (1989) 285–290. R.E. Magenis, S. Toth-Fejel, L.J. Allen, M. Black, M.G. Brown, S. Budden, R. Cohen, J.M. Friedman, D. Kalousek, J. Zonana, D. Lacy, S. LaFranchi, M. Lahr, J. Macfarlane, C.P.S. Williams, Comparison of the 15q deletions in Prader-Willi and Angelman syndromes: specific regions, extent of deletions, parental origin, and clinical consequences, Am J Med Genet 35 (1990) 333–349. M.J. Mascari, W. Gottlieb, P.K. Rogan, M.G. Butler, D.A. Waller, J.A.L. Armour, A.J. Jeffreys, R.L. Ladda, R.D. Nicholls, The frequency of uniparental disomy in Prader-Willi syndrome, N Engl J Med 326 (1992) 1599–1607. M. Matsumura, T. Kubota, E. Hidata, K. Wakui, S. Kadowaki, I. Ueta, T. Shimizu, I. Ueno, K. Yamauchi, L.B. Herzing, E.L. Nurmi, J.S. Sutcliffe, F. Fukushima, T. Katsuyama, ‘Severe’ Prader-Willi syndrome with a large deletion of chromosome 15 due to an unbalanced t(15,22)(q14;q11.2) translocation, Clin Genet 63 (2003) 79–81. R.D. Nicholls, J.L. Knepper, Genome organization, function, and imprinting in Prader-Willi and Angelman syndromes, Annu Rev Genomics Hum Genet 2 (2001) 153–175. A. Pavlícek, J. Paces, O. Clay, G. Bernardi, A compact view of isochores in the draft human genome sequence, FEBS Letters 511 (2002) 165–169. A. Prader, A. Labhart, H. Willi, Ein Syndrom von Adipositas, Kleinwuchs, Kryptochismus und Oligophrenie nach myotonieartigem Zustand im Neugeborenenalter, Schweiz Med Wochenschr 86 (1956) 1260– 1261. S. Saccone, S. Cacciò, J. Kusuda, A. Andreozzi, G. Bernardi, Identification of gene-richest bands in human chromosomes, Gene 174 (1996) 85–94. A. Smith, L. Robson, A. Neumann, M. Mulcahy, V. Chabros, Z.-M. Deng, T. Woodage, R.J. Trent, Fluorescence in situ hybridization and molecular studies used in the characterization of a Robertsonian translocation (13q15q) in Prader-Willi syndrome, Clin Genet 43 (1993) 5–8. A. Smith, A. Jauch, L.S. Heaps, L. Robson, B. Kearney, Unbalanced translocation t(15;22) in “severe” Prader-Willi syndrome, Ann Gènèt 43 (2000) 125–130. P. Ungaro, S.L. Christian, J.A. Fantes, A. Mutirangura, S. Balck, J. Reynolds, S. Malcolm, W.B. Dobyns, D.H. Ledbetter, Molecular characterization of four cases of intrachromosomal triplication of chromosome 15q11-q14, J Med Genet 38 (2001) 26–34. A.E. Wandstrat, J. Leana-Cox, L. Jenkins, S. Schwartz, Molecular cytogenetic evidence for a common breakpoint in the largest inverted duplications of chromosome 15, Am J Hum Genet 62 (1998) 925–936. M.C. Varela et al. / Annales de Génétique 47 (2004) 267–273 273 [23] C. Windpassinger, E. Petek, K. Wagner, A. Langman, K. Buiting, P.M. Kroisel, Molecular characterization of a unique de novo 15q deletion associated with Prader-Willi syndrome and central visual impairment, Clin Genet 63 (2003) 297–302. [24] M. Zeschnigk, C. Lich, K. Buiting, W. Doerfler, B. Horsthemke, A single tube PCR test for the diagnosis of Angelman and Prader-Willi syndrome based on allelic methylation differences at the SNRPN locus, Eur J Hum Genet 5 (1997) 94–98.